
To assess the functional results of intertrochanteric fractures treated with the short PFNA2 were assessed using the Modified Harris Hip Score, with fracture reduction and fixation evaluated based on the neck–shaft angle and tip–apex index.
Dr. K V Prem Kumar, Department of Orthopaedics, Chettinad Hospital and Research Institute, Chettinad Academy of Research and Education, Kelambakkam, Chengalpattu - 603 103, Tamil Nadu, India. E-mail: drpremkumar.kvk@gmail.com
Introduction: Intertrochanteric fractures are among the most common fractures in elderly patients, often associated with osteoporosis and high morbidity. Surgical fixation is the preferred treatment approach to enable early mobilization and reduce complications. The Short Proximal Femoral Nail Anti-Rotation-2 (PFNA-2) has emerged as an effective implant for these fractures, offering improved stability, enhanced biomechanical properties, and reduced risk of implant failure. This study aims to evaluate the functional and radiological outcomes of PFNA-2 in the management of intertrochanteric fractures.
Materials and Methods: This prospective study was conducted at the Department of Orthopaedics, Chettinad Health Institute, Tamil Nadu, involving 50 patients with Boyd and Griffin Type 1–4 intertrochanteric fractures. Functional outcomes were assessed using the Modified Harris Hip Score (MHHS), while radiological outcomes were evaluated based on fracture union time, neck–shaft angle, and tip–apex distance (TAD). Patients were followed for a minimum of 6 months postoperatively, with serial radiographic assessments conducted at 6, 12, and 24 weeks. Post-operative rehabilitation included early mobilization, pain management, and weight-bearing exercises to optimize recovery.
Results: The mean age of the study population was 69.04 ± 10.69 years, with a slight female predominance (52%). The mean MHHS was 83.08 ± 8.005, with 44% of patients categorized as having good outcomes and 26% classified as excellent. Younger patients demonstrated significantly better functional outcomes (P = 0.000). The mean neck–shaft angle was 130.6° ± 2.1°, with no significant variation across demographic groups (P = 0.191). The mean TAD was 18.25 ± 4.89 mm, with 12% of patients having a TAD >25 mm. Post-operative complications were minimal, with screw cut-out occurring in 4% of cases and superficial wound healing delays in 2%.
Conclusion: The findings suggest that PFNA-2 provides effective fixation and favorable functional outcomes in intertrochanteric fractures, particularly in elderly patients. With minimal complications and early mobilization benefits, PFNA-2 proves to be a reliable implant for optimizing recovery. Future studies with larger cohorts and longer follow-ups are recommended to validate these findings.
Keywords: Intertrochanteric fractures, proximal femoral nail, Harris Hip Score.
Intertrochanteric and per-trochanteric fractures are among the most common traumatic injuries in individuals over 60 years of age. These fractures, which occur outside the hip joint capsule, typically involve the proximal femur between the greater and lesser trochanters and may occasionally extend into the subtrochanteric region. Their incidence increases significantly with age and poses substantial challenges to healthcare systems due to the complexity of management and the frequent presence of comorbidities such as osteoporosis, diabetes, hypertension, and renal insufficiency. These fractures lead to considerable declines in mobility and independence in older adults, with many patients requiring assistance for daily activities. While non-operative management may be considered for patients with minimal pain or limited ambulatory status, surgical intervention is generally preferred as it provides more reliable fixation and facilitates early mobilization. Despite advancements in surgical techniques and implant designs, managing intertrochanteric fractures remains challenging, particularly in osteoporotic elderly patients. The cancellous nature of such bone makes achieving stable fixation difficult, as it is less robust and more prone to failure under internal fixation forces. Several factors influence successful fixation, including bone quality, fracture stability, anatomical alignment, reduction quality, implant design, and placement accuracy. Among these, surgeons have significant control over implant selection and placement. While devices such as the dynamic hip screw have been widely used for years, they may not be ideal for elderly patients with osteoporosis, as complications like screw cut-out are more common in this group. The Short Proximal Femoral Nail Anti-Rotation II (PFNA-2) has emerged as a promising alternative for managing stable intertrochanteric fractures, particularly in elderly patients. Unlike traditional lag screws, the PFNA-2 incorporates a helical blade designed to provide superior rotational stability and promote bone compaction at the femoral neck, resulting in stronger fixation. This design significantly reduces complications such as screw cut-out. An important modification in the PFNA-2 is the reduction of the mediolateral angle from 6° in earlier models to 5°, which enhances the implant’s stability, particularly in osteoporotic bone. Additionally, the implant is designed to facilitate early post-operative mobilization, accelerate fracture healing, and reduce the risks of complications such as implant failure, medial penetration, or back-out of the helical blade. Although the short PFNA-2 has shown encouraging results in improving functional outcomes, its overall effectiveness and clinical benefits are not yet fully established. This is particularly true for unstable fractures, where comparative studies remain limited. Addressing these gaps is crucial to optimizing treatment strategies, especially in elderly patients with compromised bone quality. This study is to evaluate the functional and radiological outcomes in short PFNA-2 in treating intertrochanteric fractures in elderly patients. The functional outcomes will be assessed using the Harris Hip Score (HHS), focusing on pain levels, functional ability, absence of deformity, and range of motion. Radiological outcomes will include the time to fracture union and the quality of fracture reduction and fixation as assessed through radiographic imaging. By examining these parameters, this study seeks to provide robust evidence supporting the use of PFNA-2, contributing to improved treatment strategies and patient outcomes in this clinical context.
This study was done in the Department of Orthopaedics, Chettinad Health Institute, Kelambakkam, Tamil Nadu, and included 50 patients with stable intertrochanteric fractures. Participants were followed for a minimum period of 6 months after undergoing surgical intervention. Inclusion criteria comprised individuals over the age of 18 years with Boyd and Griffin Type 1–4 intertrochanteric fractures who were ambulatory prior to the fracture. Patients with significant comorbidities that rendered them unfit for surgery, open fractures, local infections at the fracture site, pre-existing hip conditions such as osteoarthritis or avascular necrosis, multiple fractures, or those who declined surgical treatment were not included in the study. Written informed consent was obtained from all participants and their data were collected prospectively using a standardized pro forma that included demographic, clinical, and radiological details. The study assessed both functional with radiological outcomes of fractures managed with the short PFNA-2. Functional outcomes were evaluated using the HHS, which included assessments of pain, mobility, absence of deformity, and range of motion. Radiological outcomes were assessed by monitoring the time required for fracture union using serial radiographs taken at intervals of 6, 12, and 24 weeks postoperatively. Additional parameters evaluated included the quality of fracture reduction, determined by comparing the neck–shaft angle with the contralateral normal hip, and the quality of fixation using the tip–apex index, which measures the placement and stability of the implant. Post-operative care was focused on early mobilization and rehabilitation to improve recovery and minimize complications. On the 1st post-operative day, the patients were to be encouraged to begin mobilizing and bear weight as tolerated based on the surgeon’s recommendations. A structured rehabilitation protocol was followed, including chest exercises, joint mobilization, and gradual weight-bearing exercises. Pain management, deep venous thrombosis prophylaxis with pharmacological and mechanical methods, and follow-up radiographic imaging were integral components of post-operative care. Sutures were removed approximately 12 days post-surgery, and follow-ups were scheduled at 3 and 6 months to assess both clinical and radiological outcomes. The study aims in evaluating the effectiveness of the PFNA-2 implant in managing intertrochanteric fractures, particularly in elderly osteoporotic patients. The data collected were analyzed to determine the functional improvements based on HHS scores and the radiological success of the implant. By assessing parameters such as fracture union time, implant stability, and reduction quality, the study sought to establish the clinical utility and reliability of the PFNA-2 in providing optimal outcomes for this patient population.
A total of 50 patients were included in this study. Table 1 shows the distribution of pre-operative patients’ characteristics. The mean age of the patients in this study was 69.04 ± 10.69. A majority of patients were in the 60–74-year age group, with more female predominance. Right seems to be more common than left side. In terms of fracture severity, Boyd and Griffin Type 2 fractures were the most frequent, followed by Type 1.

Table 2 summarizes the intraoperative details of the study participants. The mean operation time was 66.4 min with a standard deviation of 5.1 min, ranging from 60 to 75 min. The mean blood loss was 99 mL with a standard deviation of 6.2 mL, ranging from 90 to 110 mL.

Post-operative assessment
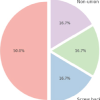
Table 3 summarizes the distribution of Modified HHS (MHHS) among these study participants. The MHHS among study participants revealed significant variations with age, while differences based on sex and Boyd and Griffin classification were not statistically significant. Participants aged <60 years had the highest mean score (88.2 ± 4.1), followed by those aged 60–74 years (85 ± 7.4) and >75 years (76.5 ± 6.9), with significant P = 0.000. Males had a slightly higher mean score (83.87 ± 8.023) compared to females (82.35 ± 8.074), and the P value was 0.505. Among Boyd and Griffin classification types, Type 3 fractures had the highest mean score (85.50 ± 6.172), while Type 4 had the lowest (80.86 ± 6.669), with P = 0.548. Fig. 1 shows the distribution of patients based on the MHHS where 26% had an excellent score and 44% had a good score. Overall, the total mean of MHHS was 83.08 ± 8.005. Fig. 2 shows pre-operative X-rays (a and b) and immediate post-operative (c and d) X-ray findings.


The distribution in neck–shaft angle among study participants had no statistically significant differences across age, sex, or Boyd and Griffin classification groups (Table 4). Participants aged >75 years had the highest mean angle (130.9° ± 2.5°), followed closely by those aged 60–74 years (130.8° ± 1.8°) and <60 years (129.5° ± 2.0°), with P = 0.191. Males and females had identical mean neck–shaft angles (130.6°), with standard deviations of 1.9° and 2.2°, respectively, and P = 0.991. Among Boyd and Griffin classification types, Types 2 and 3 had the highest mean angles (130.8° ± 2.5° and 130.8° ± 1.8°, respectively), while Types 1 and 4 had slightly lower means (130.3° ± 2.2° and 130.3° ± 1.4°, respectively), with P = 0.875. The overall mean neck–shaft angle was 130.6° ± 2.1°. Fig. 3 shows the follow-up X-rays taken at the 3rd month (a and b), 6th month (c and d), and after 1 year (e and f).


The analysis of tip–apex distance (TAD) among study participants did not show statistically significant differences by age, sex, or Boyd and Griffin classification (Table 5). The overall mean TAD in this study was 18.25 ± 4.89 mm, with 12% of participants having a TAD >25 mm. Participants aged >75 years had the highest mean TAD (19.47 ± 5.44 mm), followed by those aged 60–74 years (18.14 ± 5.18 mm) and <60 years (16.67 ± 2.66 mm), though the differences were not statistically significant (P = 0.376). Females had a slightly higher mean TAD (18.63 ± 5.96 mm) compared to males (17.83 ± 3.44 mm). Among Boyd and Griffin classifications, Type 3 and Type 4 fractures showed higher mean TAD values (19.36 ± 5.00 mm and 19.33 ± 6.87 mm, respectively). Fig. 4 shows the X-rays of one of the patients displaying the tip–apex index (a and b).


Table 6 shows the distribution of post-operative complications among the study participants. In this study, post-operative complications were minimal. Screw cut-out occurred in 4% of patients (2 patients), while negative cortical support, positive medial cortical support, and delayed superficial wound healing were each observed in 2% of cases (1 patient each) Fig. 5 shows the clinical photograph of a patient during follow-up, demonstrating a restored range of motion and functional recovery after surgical management.

Intertrochanteric fractures seem to be among the most common fractures in the elderly, often resulting from low-energy falls in osteoporotic bone. The management of these fractures poses significant challenges, especially in ensuring optimal functional and radiological outcomes [1]. The short PFNA-2 has emerged as a reliable implant for these fractures, offering biomechanical stability and minimally invasive application. In this study, we evaluated the functional and radiological outcomes of PFNA-2, focusing on parameters such as fracture reduction quality, implant positioning, and post-operative recovery. Fifty patients totally were included in this study, and the results are discussed in detail below. Intertrochanteric fractures are predominantly observed in the elderly population, primarily due to age-related declines in bone density and increased susceptibility to falls. In our study, the mean age in patients was 69.04 ± 10.69 years, majority falling within the 60–74-year age group, a finding consistent with global trends. Hedlund and Lindgren [2] previously identified age as a dominant risk factor for proximal femoral fractures regardless of the cause of injury. Age-associated factors such as osteoporosis, diminished muscle strength, and impaired balance are critical contributors to the incidence of these fractures. Moreover, advancing age often complicates post-operative recovery due to the presence of comorbidities that may delay fracture healing and impact functional outcomes. These observations underscore the importance of age-specific strategies in preventing and managing intertrochanteric fractures. The predominance of female patients in our study aligns with existing literature on intertrochanteric fractures, which consistently highlights a higher incidence among women. This increased vulnerability in females is largely attributed to post-menopausal osteoporosis, where decreased estrogen levels lead to accelerated bone loss and reduced bone mineral density. Additionally, women tend to have longer lifespans than men, which increases their likelihood of sustaining low-energy fractures, such as intertrochanteric fractures, at older ages. Studies have also indicated that certain anatomical and biomechanical factors, such as wider pelvic structure and lower muscle mass in females, may further contribute to this predisposition [3]. The Boyd and Griffin classification provides a structured framework for categorizing intertrochanteric fractures based on fracture patterns, which can influence surgical planning and outcomes. In our study, Type 2 fractures were the most prevalent (34.0%), followed by Type 1 (28.0%), Type 3 (24.0%), and Type 4 (14.0%). The predominance of Type 2 fractures aligns with existing data [4,5] that suggest this type often results from low-energy trauma in osteoporotic bone, which is common in elderly populations. Type 1 and 3 fractures, while less frequent, are relatively stable and easier to manage surgically, whereas Type 4 fractures, being comminuted and unstable, pose greater challenges in achieving optimal reduction and fixation. The mean post-operative neck–shaft angle of 130.6° ± 2.1° observed in this study is consistent with the desired anatomical restoration aimed for during surgical fixation of intertrochanteric fractures. Maintaining an optimal neck–shaft angle is crucial as it directly impacts the biomechanics of the hip joint, ensuring appropriate load distribution and functional recovery. Deviations from the normal range (approximately 125°–135°) may result in complications such as varus malalignment, implant failure, or altered gait mechanics. The minimal variation in the post-operative angle reflects the precision achieved in fracture reduction and fixation techniques. The MHHS is a reliable tool for evaluating post-operative outcomes in patients undergoing surgical management of hip fractures, particularly intertrochanteric fractures [6]. It assesses pain and functional capacity across domains such as mobility, gait, and daily activity performance, providing a robust measure of recovery. In this study, the total mean MHHS was 83.08 ± 8.005 (44% good and 26% excellent) indicating favorable post-operative outcomes with effective surgical management and rehabilitation. This score aligns with good functional recovery, reduced pain, and restored mobility. Similar findings were reported by Sharma et al., [7] where the mean MHHS was 78.85, with 36% of patients categorized as having “good” outcomes and 13% classified as “excellent.” Additionally, Kassem et al. [8] observed a mean HHS of 80.4 ± 8.7 after 12 months of proximal femoral nailing for unstable intertrochanteric fractures. The slightly higher mean score in the current study suggests that PFNA-2 may provide marginally better functional outcomes, potentially due to enhanced biomechanical stability or reduced post-operative complications. However, differences in patient demographics, fracture patterns, rehabilitation protocols, and scoring systems (Modified vs. Original HHS) might account for this variation. These findings underline the need for further comparative research to establish the advantages of PFNA-2 over PFN. The MHHS in this study demonstrated significant variability across age groups, highlighting the impact of age on post-operative outcomes. Participants under 60 years achieved the highest mean score (88.2 ± 4.1), reflecting superior recovery likely due to better bone quality, muscle strength, and fewer comorbidities. The 60–74-year age group scored moderately well (85 ± 7.4), while those over 75 years had the lowest mean score (76.5 ± 6.9), indicative of challenges such as osteoporosis, frailty, and higher comorbidity burden in older patients. The significant P-value (0.000) underscores age as a critical factor influencing functional recovery, emphasizing rehabilitation in age-specific and strategical care to optimize outcomes in elderly patients. This finding aligns with existing literature [9], which consistently identifies age as a major predictor of outcomes in hip fracture management. Although there was variation in TAD between different age groups, sex, and Boyd and Griffin classification, they were not statistically significant. The overall mean TAD was 18.25 ± 4.89 mm. Additionally, 12% of participants with a TAD >25 mm underscore a subgroup at higher risk for complications, as studies [10,11] have shown that a >25 mm TAD is associated with increased implant failure rates. In this study, post-operative complications were minimal. Screw cut-out occurred in 4% of patients (2 patients), while negative cortical support, positive medial cortical support, and delayed superficial wound healing were each observed in 2% of cases (1 patient each).Medial migration or penetration of the helical blade, loss of reduction in unstable fractures, and periprosthetic fractures are major concerns in the treatment of proximal femoral fractures, particularly with devices such as PFNA-2. These complications typically result from factors such as improper placement of the helical blade, compromised bone quality, and suboptimal surgical techniques, potentially leading to serious outcomes such as joint damage, persistent pain, or the need for revision surgery. Furthermore, loss of reduction and periprosthetic fractures can hinder recovery and slow rehabilitation, especially in elderly or osteoporotic patients. These challenges emphasize the importance of thorough surgical planning, careful implant selection, and diligent post-operative care. Continuous research is crucial to advance implant designs, enhance surgical techniques, and identify at-risk patients, ultimately minimizing complications and improving long-term outcomes. Tackling these issues will help increase the success of femoral fracture treatments and improve patients’ quality of life. There were no major complications such as implant failure, deep infections, or reoperation requirements. All patients showed good functional outcomes, demonstrating the effectiveness and safety of PFNA-2 in treating intertrochanteric fractures. The implant provided stable fixation and supported recovery with minimal complications.
Limitations
The study seemed to have several limitations, including quite relatively small sample size, which may have affected the generalizability of the results. The follow-up period was relatively short, potentially missing long-term complications or functional changes. Additionally, being a single-center study, the findings may not reflect variations across different settings or patient demographics. Selection bias could also have influenced the results, as certain groups, such as those with severe comorbidities, may have been excluded. Finally, while the MHHS is one of the best-established tools, it may not capture all aspects of functional recovery or quality of life, limiting the comprehensiveness of the outcome assessment.
The study demonstrates that the use of the short PFNA-2 in intertrochanteric fractures provides favorable post-operative outcomes, as reflected by a mean MHHS of 83.08 ± 8.005 and an overall mean TAD of 11.74 ± 7.03 mm. These results indicate effective surgical fixation and functional recovery. The findings also highlight the influence of age, fracture classification, and surgical technique on outcomes, emphasizing the need for individualized management strategies. Future multicenter studies with a greater number of sample sizes along with longer follow-up periods are to be recommended to validate the above findings and explore their applicability in diverse patient populations.
Intertrochanteric fractures are frequently seen in elderly individuals with osteoporosis, often accompanied by other comorbid conditions. The short PFNA-2 is a more appropriate choice for these patients as it involves a shorter surgical time and reduced blood loss. With short PFNA-2 fixation, only proximal reaming is required, eliminating the need for serial reaming of the medullary canal and consequently lowering the risk of embolism. Furthermore, for elderly patients with subtrochanteric fractures and significant anterior bowing of the femur, the Short PFNA-2 is a viable alternative to the long PFNA-2.
References
- 1.Broderick JM, Bruce-Brand R, Stanley E, Mulhall KJ. Osteoporotic hip fractures: The burden of fixation failure. ScientificWorldJournal 2013;2013:515197. [Google Scholar | PubMed]
- 2.Hedlund R, Lindgren U. Trauma type, age, and gender as determinants of hip fracture. J Orthop Res 1987;5:242-6. [Google Scholar | PubMed]
- 3.Rathbun AM, Shardell M, Orwig D, Hebel JR, Hicks GE, Beck TJ, et al. Difference in the trajectory of change in bone geometry as measured by hip structural analysis in the narrow neck, intertrochanteric region, and femoral shaft between men and women following hip fracture. Bone 2016;92:124-31. [Google Scholar | PubMed]
- 4.Kumar R, Ranjan R, Jeyaraman M, Chaudhary D. Clinico-radiological and functional outcome of intertrochanteric fractures by dynamic hip screw. Nat J Clin Orthop 2020;4:19-22. [Google Scholar | PubMed]
- 5.Naganur R, Basavaraddi BR. Clinical profile of patients with intertrochanteric fracture of femur. Int J Orthop Sci 2019;5:726-8. [Google Scholar | PubMed]
- 6.Harold RE, Butler BA, Delagrammaticas D, Sullivan R, Stover M, Manning DW. Patient-reported outcomes measurement information system correlates with modified harris hip score in total hip arthroplasty. Orthopedics 2020;44:e19-25. [Google Scholar | PubMed]
- 7.Sharma A, Mahajan A, John B. A comparison of the clinico-radiological outcomes with proximal femoral nail (PFN) and proximal femoral nail antirotation (PFNA) in fixation of unstable intertrochanteric fractures. J Clin Diagn Res 2017;11:RC05-9. [Google Scholar | PubMed]
- 8.Kassem E, Younan R, Abaskhron M, Abo-Elsoud M. Functional and radiological outcomes of dynamic hip screw with trochanteric stabilizing plate versus short proximal femoral nail in management of unstable trochanteric fractures: A randomized-controlled trial. Jt Dis Relat Surg 2022;33:531-7. [Google Scholar | PubMed]
- 9.Xu BY, Yan S, Low LL, Vasanwala FF, Low SG. Predictors of poor functional outcomes and mortality in patients with hip fracture: A systematic review. BMC Musculoskelet Disord 2019;20:568. [Google Scholar | PubMed]
- 10.Sahu B, Prusty A, Tudu B. Tip apex distance - is it enough to predict implant failure in trochanteric fractures. Indian J Orthop Surg 2017;3:386-8. [Google Scholar | PubMed]
- 11.Geller JA, Saifi C, Morrison TA, Macaulay W. Tip-apex distance of intramedullary devices as a predictor of cut-out failure in the treatment of peritrochanteric elderly hip fractures. Int Orthop 2010;34:719-22. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Functional and Radiological Outcomes of Proximal Femoral Nailing in Unstable Peritrochanteric Fractures: A Prospective Observational Study
February 1, 2026 Functional and Radiological Outcomes of Proximal Femoral Nailing in Unstable Peritrochanteric Fractures: A Prospective Observational Study March 1, 2025 Evaluation of Functional and Radiological Outcome of Different Cephalomedullary Nail Designs in Intertrochanteric Fractures of Femur
March 1, 2025 Evaluation of Functional and Radiological Outcome of Different Cephalomedullary Nail Designs in Intertrochanteric Fractures of Femur April 1, 2026 Functional Outcome of Unstable Intertrochanteric Femur Fracture Treated Surgically With Long Proximal Femoral Nail
April 1, 2026 Functional Outcome of Unstable Intertrochanteric Femur Fracture Treated Surgically With Long Proximal Femoral Nail March 1, 2026 Comparison of Cemented Versus Cementless Total Hip Arthroplasty in Elderly Patients: A Prospective Cohort Study
March 1, 2026 Comparison of Cemented Versus Cementless Total Hip Arthroplasty in Elderly Patients: A Prospective Cohort Study