
Mastering the management of bilateral Kohler’s disease for improved patient outcomes.
Dr. Ibrahim Deniz Canbeyli, Department of Orthopedics and Traumatology, Kırıkkale University, Kırıkkale Universitesi Kampusu Ankara Yolu 7. Km. Yahsihan, Kırıkkale, Türkiye. E-mail: denizcanbeyli@gmail.com
Introduction: Köhler’s disease is a self-limiting disorder affecting endochondral ossification, marked by fragmentation and sclerosis in the tarsal navicular bone. In 1908, Köhler highlighted these complexities by describing concurrent osteochondrosis of the tarsal navicular.
Case Report: A relevant case involves a 5-year-old girl who visited an orthopedic clinic with bilateral foot pain and an inability to bear weight for a week. She was diagnosed with bilateral Köhler’s disease.
Conclusion: Although uncommon, Köhler’s disease should be considered in the differential diagnosis of pediatric foot pain to avoid unnecessary treatments and to ensure optimal care for the patients.
Keywords: Kohler’s disease, avascular necrosis, pediatric foot pain, navicular bone.
Osteochondroses represent self-limiting disorders of endochondral ossification, marked by radiological fragmentation and sclerosis of the affected bone [1]. In 1908, Köhler made an important contribution to this field by reporting on the concurrent osteochondrosis of the tarsal navicular, shedding light on the complexities of these conditions [2]. Kohler disease, which occurs 3–5 times more frequently in boys than in girls, has been documented in the medical literature [1,3]. It is important to note that up to 25% of cases can affect bilateral tarsal navicular bones [4]. Our case report appears to be the first published instance of bilateral Kohler disease in a girl since the landmark case in 1930.
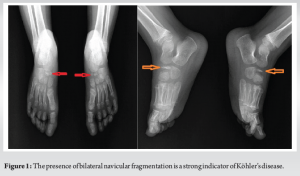
A 5-year-old girl applied to the outpatient clinic with concerning complaints of bilateral foot pain that began after sports activities and worsened throughout the day over the past week. Importantly, her pain in the right foot was significantly more intense than that in her left foot. She exhibited an antalgic gait, suggesting discomfort in her right lower extremity, and her father noted that she was pressing on the outer part of her right sole while walking. During the physical examination, tenderness was noted over the navicular bones of both feet. The pain in her right foot was rated as 7, while the left foot was rated as 4 on the visual analog scale (VAS). Radiological assessment revealed irregular sclerosis and increased density, indicating Köhler’s Disease in both navicular bones (Fig. 1). The talus, calcaneus, cuneiforms, and all other tarsal and metatarsal bones appeared normal in the radiological assessment.
A short leg splint was applied to her more affected right lower extremity for a period of 3 weeks. Regular follow-up appointments at the Orthopedics and Traumatology outpatient clinic were advised every week to ensure comprehensive care and monitoring of her progress. The patient was instructed to avoid weight-bearing activities and to take ibuprofen at a dosage of 10 mg/kg as needed for pain relief. At the 1-month follow-up, the patient confidently reported a pain level of only 1–2 on the VAS on her right side, with no pain at all on the left side. Additionally, the family mentioned that the patient was significantly better at mobilizing compared to 1 month prior, demonstrating clear improvement in her overall condition. In addition, at the 1st year follow-up, the patient’s complaints had completely regressed. Improvement was also detected on the follow-up radiograph (Fig. 2).

Köhler’s bone disease is an uncommon yet significant condition characterized by self-limited osteochondrosis affecting the tarsal navicular bone [1]. While the etiology of this disease remains elusive, it is marked by notable disruptions in endochondral ossification processes, which encompass both chondrogenesis and osteogenesis [3]. The diagnosis of Köhler’s disease is primarily based on clinical signs, notably pain and tenderness in the dorsal aspect of the midfoot. Examination reveals key tenderness in the tarsal navicular area, often coinciding with mild swelling over the midfoot [3]. Crucially, all laboratory tests may be normal, and most individuals lack a history of prior infections or any injuries that could clarify the onset of the condition. A radiographic examination of the foot and ankle often reveals characteristic features of necrosis, such as increased radiodensity, fragmentation, and flattening along the navicular bone’s longitudinal axis [5,6]. Recognizing these symptoms early can lead to timely intervention and better outcomes. Patients who received a cast experienced complete resolution of their symptoms in just 3 months, which is significantly faster than those without a cast, who took 10 months to resolve their symptoms. The prognosis for all patients is exceptionally promising, as nearly everyone achieves full restoration of bone structure within a period of 4 months–4 years [2,7]. Given these insights, it is vital to prioritize symptomatic treatment, as surgical solutions are not practical. To date, there have been just three published reports of bilateral cases. The first was a case involving a 6-year-old girl, reported by Wakeley CP in 1930, which is the only case of a girl with bilateral Kohler disease in literature [8]. In 2003, Tsirikos et al. [3] documented bilateral Kohler disease in 8-year-old male twins who presented to the outpatient clinic, similar to our patient with an antalgic gait and diffuse swelling on the anterior aspect of the foot, along with tenderness over the anterior part of the ankle joint. Most recently, in 2023, Deshpande et al. [9] reported a case of bilateral Kohler disease in a 6-year-old boy who applied to the outpatient clinic in a chair. He also had an antalgic gait and diffuse swelling on the anterior aspect of the ankle joint, mirroring the symptoms of our patient. When addressing Kohler’s disease, a non-surgical approach is often effective in a significant number of cases [9]. Fortunately, this condition is generally self-limiting [2]. For managing pain, symptomatic treatments such as non-steroidal anti-inflammatory drugs can be highly beneficial, alongside rest to minimize weight-bearing activities [2,9]. In addition, employing a short leg cast for approximately 6 weeks can provide crucial support. These combined measures can significantly enhance recovery and improve quality of life. We achieved high levels of patient satisfaction with our symptomatic treatment and the application of a short leg cast, in accordance with existing literature [10]. This demonstrates our commitment to providing high-quality care through conservative methods that meet our patients’ needs.
Kohler’s Disease is a generally benign condition that often resolves on its own, though it can cause significant pain and limping in children. While it is a rare diagnosis, it is crucial for physicians to consider it, particularly when a child presents with pain in the dorsal area of the foot. Timely recognition of Kohler’s Disease can not only alleviate unnecessary suffering but also help avoid additional tests and treatments that may not be needed. The prognosis for this condition is generally favorable, as almost all patients achieve complete restoration of bone structure without requiring any surgical intervention.
Bilateral foot pain in a child may indicate Kohler’s disease, which should be considered in the differential diagnosis.
References
- 1.Ippolito E, Ricciardi Pollini PT, Falez F. Kohler’s disease of the tarsal navicular: Long-term follow-up of 12 cases. J Pediatr Orthop 1984;4:416-7. [Google Scholar | PubMed]
- 2.Alhamdani M, Kelly C. Kohler’s disease presenting as acute foot injury. Am J Emerg Med 2017;35:1787.e5-6. [Google Scholar | PubMed]
- 3.Tsirikos AI, Riddle EC, Kruse R. Bilateral Kohler’s disease in identical twins. Clin Orthop Relat Res 2003;409:195-8. [Google Scholar | PubMed]
- 4.Trammell AP, Davis DD, Scott A. Kohler disease. In: StatPearls. Treasure Island, FL: StatPearls; 2024. [Google Scholar | PubMed]
- 5.Williams GA, Cowell HR. Kohler’s disease of the tarsal navicular. Clin Orthop Relat Res 1981;158:53-8. [Google Scholar | PubMed]
- 6.Santos L, Estanqueiro P, Matos G, Salgado M. Kohler disease: An infrequent or underdiagnosed cause of child’s limping? Acta Reumatol Port 2015;40:304-5. [Google Scholar | PubMed]
- 7.Borges JL, Guille JT, Bowen JR. Kohler’s bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-8. [Google Scholar | PubMed]
- 8.Wakeley CP. Bilateral Kohler’s disease. Proc R Soc Med 1930;23:826. [Google Scholar | PubMed]
- 9.Deshpande SV, Channawar RA, Wamborikar H, Patil B, Pundkar A. Bilateral Kohler’s disease: A case report. Cureus 2023;15:e44929. [Google Scholar | PubMed]
- 10.DiGiovanni CW, Patel A, Calfee R, Nickisch F. Osteonecrosis in the foot. J Am Acad Orthop Surg 2007;15:208-17. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Early Outcomes of Screwless Press-fit Acetabular Cups in Uncemented Total Hip Arthroplasty: A Prospective Study from Eastern India
January 1, 2026 Early Outcomes of Screwless Press-fit Acetabular Cups in Uncemented Total Hip Arthroplasty: A Prospective Study from Eastern India December 1, 2025 Retrieval of a Sunken Interference Screw during Core Decompression and Autologous Adult Live-cultured Osteoblast Injection for Bilateral Hip Avascular Necrosis: A Case Report
December 1, 2025 Retrieval of a Sunken Interference Screw during Core Decompression and Autologous Adult Live-cultured Osteoblast Injection for Bilateral Hip Avascular Necrosis: A Case Report December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System October 1, 2025 Bilateral Traumatic Scaphoid Fracture Managed Surgically with Headless Compression Screw: A Case Report with Review Literature
October 1, 2025 Bilateral Traumatic Scaphoid Fracture Managed Surgically with Headless Compression Screw: A Case Report with Review Literature