
This case report proves the efficacy of the Lower Trapezius Tendon Transfer technique in managing Irreparable Isolated Infraspinatus Musculotendinous Lesion. Key benefits include pain relief and active external rotation restoration.
Dr. Jean Kany, Clinique de l’Union, Saint Jean, Toulouse, France, Boulevard De Ratalens, 31240 Saint Jean, France. E-mail: jean.kany@icloud.com
Introduction: Irreparable isolated musculotendinous lesions of the infraspinatus are infrequently reported, yet they significantly impair shoulder function. These lesions are characterized by rapid architectural changes in the infraspinatus, with advanced atrophy and high fatty infiltration, rendering treatment particularly challenging. With its biomechanical and anatomical advantages over conventional latissimus dorsi transfer in external rotation, lower trapezius tendon transfer has demonstrated promising clinical outcomes in cases of posterior-superior irreparable rotator cuff tears.
Case Report: A case report of two patients (A 57-year-old female and a 66-year- old male) with irreparable isolated musculotendinous lesion in the infraspinatus who underwent lower trapezius tendon transfer.
Conclusion: Lower trapezius transfer effectively alleviated pain and restored active external rotation in both patients, in contrast to attempts of direct repair or augmentation with allografts previously described in the literature.
Level of evidence: Case report
Keywords: Musculotendinous lesion, infraspinatus, lower trapezius transfer, arthroscopy.
Isolated musculotendinous lesions in the infraspinatus are rare conditions, infrequently reported since their initial description by Tavernier et al. in 2006 [1]. The diagnosis requires the absence of concomitant tears in the other rotator cuff tendons, including the subscapularis, supraspinatus, and teres minor, rendering this incidence extremely rare. The natural progression of these lesion occurs in two phases: an early stage characterized by muscle edema and a late stage marked by progression to fatty infiltration (Goutallier [2] grade ≥ III), resulting in shoulder pain and weakness in active external rotation [1,3,4]. Attempts at direct repair of the infraspinatus and lateral repair between the supraspinatus and teres minor have been made, but they were unsuccessful in halting the progression to fatty infiltration of the infraspinatus. Based on the results after trying surgical repair for this condition, it was discontinued by the first authors in 2008 [3]. A subsequent review in 2009 found no significant difference in the post-operative Constant score between the operated and non-operated groups (P = 0.325) [4]. To our knowledge, no effective treatment for this condition has been reported, and isolated musculotendinous lesion of the infraspinatus may lead to persistent horizontal imbalance of the shoulder [5]. In 2016, Elhassan et al. reported satisfactory results of lower trapezius transfer using Achilles tendon allografts in patients with irreparable posterior-superior rotator cuff tears [6], with several studies subsequently showing promising clinical outcomes [7-9]. In 2018, Valenti et al. adapted this technique using a semitendinosus autograft specifically for patients with isolated loss of external rotation (ILER) [10]. Both studies reported positive outcomes in terms of pain relief and restoration of active external rotation. We hypothesized that lower trapezius tendon transfer could be a viable surgical option for treating isolated musculotendinous lesions in the infraspinatus during the chronic phase when fatty infiltration is ≥ grade III. We present two cases of ILER and shoulder pain due to isolated irreparable lesions in the musculotendinous junction of the infraspinatus, which were successfully treated with lower trapezius transfer.
All the patients provided informed consent for the use of their data and images for research and publications.
Patients’ demographics
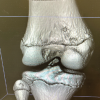
The first patient (Patient 1), a 57-year-old athletic female, experienced the onset of subacromial impingement in her non-dominant shoulder 10 years before presentation, accompanied by posterior calcific tendinopathy. Initial treatment involved barbotage and several subacromial injections, which provided temporary relief for a few months. However, the patient continued to have trouble performing daily activities, with a preoperative visual analog scale (VAS) score of 8. Preoperative active forward elevation (FE) was 60°, with 0° of active external rotation with the elbow at the side (ER1). She exhibited a positive external rotation lag sign exceeding 40°, as well as positive drop sign, with strength in ER1 measured at 0/5. Magnetic resonance imaging (MRI) revealed an isolated musculotendinous lesion in the infraspinatus, associated with calcific tendinopathy and grade IV fatty infiltration (Fig. 1a). The remaining rotator cuff tendons were intact.
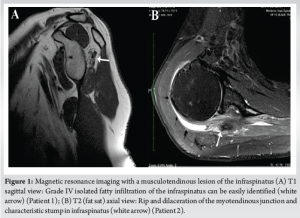
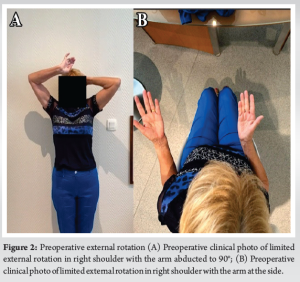
The second patient (Patient 2), a 66-year-old male, experienced pain in his right dominant shoulder several years before presentation. Despite conservative treatment, the patient continued to complain of extreme shoulder pain, with the preoperative VAS score at 9. Regarding preoperative range of motion (ROM), active FE was limited to 40°, and active ER1 was at −15°. A significant external rotation lag sign was observed, the drop sign was positive, and the patient exhibited poor strength in ER1 (1/5) (Fig. 2a and b). MRI results indicated isolated grade IV fatty infiltration of the infraspinatus, ripping (dilaceration) of the musculotendinous junction, and the characteristic stump (Fig. 1b). There were no signs of tear in the remaining rotator cuff.
Despite the absence of a traumatic event and prolonged conservative treatments, both patients presented with complaints of shoulder pain, weakness, and deficits in active external rotation. However, there were no signs of nerve-related problems, including suprascapular nerve palsy, as confirmed by both physical examination and electromyography studies. Plain radiography showed no signs of glenohumeral arthritis, and MRI revealed an isolated musculotendinous lesion in the infraspinatus associated with calcific tendinopathy, while the remaining rotator cuff tendons were intact. Since the infraspinatus was deemed irreparable status with grade 4 fatty infiltration, both patients underwent lower trapezius transfer.
Surgical procedure
Patient-specific findings
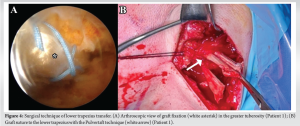
Patient 1: Arthroscopic examination of the glenohumeral joint revealed no glenohumeral arthritis, with intact cartilage. A dystrophic lesion was noted in the deep layer of the rear supraspinatus, but strong continuity of the supraspinatus tendon was observed. An infraspinatus musculotendinous junction lesion with a nearby calcific deposit was identified, but the tendinous portion remained intact. There was fatty infiltration in the infraspinatus muscle belly, and no significant tears in the other remaining rotator cuffs (Fig. 3a).

Patient 2: Arthroscopic examination of the glenohumeral joint revealed glenohumeral arthritis, but the cartilage was intact. There were no significant lesions in the tendinous portion of the infraspinatus. However, significant fatty infiltration of the infraspinatus muscle belly was observed, along with a calcific deposit at the site of the musculotendinous junction lesion. The other remaining rotator cuffs were intact.
Surgical steps
We followed the general surgical steps described by Valenti and Werthel [10]. The surgical procedure was done in beach chair position under general anesthesia for both patients. Initially, bursectomy, extensive synovectomy, and acromioplasty were performed in the subacromial space. The semitendinosus tendon autograft was harvested from the ipsilateral knee and folded independently to obtain adequate length. A mini-open posterior approach was used to dissect the lower trapezius distal to the spine of the scapula. The inferior border of the lower trapezius was released and separated from the infraspinatus fascia. The lower trapezius was then split horizontally from the lateral to medial side at the scapular spine level to separate the lower trapezius from the middle trapezius. The lower trapezius tendon was detached from its insertion site, while taking care to protect the spinal accessory nerve. A tunnel was created between the posterior deltoid and infraspinatus using a blunt instrument to reach the glenohumeral joint. A “window” was then created through the infraspinatus to remove the calcification (Fig. 3b). The autograft was passed through the “window” and fixed arthroscopically with two suture anchors (Versalock, Mitek, Raynham, MA, USA) on the infraspinatus footprint. The lower trapezius tendon was sutured using the Pulvertaft technique (Fig. 4a and b) at the 45°external rotation of shoulder. By rotating the shoulder internally and externally, secure fixation of the autograft in both the humerus and lower trapezius was confirmed.
Post-operative care
Both patients wore a 45° ER1 sling for 6 weeks post-operatively. This was followed by a physiotherapy regimen comprising 4 weeks of passive and pendular mobilization, and subsequently, 8 weeks of progressive active shoulder reinforcement. They were advised to avoid heavy or manual labor until 6 months post-operatively.
Promising clinical results were seen in both patients over a 4-year follow-up. (Patient #1, 50 months; Patient #2, 52 Months) Post-operatively, there was significant alleviation of pain, with VAS 0 for both patients, and functional scores showed satisfying results, with activities of daily living requiring external rotation scores of 30/30 for both patients. Regarding ROM, there was notable improvement in ER1 from 0° to 45° for Patient 1 and from −15° to 45° for Patient 2. Using a portable hanging scale, the measured strength of ER1 improved from 0/5 to 3/5 for Patient 1 and from 1/5 to 3/5 for Patient 2. For both patients, the external rotation lag and dropping signs were negative after surgery. No progression of arthritis was observed. No significant post-operative complications or donor site morbidity were reported.
In this case report, we present the satisfying clinical outcomes of lower trapezius tendon transfer in two patients with irreparable isolated infraspinatus musculotendinous lesions associated with calcific tendinopathy, observed over a comprehensive 4-year follow-up period. The diagnosis of an isolated musculotendinous lesion of the infraspinatus, compounded by calcific tendinopathy, is relatively uncommon and can often be misdiagnosed as extensive posterior-superior cuff tears or compression of the suprascapular nerve. Despite the studies in the literatures, the precise etiology remains elusive, although the condition typically falls into two discernible groups. The primary group includes patients experiencing prolonged shoulder discomfort, often accompanied by calcific tendinopathy and a history of therapeutic injections. Conversely, the secondary group comprises individuals with a history of traumatic events that may have triggered their symptoms [4]. Without effective conservative treatment and suitable surgical intervention, patients with such lesions often experience severe pain and/or disability during daily activities. Treatments for these particular lesions had been attempted with arthroscopic repair, but clinical results are often unpredictable [3,11,12]. Moreover, rapid architectural changes, such as advanced atrophy and high-grade fatty infiltration, frequently manifest post-operatively, contributing to the cautious approach adopted by many surgeons who have discontinued surgical repair for such lesions [1,3,4]. Nonetheless, promising results have been reported by Lee et al. [11], who demonstrated significant clinical improvement in four patients following arthroscopic repair, as evidenced by improvements in VAS score, American Shoulder and Elbow Surgeons scores, and constant scores. However, these outcomes were evaluated only at a 6-month follow-up, and the preoperative status of the lesions was considered potentially repairable. Similarly, Hall et al. [12] reported satisfactory outcomes using a dermal allograft for this condition, although the preoperative condition of the infraspinatus exhibited minimal fatty infiltration. This present case report highlights significant pain relief achieved in both patients post-operatively following lower trapezius tendon transfer augmented by a semitendinous tendon autograft. Both patients demonstrated substantial improvements in ER1, with preoperative external rotation lag sign reversing post-operatively. These favorable outcomes can be attributed to the anatomical similarities between the lower trapezius and infraspinatus, as the lower trapezius exhibits a comparable line of pull and excursion to that of the infraspinatus [13,14]. Finally, our clinical results align with previously reported satisfying results of lower trapezius tendon transfer in managing posterior-superior irreparable rotator cuff tears, with all patients reporting significant pain reduction and restoration of active external rotation [6-10].
In the present case report, we present satisfying results of lower trapezius tendon transfer, which appears effective in alleviating pain and restoring strength and active external rotation in cases of irreparable isolated infraspinatus musculotendinous lesion associated with calcific tendinopathy. However, since the results are limited to only two patients, clinical studies with longer follow-up and a larger number of patients are warranted to thoroughly evaluate the effectiveness of lower trapezius tendon transfer for this specific condition.
Lower trapezius transfer can effectively alleviate pain and restore active external rotation in patients with irreparable isolated infraspinatus musculotendinous lesion.
References
- 1.Tavernier T, Walch G, Barthelemy R, Nove-Josserand L, Liotard JP. Isolated lesion of the infraspinatus at the myotendinous junction: A new lesion. J Radiol 2006;87:1875-82. [Google Scholar | PubMed]
- 2.Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res 1994;304:78-83. [Google Scholar | PubMed]
- 3.Lunn JV, Castellanos-Rosas J, Tavernier T, Barthelemy R, Walch G. A novel lesion of the infraspinatus characterized by musculotendinous disruption, edema, and late fatty infiltration. J Shoulder Elbow Surg 2008;17:546-53. [Google Scholar | PubMed]
- 4.Walch G, Nové-Josserand L, Liotard JP, Noël E. Musculotendinous infraspinatus ruptures: An overview. Orthop Traumatol Surg Res 2009;95:463-70. [Google Scholar | PubMed]
- 5.Kany J. Tendon transfers in rotator-cuff surgery. Orthop Traumatol Surg Res 2020;106:S43-51. [Google Scholar | PubMed]
- 6.Elhassan BT, Wagner ER, Werthel JD. Outcome of lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tear. J Shoulder Elbow Surg 2016;25:1346-53. [Google Scholar | PubMed]
- 7.Elhassan BT, Sanchez-Sotelo J, Wagner ER. Outcome of arthroscopically assisted lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tears. J Shoulder Elbow Surg 2020;29:2135-42. [Google Scholar | PubMed]
- 8.Baek CH, Kim BT, Kim JG, Kim SJ. Mid-term outcomes of arthroscopically assisted lower trapezius tendon transfer using Achilles allograft in treatment of posterior-superior irreparable rotator cuff tear. J Shoulder Elbow Surg 2024;33:1293-305. [Google Scholar | PubMed]
- 9.Baek CH, Kim BT, Kim JG, Kim SJ. Clinical results of arthroscopically-assisted lower trapezius transfer using fascia lata autograft for posterior superior irreparable rotator cuff tear. J Orthop 2024;52:78-84. [Google Scholar | PubMed]
- 10.Valenti P, Werthel JD. Lower trapezius transfer with semitendinosus tendon augmentation: Indication, technique, results. Obere Extrem 2018;13:261-8. [Google Scholar | PubMed]
- 11.Lee KY, Kim SH, Oh JH. Isolated ruptures of the infraspinatus: Clinical characteristics and outcomes. Clin Shoulder Elbow 2017;20:30-6. [Google Scholar | PubMed]
- 12.Hall T, Danielson K, Brandenburg S, Matelic T. A case series of recurrent myotendinous rotator cuff tears repaired and augmented with dermal allograft: Clinical outcomes at two years. J Shoulder Elbow Surg 2020;29:2264-71. [Google Scholar | PubMed]
- 13.Reddy A, Gulotta LV, Chen X, Castagna A, Dines DM, Warren RF, et al. Biomechanics of lower trapezius and latissimus dorsi transfers in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 2019;28:1257-64. [Google Scholar | PubMed]
- 14.Moraiti K, Zampeli F, Reinares F, Gantsos A, Valenti P. Feasibility of lower trapezius transfer extended by the infraspinatus fascia for restoration of external rotation in irreparable posterosuperior rotator cuff tears: An anatomical study. Eur J Orthop Surg Traumatol 2021;31:661-7. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Femoral-Sided Avulsion Fracture Treated with a Novel Arthroscopic Physeal-Sparing Method in a Skeletally Immature Patient
March 1, 2026 Femoral-Sided Avulsion Fracture Treated with a Novel Arthroscopic Physeal-Sparing Method in a Skeletally Immature Patient March 1, 2026 Clinical Outcome of Arthroscopic Anterior Cruciate Ligament Reconstruction with Simultaneous Meniscus Repair
March 1, 2026 Clinical Outcome of Arthroscopic Anterior Cruciate Ligament Reconstruction with Simultaneous Meniscus Repair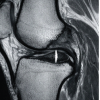 March 1, 2026 Functional Recovery after Arthroscopic Management of Meniscal Tears
March 1, 2026 Functional Recovery after Arthroscopic Management of Meniscal Tears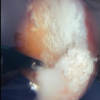 February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report
February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report