
Failure of inflation of balloon can lead to failure of stent which has not been reported so far. This can be due to a malfunction of device but case selection is also vital.
Dr. Mantu Jain, Department of Orthopaedic, AIIMS, Bhubaneswar, Odisha, India. E-mail: montu_jn@yahoo.com
Introduction: Ballon-mounted stentoplasty is the latest cement augment stabilization for osteoporotic vertebral fracture (OVF). The technique is almost similar to kyphoplasty except for stent placement in a created void and filling it with cement. Here, we describe a patient with a failure of balloon inflation in an elderly male presented with OVF.
Case Report: An elderly male presented with OVF of the L1 was planned for stentoplasty. The balloon was inserted inside and inflated but beyond 22–25 atm (atmospheric pressure), the device was turning “false” and returned to zero. This happened again with the stent mounted ballon and the procedure was abandoned and vertebroplasty was done.
Conclusion: Failure of balloon inflation in stentoplasty due to balloon malfunction is a rare complication that has not been reported so far.
Keywords: Osteoporotic vertebral fracture, stentoplasty, malfunction of device, vertebroplasty.
Ballon-mounted stentoplasty is the latest cement augment stabilization for osteoporotic vertebral fracture (OVF) [1,2]. This works on similar principles of vascular stents [3]. The procedure looks very attractive and can potentially restore the height of a collapsed vertebral body in the long term compared to kyphoplasty. The technique is almost similar to kyphoplasty except for stent placement in a created void and filling it with cement. Here, we describe a patient with a failure of balloon inflation in an elderly male presented with OVF.
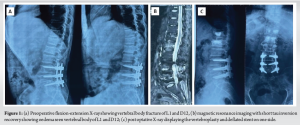
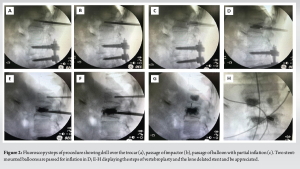
An elderly male presented with OVF of the L1 (with a bone mineral density showing a T-score of −3.7) of 3 weeks history with a pain in the back and intact neurology. The pain was severe with a visual analog score (VAS) scale 7/10 that was mechanical in nature aggravated with tuning on bed and on loading of spine. The X-ray showed a fracture of D12 and L1 (Fig. 1a) and it was confirmed on the magnetic resonance imaging (MRI) showing an acute fracture (Fig. 1b). He was planned for stentoplasty (VBS System, DePuy Synthes, Johnson & Johnson) at L1 and vertebroplasty at D12. The patient was positioned prone and given me an erector spine block at D11 level for the case. The field was sterilised and draped. A wide trocar (number 7) was railroaded over the guide wire pins. The guide wires were removed, a drill was passed in the trocar (Fig. 2a), and an impactor was placed to create the void (Fig. 2b). Nest, balloon was inserted inside and inflated (Fig. 2c), but beyond 22–25 atm (atmospheric pressure), the device was turning “false” and returned to zero. It happened on both sides and on both devices. The balloon was tested outside and found to be working adequately. The stent-mounted balloon was next inserted (Fig. 2d), and after a partial inflation on the left side, the stents did not expand. The right-side stent and balloon could not be inflated. The cement inserter failed to pass through the trocar; vertebroplasty was done on either side of the stent and also on the right side (Fig. 2e-f). At the proximal D12 level, vertebroplasty was done (Fig. 2g-h). Post-procedure, the neurology of the patient was intact. The post operative x-ray was satisfactory (Fig. 1c) and patient discharged next day after mobilisation. He had tremendous relief of pain (VAS of 1/10).
Non-inflation of balloon leading to failure of stent expansion has not been reported. Failure of balloon inflation during kyphoplasty/stentoplasty could be attributed to patient selection or procedural complication. An ideal patient would have more than 35% collapse, 15° kyphosis, and fracture life <4 weeks [4]. Sebaaly et al. proposed an algorithm in which painful OVF should be cement augmented with kyphoplasty for <3 months and vertebroplasty for > 3 months [5]. A consolidated or very bone-dense fracture will have resistance to expansion. MRI showing hyperintensity signal on T2-weighted scans is a clear a marker of oedema which is correlated well with acuteness of fracture and pain levels as seen in our case that was only 3-week-old fracture patient with severe osteoporosis. Technical failure due to balloons has been reported in cardiac stents mainly due to deflation failure but not documented in vertebral body stents [6,7]. Ballon malfunction can be a manufacturing defect, but, in our case, we tested it before insertion. The problem was a failure to elevate the pressure beyond 25 atm as it went “false” and returned to zero every time. It was not happening outside the vertebral body while testing. The company’s instruction manual suggests a maximum pressure of 30 atm (440 psi) can reached without causing a leak due to balloon explosion [8]. We did not test the balloon at the proximal level. As a bail-out procedure, we completed the vertebroplasty at both levels. The other reported complication with balloon kyphoplasty is balloon rupture, cortical fracture, vertebral re-collapse and transient hyperalgesia [9]. Apart from this hematoma and cement leak are other potential complications [10].
Failure of balloon inflation in stentoplasty is a rare complication that has not been reported so far because of limited clinical experiences especially in our set up. There can be malfunction of the device but patient selection is equally important.
This case highlights the importance of cautious balloon inflation, optimal patient selection, and consideration of alternative augmentation techniques in fragile osteoporotic spines to prevent mechanical failure.
References
- 1.Martín-López JE, Pavón-Gómez MJ, Romero-Tabares A, Molina-López T. Stentoplasty effectiveness and safety for the treatment of osteoporotic vertebral fractures: A systematic review. Orthop Traumatol Surg Res 2015;101:627-32. [Google Scholar | PubMed]
- 2.Muijs SP, Nieuwenhuijse MJ, Van Erkel AR, Dijkstra PD. Percutaneous vertebroplasty for the treatment of osteoporotic vertebral compression fractures: Evaluation after 36 months. J Bone Joint Surg Br 2009;91:379-84. [Google Scholar | PubMed]
- 3.Buranakarl T, Jaisanuk K, Varatorn R, Suchato C, Srisuphap S. Stentoplasty (cemented kyphoplasty with stent) under biplane digital subtraction angiography (biplane DSA). BKK Med J 2019;2:48. [Google Scholar | PubMed]
- 4.Heini PF, Teuscher R. Vertebral body stenting / stentoplasty. Swiss Med Wkly 2012;142:1-10. [Google Scholar | PubMed]
- 5.Sebaaly A, Rizkallah M, Bachour F, Atallah F, Moreau PE, Maalouf G. Percutaneous cement augmentation for osteoporotic vertebral fractures. Efort Open Rev 2017;2:293-9. [Google Scholar | PubMed]
- 6.Komócsi A, Költô G, Horváth IG, Kónyi A. Comminution of a prolapsed thrombus after coronary stent implantation using cutting balloon. Interv Med Appl Sci 2012;4:103-5. [Google Scholar | PubMed]
- 7.Yang Y, Yang S, Cheng X, Liu K. A rare case report of the successful withdrawal of a stent balloon that failed to deflate. BMC Cardiovasc Disord 2023;23:190. [Google Scholar | PubMed]
- 8.DePuy Synthes. Vertebral Body Stenting - Surgical Technique. Available from: https://emea.depuysynthes.com/hcp/reprocessing-care-maintenance [Last accessed on 2016. [Google Scholar | PubMed]
- 9.Saliou G, Rutgers DR, Kocheida EM, Langman G, Meurin A, Deramond H, et al. Balloon-related complications and technical failures in kyphoplasty for vertebral fractures. AJNR Am J Neuroradiol 2010;31:175-9. [Google Scholar | PubMed]
- 10.Huang IK, Pua U, Quek LH, Kwan J, Lim GH. Cone-beam computed tomography guided unipedicular central stentoplasty of the thoracolumbar spine: Early technical experience and results. J Med Imaging Radiat Oncol 2020;64:620-5. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 To Study the Functional Outcome of Vertebroplasty versus Conservative Management in Osteoporotic Fractures
May 1, 2025 To Study the Functional Outcome of Vertebroplasty versus Conservative Management in Osteoporotic Fractures November 10, 2019 A Novel Unidirectional Porous ß-tricalcium Phosphate Grafting Impregnated with Bone Marrow Blood Collected from Unfractured Vertebral Bodies for Non-union of Osteoporotic Vertebral Fracture: A Preliminary Case Report
November 10, 2019 A Novel Unidirectional Porous ß-tricalcium Phosphate Grafting Impregnated with Bone Marrow Blood Collected from Unfractured Vertebral Bodies for Non-union of Osteoporotic Vertebral Fracture: A Preliminary Case Report January 10, 2024 Isolated Trochlear Fracture in an Elderly Lady: A Rare and Interesting Case Treated in a Rural Coal Mines Hospital
January 10, 2024 Isolated Trochlear Fracture in an Elderly Lady: A Rare and Interesting Case Treated in a Rural Coal Mines Hospital September 1, 2025 Chondroblastoma of the Right Distal Femur Medial Condyle: A Case Report
September 1, 2025 Chondroblastoma of the Right Distal Femur Medial Condyle: A Case Report