
Bilateral lateral end clavicle fractures are rare injuries typically resulting from high-energy trauma and require careful clinical and radiological evaluation. Dog bone button fixation offers a reliable surgical solution for stabilizing such complex fractures. Early operative management combined with structured rehabilitation leads to favorable functional and radiological outcomes.
Dr. Naveen Sathyaseelan, Department of Orthopaedics, Saveetha Institute of Medical and Technical Sciences, Chennai, Tamil Nadu, India. E-mail: spnaveen17@gmail.com
Introduction: Clavicle fractures, particularly at the lateral end, are uncommon and pose diagnostic and management challenges. Bilateral lateral end clavicle fractures are rare, and surgical management is often necessary to restore shoulder function scenarios.
Case Report: A 52-year-old male presented with bilateral shoulder pain and restricted movements following a motorcycle fall. Clinical and radiological evaluation revealed a right undisplaced lateral clavicle fracture, a comminuted left lateral clavicle fracture, and associated right-sided rib fractures. Surgical fixation using the dog bone button technique was performed bilaterally. Post-operative rehabilitation involved early mobilization, and at 6 weeks, the patient demonstrated significant functional improvement, confirmed by disabilities of the arm, shoulder and hand and Oxford shoulder scores. Radiographs showed good fracture healing with bridging callus formation.
Conclusion: Dog bone button fixation is an effective technique for managing bilateral lateral clavicle fractures, offering good functional and radiological outcomes.
Keywords: Distal third clavicle fracture, dog bone button fixation, bilateral lateral third clavicle fracture.
Distal third clavicle fractures constitute 10–25% of adult clavicle fractures and are typically caused by direct shoulder trauma. Displaced lateral clavicle fractures, though less common than midshaft fractures, have a higher risk of non-union and poorer functional outcomes when treated nonoperatively, making surgical management preferable. Common techniques include rigid plate fixation or coracoclavicular fixation, chosen based on fracture displacement and ligament integrity. While plates ensure anatomical reduction and stability, they may require removal due to implant prominence or restricted movement. The endobutton technique, a newer minimally invasive approach, addresses these limitations by stabilizing fractures with minimal hardware and has demonstrated excellent outcomes.
A 52-year-old male came to the hospital with an alleged history of a slip and fall from a motorcycle and sustained injury to his chest and bilateral shoulder. A history of pain and swelling over the bilateral shoulder was present, which was sudden in onset, aggravated on movement, and relieved on rest. He also gives a history of pain in the right chest. No history of loss of consciousness, Seizures, vomiting, and ENT bleeding. On examination of his bilateral shoulders, there was swelling present, he had tenderness in the lateral end of the clavicle, his shoulder range of movements was significantly restricted due to pain, and there were no neurovascular deficits. His chest compression test was positive on the right side. Plain radiographs of his chest with bilateral shoulders were taken, which showed an undisplaced right lateral end of clavicle fracture, comminuted fracture of the left lateral end of clavicle with fracture of right 4th, 5th, 6th, and 7th rib (Fig. 1a). Computed tomography of the chest showed comminuted extra-articular minimally displaced fracture seen involving the mid and lateral third of the left clavicle with adjacent soft-tissue inflammatory changes. A complete transverse fracture involving the lateral one-third of the right clavicle, with mild inferior displacement of the distal fragment (Fig. 1b). The right acromioclavicular joint (ACJ) appears normal. Comminuted displaced fracture of the posterior shaft of the right 4th, 5th, 6th, and 7th rib.
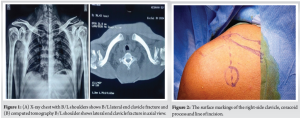
After obtaining surgical fitness, he planned for open reduction with dog bone button fixation for bilateral lateral end of clavicle fracture. Under aseptic precaution and under general anesthesia, the patient is in the beach chair position, with a sandbag placed posteriorly at the medial border and spine of the scapula for support, and straps applied over the head. A Betadine scrub solution was used for pre-washing. An image intensifier was employed to assess the positioning of the implant and ensure proper fracture fixation. The bony landmarks of the clavicle and the fracture site, as well as the coracoid process, were palpated, and the skin incision was marked using a skin marker. A 6 cm vertical incision, commonly referred to as a “Bra strap incision,” was made perpendicular to the clavicle’s long axis, approximately 2–3 cm medial to the ACJ (Fig. 2). The incision was based proximally on the coracoid process. The delto-trapezial fascia was carefully incised to align with the clavicle, and blunt dissection was performed to separate the soft tissues around both sides of the coracoid process.
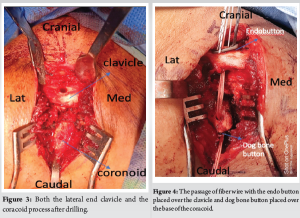
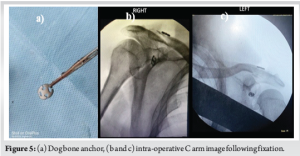
After exposing the coracoid process and the lateral end of the clavicle, a 3.2 mm drill hole was created in both the clavicle and the base of the coracoid process. A guide wire was then passed through, followed by the use of a 3.2 mm cannulated reamer. A Beath pin was inserted to confirm that the tunnel was sufficiently large to accommodate the endobutton and fiber tape (Fig. 3). The beath pin was removed, and the suture material was carefully threaded through the clavicle and into the base of the coracoid process, taking care to avoid any damage to the coracoid. The fiber wire, attached to both the suture material and the endobutton, was then gently pulled from the clavicle down to the base of the coracoid process (Fig. 4). After the endo button was inserted over the clavicle and the fiber wire was passed through the clavicle to the coracoid process, the dog button was secured at the base of the coracoid (Fig. 5a). The fiber wire was gradually tightened, facilitating the reduction of the fracture. Once the fracture was properly reduced, the fiber wire was securely tightened and trimmed. Fixation was checked under C ARM guidance (Fig. 5b and c). The wound was thoroughly irrigated, closed in layers, and covered with a sterile dressing.
Post-operative care after surgery, patients received intravenous antibiotics for 1 day, followed by oral antibiotics for an additional 3 days. Painkillers were given as needed. Post-operative rehabilitation included the following exercises:
- Active shoulder mobilization (flexion, extension, abduction, and adduction)
- Shoulder pendulum exercises
- Elbow, hand, and finger mobilization, starting from the 1st postoperative day (POD).
Sterile dressings were applied, and wound inspections were performed on POD 2 and 5. On the 12th POD, stitches were removed, and the patients were discharged. The patient was then followed up at 6 weeks and showed a significant improvement in his functional outcome according to the disabilities of the arm, shoulder, and hand questionnaire (specific to the upper limb) and the Oxford shoulder score. The X-ray taken at 6 weeks’ follow-up showed good fracture healing with a significant amount of the presence of bridging callus or trabeculations across the fracture site (Fig. 6).

About 10–25% of adult clavicle fractures occur in the distal third segment and are usually caused by direct trauma to the shoulder [1]. Displaced fractures of the lateral clavicle occur less frequently than mid-shaft fractures, but they carry a greater risk of non-union and lead to poorer functional outcomes when managed nonoperatively [2,3]. As a result, surgical treatment is generally recommended for medically fit patients [3,4]. Several surgical techniques have been developed for the treatment of lateral clavicle fractures. Most modern approaches involve open reduction with either rigid plate fixation or coracoclavicular fixation [5-8]. The distal end of the clavicle’s displacement and stability, as dictated by the coracoclavicular ligament’s condition, will decide how these injuries are treated. Significantly superior clavicle displacement occurs in Neer’s type 2 fractures where the coraco-clavicular ligaments are either ripped or connected to the lateral fragment [9]. However, poor bone quality at the distal end of the fracture can increase the risk of fixation failure. In addition, plate removal may be necessary later due to implant prominence or restricted shoulder movement [10,11]. Techniques for treating lateral clavicle fractures such as indirect coracoclavicular ligament stabilisation using methods such as suture anchors, coracoclavicular screw fixation, or double-looped endobuttons, as well as direct osteosynthesis with anatomical pre-contoured locking plates or hook plates. Plate fixation, using either a locking plate or a hook plate, provides the benefit of anatomical reduction and rigid internal fixation, with excellent reported outcomes. Indirect fixation works by neutralizing the forces that cause instability, transforming an unstable fracture into a stable one. This method, which involves minimal hardware, promotes fracture healing by directly addressing the fragments. The endobutton technique, a newer and simpler approach, has been proposed to overcome the limitations of direct osteosynthesis and has shown excellent results [12]. The unstable nature of lateral end clavicle fractures, particularly Neer’s type II, requires special attention. Conservative treatment is generally not appropriate for these fractures due to the continuous strain exerted by the trapezius muscle and the weight of the arm on the shoulder girdle. When distal clavicle fractures in adults are managed nonoperatively, especially with coracoclavicular ligament separation, satisfactory healing is not always achieved. This can lead to symptomatic non-union, often necessitating delayed surgery, as noted by Sarda [13] and Robinson and Cairns [14]. Surgical techniques for managing distal clavicle fractures can be broadly classified into three categories such as direct osteosynthesis using distal clavicle plates (±CC ligament augmentation) or hook plates, tension band and/or trans articular K-wire fixation through the ACJ, indirect reduction using CC ligament reconstruction and direct ligament repair, as per Neer . While locking plate fixation is a reliable method with a high union rate and stable fixation, it becomes less effective in cases where the distal fragment is small or comminuted, limiting its application in such scenarios. The primary advantage of dog bone button fixation over non-suture-based implants is its low rate of requiring a secondary surgical procedure for implant removal. In contrast, implants such as coracoclavicular screws, lateral clavicular plates, and hook plates are often associated with ongoing stiffness, leading many experts to recommend their routine removal [ 15]. However, removing these implants too early can compromise fracture stability and increase the risk of displacement if the fracture has not fully healed. In a study examining bidirectional clavicular loop fixation with two endobuttons over the clavicle, it was found that although the clavicular drill hole increased in size during long-term follow-up, there was no indication of endobutton migration [16]. In addition, Struhl and Wolfson reported encouraging outcomes for coracoclavicular stabilization using a commercially available, prefabricated closed-loop double endobutton. They claim that to prevent anterior over-reduction of the fracture and to minimize the risk of late fracture due to bone degradation, the cerclage wire should be threaded through the drill hole in the coracoid rather than positioned beneath it. Anatomically restoring the coracoclavicular interval, TightRope is a suture button device with adjustable length that inhibits knot fixing. According to Soh et al. [17], the use of the device as a coracoclavicular stabilizer achieved a union rate of approximately 95%. However, some complications were noted, including non-union, malunion, intraoperative coracoid fracture, and shoulder stiffness. Our goal was to provide the patient with a 100% union rate and an excellent clinical outcome with an adequate range of movements to perform his daily activities.
This report highlights a rare case of bilateral lateral end clavicle fractures successfully managed with the dog bone button fixation technique. This innovative approach provided a biomechanically robust construct, resulting in excellent clinical and radiographic outcomes. The case underscores the effectiveness of this technique in addressing complex clavicle fractures while promoting optimal recovery and function.
The use of dog bone button fixation for displaced lateral clavicle fractures is a reliable technique that yields excellent functional outcomes with low complication rates. In addition, routine implant removal is not necessary.
References
- 1.Postacchini F, Gumina S, DeSantis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg 2002;11:452-6. [Google Scholar | PubMed]
- 2.Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res 1968;58:43-50. [Google Scholar | PubMed]
- 3.Nordqvist A, Petersson C, Redlund-Johnell I. The natural course of lateral clavicle fracture. 15 (11-21) year follow-up of 110 cases. Acta Orthop Scand 1993;64:87-91. [Google Scholar | PubMed]
- 4.Eskola A, Vainionpää S, Pätiälä H, Rokkanen P. Outcome of operative treatment in fresh lateral clavicular fracture. Ann Chir Gynaecol 1987;76:167-9. [Google Scholar | PubMed]
- 5.Lee W, Choi CH, Choi YR, Lim KH, Chun YM. Clavicle hook plate fixation for distal-third clavicle fracture (Neer Type II): Comparison of clinical and radiologic outcomes between Neer Types IIA and IIB. J Shoulder Elbow Surg 2017;26:1210-5. [Google Scholar | PubMed]
- 6.Good DW, Lui DF, Leonard M, Morris S, McElwain JP. Clavicle hook plate fixation for displaced lateral-third clavicle fractures (Neer Type II): A functional outcome study. J Shoulder Elbow Surg 2012;21:1045-8. [Google Scholar | PubMed]
- 7.Hsu KH, Tzeng YH, Chang MC, Chiang CC. Comparing the coracoclavicular loop technique with a hook plate for the treatment of distal clavicle fractures. J Shoulder Elbow Surg 2018;27:224-30. [Google Scholar | PubMed]
- 8.Struhl S, Wolfson TS. Closed-loop double endobutton technique for repair of unstable distal clavicle fractures. Orthop J Sports Med 2016 Jul 26;4(7);4:2325967116657810. [Google Scholar | PubMed]
- 9.Neer CS 2nd. Fracture of the distal clavicle with detachment of the coracoclavicular ligaments in adults. J Trauma 1963;3:99-110. [Google Scholar | PubMed]
- 10.Sajid S, Fawdington R, Sinha M. Locking plates for displaced fractures of the lateral end of clavicle: Potential pitfalls. Int J Shoulder Surg 2012;6:126-9. [Google Scholar | PubMed]
- 11.Brouwer KM, Wright TC, Ring DC. Failure of superior locking clavicle plate by axial pull-out of the lateral screws: A report of four cases. J Shoulder Elbow Surg 2009;18:e22-5. [Google Scholar | PubMed]
- 12.Robinson CM, Akhtar MA, Jenkins PJ, Sharpe T, Ray A, Olabi B. Open reduction and endobutton fixation of displaced fractures of the lateral end of the clavicle in younger patients. J Bone Joint Surg Br 2010;92:811-6. [Google Scholar | PubMed]
- 13.Sarda P. Lateral clavicle fractures with coracoclavicular ligament disruption (Neer’s Type IIB): Review of literature and a new technique for all-suture fixation. Indian J Orthop 2019;53:465-71. [Google Scholar | PubMed]
- 14.Robinson CM, Cairns DA. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-82. [Google Scholar | PubMed]
- 15.Lanier PJ, Speirs J, Koehler L, Bader J, Abdelgawad A, Waterman BR. Predictors of persistent pain after fixation of distal clavicle fractures in an active military population. Orthopedics 2018;41:e117-26. [Google Scholar | PubMed]
- 16.Kanchanatawan W, Wongthongsalee P. Management of acute unstable distal clavicle fracture with a modified coracoclavicular stabilization technique using a bidirectional coracoclavicular loop system. Eur J Orthop Surg Traumatol 2016;26:139-43. [Google Scholar | PubMed]
- 17.Soh CJ, Sivapathasundaram N, Parthiban R, Ramanand A. A technique of distal clavicle fracture fixation using the tightrope procedure. Malays Orthop J 2011;5:20-3. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2024 Terrible Triad Injuries around the Elbow: It is Still a Puzzle? Prospective Study
October 1, 2024 Terrible Triad Injuries around the Elbow: It is Still a Puzzle? Prospective Study September 10, 2017 Bilateral Anterior Shoulder Dislocation in the Elderly – A Case Report and Review of the Literature
September 10, 2017 Bilateral Anterior Shoulder Dislocation in the Elderly – A Case Report and Review of the Literature July 10, 2013 Progressive Brachial Plexus Palsy after Osteosynthesis of an Inveterate Clavicular Fracture
July 10, 2013 Progressive Brachial Plexus Palsy after Osteosynthesis of an Inveterate Clavicular Fracture February 1, 2026 Single-Stage Correction of Genu Recurvatum with Dual-Pillar Plating – A Case Report
February 1, 2026 Single-Stage Correction of Genu Recurvatum with Dual-Pillar Plating – A Case Report