
Open dislocation of hallux interphalangeal joint in the pediatric population is a rare type of injury that, when encountered can be successfully managed with surgical irrigation and debridement, reduction along with temporary K-wire fixation.
Dr. Demah Mohammed Benfaris, Department of Pediatric Orthopedics, King Saud University Medical City, Riyadh, Saudi Arabia. E-mail: deema.alfaris@hotmail.com
Introduction: Despite frequent toe injuries in the pediatric population, first interphalangeal joint dislocations remain an infrequently observed injury. The hallux interphalangeal joint is inherently a stable joint, supported by collaterals, joint capsule, volar To the best of our knowledge, there have been no published reports specific to this injury pattern in the pediatric population.
Case Report: We report a case of open HIP joint dislocation in a 7-year-old boy surgically managed with irrigation and debridement and K-wire fixation. The HIP joint was found to be stable at 4 weeks after K-wire removal and the patient had full, painless HIP joint range of motion at 24 weeks.
Conclusion: Despite being a rare injury, from our experience, open HIP joint dislocation in the pediatric population can be successfully managed with surgical irrigation and debridement, reduction, capsule repair, and temporary K-wire fixation.
Keywords: Open big toe dislocation, open hallux dislocation, pediatric big toe dislocation, hallux interphalangeal joint dislocation, pediatric open big toe dislocation, pediatric open hallux dislocation, open first interphalangeal joint dislocation.
Despite frequent toe injuries in the pediatric population, first interphalangeal joint dislocations remain an infrequently observed injury. The hallux interphalangeal joint (HIJ) is inherently a stable joint, supported by collaterals, joint capsule, volar plate, as well as dynamic stabilizers, including flexor hallucis longus (FHL) and extensor hallucis longus [1]. Open HIP joint dislocations are considered rare, especially in children. In a thorough literature review, we only found one reported pediatric patient, a 9-year-old boy, in a retrospective case series of toe interphalangeal dislocations in whom the great toe was affected; however authors did not specify whether the injury was open or closed upon presentation [2]. In this case report, we present an open dislocation of the first interphalangeal joint for a 7-year-old boy who presented to our pediatric emergency department (ED) after trauma.
A 7-year-old healthy, fully vaccinated boy was brought by his parents to our institution’s pediatric ED complaining of right big toe deformity and open wound after a history of trauma while playing with his sibling at home, described as tripping on a hyper-plantarflexed big toe. (Fig. 1 and 2).
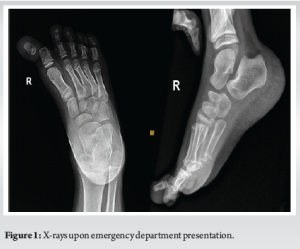

The patient was initially attended and examined by an emergency physician who then started intravenous (IV) cefazolin and consulted orthopedic surgery as a case of open first interphalangeal joint dislocation. Upon examination from the orthopedic resident oncall, the patient was found to have an approximately 3 cm transverse laceration along the plantar and lateral aspect of the base of the right big toe. After irrigation with normal saline, no visible contamination was noted, and the articular surface of the proximal phalanx was exposed. Cap refill noted to be <2 s and gross toe sensation was intact. Radiographs confirmed a medial HIJ dislocation. The nature of condition and management plan was discussed with the patient and his parents, and consents were obtained. After obtaining narcotic analgesia, closed reduction was successfully done by the orthopedic resident oncall, utilizing a traction and lateral translation maneuver, the wound was covered by wet-to-dry sterile gauze and immobilized with plaster and buddy taping. The patient was then booked for exploration, irrigation, and debridement with K-wire fixation as CAT-II. The patient underwent surgical intervention under general anesthesia the next day, found to have an intact FHL tendon and volar plate, the capsule was repaired, wound was irrigated thoroughly, and the HIP joint was fixed with a retrograde 1.8 mm Kirschner wire, wound closed primarily with prolene. Proper K-wire placement and joint reduction confirmed under orthogonal intra-operative radiographs utilizing C-arm. Cap refill was noted to be <2 s. The joint was immobilized with a short backslab with extension to toes, reflected distally to cover the bent K-wire tip to avoid inadvertent removal by the child (Fig. 3).

The patient was discharged after 48 h of IV antibiotics (cefazolin) post-operatively, advised forefoot off-loading and prescribed oral cefuroxime for 7 days with a follow-up in the clinic the following week for wound check. Two weeks post-surgery, the wound was healed, and sutures were removed, big toe sensation was preserved, X-rays showed a stable implant and HIP joint. At 4 weeks post-operatively, the K-wire was removed, and radiographs showed a stable HIP joint. At 12 weeks, the patient had a painlessly mobile great toe. At 24 weeks follow-up the patient was found to have a painless full right big toe range of motion and was hence discharged from the clinic (Fig. 4 and 5).

No previous report of open first interphalangeal joint dislocation in the pediatric population was found in the literature. The largest reported series on toe interphalangeal joint dislocations was reported by Isaac and colleagues in their retrospective case series of 18 patients, 6 of which involved the great toe, 2/6 were 16 years of age presenting with a closed injury and ⅙ was a 9 year old boy who was managed surgically, unfortunately authors only specified in their review that 6/7 patients in whom open reduction had open wounds, without further details whether the pediatric patient was amongst them [2]. Jones et al. reported two open HIJ dislocations in adult patients with a similar mechanism of injury during combative training, concluding that having the bare toes stuck between mats with a pivoting movement can create forces that reproduce this injury pattern [3]. Other mechanisms of injury, such as football trauma have also been reported in an adult with open HIP joint plantar dislocation [4]. Irreducible closed HIP joint dislocations in adults were previously reported in the literature, accounting for interposition of the volar plate and/or sesamoids as the cause which can pose and interesting challenge in the pediatric population considering that the hallucal ossicles do not ossify until late during the first decade of life, between 8 and 12 years [5-7]. Two separate reports of adult closed irriducibile HIP joint dislocations described assisted reduction with the aid of K-wires and 18-gauge needles, respectively [8,9]. In our pediatric patient, we did not encounter difficulties in reduction. In a report by Crosby et al. describing an irreducible closed HIP joint in an adult, hyperextension with axial loading was proposed as the causative forces active on the joint [10]. We have come across an interesting case of open simultaneous first metatarsophalangeal and interphalangeal joint dislocation in an adult [11]. The paucity in the literature regarding HIP joint dislocations can be explained by shoe wear, inherent first interphalangeal joint static and dynamic stability, as well as the tendency of toe injuries to affect the little toe.
Despite being a rare injury, from our experience, open HIP joint dislocation in the pediatric population can be successfully managed with an attempt of reduction in the ED, followed by timely surgical irrigation and debridement, capsule repair, +/- reduction, and temporary K-wire fixation.
Open HIJ dislocation in the pediatric population is a rare injury pattern that can be successfully managed with prompt surgical intervention, with excellent long-term results.
References
- 1.Paulus MC, Neufeld SK. Irreducible longitudinal distraction-dislocation of the hallux interphalangeal joint. Am J Orthop (Belle Mead NJ) 2013;42:329-30. [Google Scholar | PubMed]
- 2.Yang IB, Sun KK, Sha WL, Yu KS, Chow YY. Interphalangeal dislocation of toes: A retrospective case series and review of the literature. J Foot Ankle Surg 2011;50:580-4. [Google Scholar | PubMed]
- 3.Jones MD, May IC, Sweet KJ. Rare open hallux interphalangeal joint dislocations sustained in combatives training: A case series. Mil Med 2014;179:e253-8. [Google Scholar | PubMed]
- 4.Malahias MA, Oikonomou D, Kadu VV, Kotsapas M, Paschos NK, Giotis D. Open interphalangeal dislocation of the great toe in an amateur football player: A rare case report. J Orthop Case Rep 2020;10:78-81. [Google Scholar | PubMed]
- 5.Yasuda T, Fujio K, Tamura K. Irreducible dorsal dislocation of the interphalangeal joint of the great toe: Report of two cases. Foot Ankle 1990;10:331-6. [Google Scholar | PubMed]
- 6.Ab Rahman S, Sulaiman AR, Muzaffar T. Irreducible dorsal dislocation of the interphalangeal joint of the big toe: A case report. Trauma Case Rep 2016;3:32-5. [Google Scholar | PubMed]
- 7.Sun T, Wang L, Zhao H, Wu W, Hu W. Prevalence, morphological variation and ossification of sesamoid bones of the forefoot: A retrospective radiographic study of 8,716 Chinese subjects. J Clin Transl Res 2016;2:91-6. [Google Scholar | PubMed]
- 8.Özdemir E, Evren AT, Özer M, Altay M. Percutaneous reduction of irreducible dislocation of the interphalangeal joint of the hallux: A simple technique for a rare injury. Jt Dis Relat Surg 2020;31:610-3. [Google Scholar | PubMed]
- 9.Takeda S, Nishimura A, Yamaji S, Tabuchi A, Sudo A, Hirata H. Percutaneous reduction of a dislocation of the interphalangeal joint of the great toe: A case report. J Foot Ankle Surg 2020;59:1072-5. [Google Scholar | PubMed]
- 10.Crosby LA, McClellan JW 3rd, Prochaska VJ. Irreducible dorsal dislocation of the great toe interphalangeal joint: Case report and literature review. Foot Ankle Int 1995;16:559-61. [Google Scholar | PubMed]
- 11.Henderson CE, Denno GJ. Simultaneous open dislocation of the metatarsophalangeal and interphalangeal joints of the hallux: A case report. Foot Ankle 1986;6:305-8. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2018 Axillary Artery Injury Following Closed Reduction of an Age-Indeterminate Anterior Glenohumeral Dislocation
July 10, 2018 Axillary Artery Injury Following Closed Reduction of an Age-Indeterminate Anterior Glenohumeral Dislocation November 10, 2018 Open Treatment of Closed Talus Dislocation without Fracture: A Case Report and Literature Review
November 10, 2018 Open Treatment of Closed Talus Dislocation without Fracture: A Case Report and Literature Review April 10, 2022 Surgical Treatment Modalities in Pediatric Monostotic Fibrous Dysplasia of Proximal Femur – A Case Series
April 10, 2022 Surgical Treatment Modalities in Pediatric Monostotic Fibrous Dysplasia of Proximal Femur – A Case Series March 10, 2024 Computer Navigation-assisted Bilateral Total Knee Arthroplasty with Osteosynthesis in Single Sitting in Patients Presenting with Distal Femur Fracture with Pre-existing Knee Arthritis: A Case Series
March 10, 2024 Computer Navigation-assisted Bilateral Total Knee Arthroplasty with Osteosynthesis in Single Sitting in Patients Presenting with Distal Femur Fracture with Pre-existing Knee Arthritis: A Case Series