
Case of Volkmann's Ischemic Contracture treated with surgical release reduces disability and gives better functional hand.
Dr. T Binay Gowda, Department of Orthopaedic, BGS Global Institute of Medical Sciences, BGS Health and Education City, Bengaluru, Karnataka, India. E-mail: binaygowda97@gmail.com
Introduction: The Volkmann’s ischemic contracture (VIC) of the forearm is a sequel of the compartment syndrome of the forearm. We present a case of VIC treated by the Max page operation with a good functional outcome.
Case Report: We report a case of 14-year-old boy with fingers flexion contracture, decreased hand mobility and pain on his left hand. He had a history of left forearm fracture and that was treated by a traditional bonesetter with herbs and cardboards 6 months back. Later he started to have pain and deformity of left hand for which they came to the BGS Global Institute of Medical Sciences and diagnosed with VIC and started with antibiotics, analgesics and performed a Max Page operation after thorough work up.
Discussion: Tight external splint age for supracondylar fractures of the humerus was the most common cause of ischemic contracture. The treatment of an established contracture is complicated and depends on the severity of the infarction and the affected muscle and nerve tissue. Flexor origin slide was the preferred treatment if the flexors still retain adequate strength. The procedure is simple and easy to perform. Adequate muscle release and proper post-operative physiotherapy are key to achieving good results.
Conclusion: VIC is not uncommon following a fracture treated in a traditional bonesetter. For moderate VIC, the flexor origin slide procedure and tendon transfer could still give benefit.
Keywords: Volkmann ischemic contracture, compartment syndrome, and Max page operation.
In 1881, Volkmann described a condition involving muscle ischemia and necrosis that subsequently led to fibrosis and contracture of the forearm [1]. In 1909, Thomas [2] collected 107 cases that had been reported in the literature and among these were cases in which no splint or bandage had been applied. Brooks [3] described a similar condition and believed that venous obstruction was the main factor involved in contracture formation. It is now well recognized that ischemic contractures can develop from many different injuries, as long as the injuries cause swelling of the soft tissues that are contained in relatively non-distensible Osseo-fascial compartments [4]. As a result of this swelling, intramuscular pressure is elevated to a magnitude sufficient to occlude capillary perfusion. The compartments with the least ability to expand are most severely affected by this ischemic insult. Because the deep flexor compartment of the forearm lies next to the bone, it is the first and most severely affected variable levels of necrosis and fibrosis, though to a lesser degree, may also be evident in the flexor digitorum superficialis and the superficially located muscles, such as the wrist flexors. The muscle degeneration which follows is most marked in the middle and its extent decreases peripherally, so that a so-called ellipsoid-shaped infarct as described by Seddon may be the end result. Nerve trunks running in the ischemic zone also suffer damage; this is initially caused by ischemia but is later aggravated by the subsequent muscle fibrosis. The incidence of Volkmann’s contracture is low and it is considered as a rare condition with an incidence of 0.5%. The treatment of an established contracture is complicated and depends on the severity of the infarct and the affected muscle and nerve tissue [5]. It includes physiotherapy, splinting, muscle sliding, tendon transfer, neurolysis, fibrotic tissue excision, muscle grafting and osteotomy [6]. In our case report the Volkmann ischemic contracture (VIC) was caused by excessively tight splint wrapped around the forearm fracture applied by a traditional bonesetter treated successfully with Max page muscle sliding operation.
Here is a 14-year-old boy came to orthopedic department at BGS Global Institute of Medical Sciences hospital (GIMS) with complaints of pain in the left forearm and inability to move left forearm for 6 months. Patient gives history of fall from bicycle after which patient sustained injuries to left elbow for which he took osteopath treatment for 1 week where herbs and cardboard was used. Following which patient developed soakage of wound dressing then took him to other private hospital where X-ray was done, wound was managed and advised for follow-up after 6 months for deformity correction. Later patient came to BGS GIMS for further management. On examination, wasting of the thenar and hypothenar eminence noted, a hypopigmented scar of about 7 × 5 cm present over volar aspect of proximal forearm, hypoesthesia noted over palmar aspect of hand. Movements at elbow both supination and pronation were reduced. There was a flexion deformity at left elbow and wrist joint, hyperextension at the metacarpophalangeal joint, flexion at the proximal interphalangeal, and distal interphalangeal joints. (Fig. 1,2)


Later X-ray was done which showed 6-month-old supracondylar fracture (Figure 1) and diagnosed VIC of the left upper limb, moderate degree based on Tsuge classification (Table 1). Patient was treated with analgesics, antibiotics and other supportive measures. Later under general anesthesia Max Page release surgery was done (Fig. 3). Post-operatively antibiotics, analgesics were continued and good correction was seen at 6months follow up (Fig. 4). A splint was applied to maintain correction (Fig. 5).




VIC is a permanent flexion deformity caused by ischemia that results in a claw-like presentation of the hand. The key precipitating event was acute compartment syndrome, which may occur due to decrease in compartment size or an increase in the volume of the compartment, which can lead to a decrease in blood flow to the muscles and nerves within that compartment. Any cause of compartment syndrome may result in VIC. Intercompartmental pressures of >30 mmHg significantly impair the arterial circulation and are indicative of compartment syndrome [7]. VIC is late sequelae of compartment syndrome that occurs when there is sustained ischemic damage to the muscles [8]. Acute compartment syndrome is predominantly caused by acute fracture trauma, but it may also result from soft tissue crush injuries or vascular complications [9-11]. The etiology of traumatic hand compartment syndrome into three groups: Soft tissue injury-related, fracture-related, and vascular injury-related causes. The most common etiology of hand compartment was related to soft tissue injuries, which constituted 86.8 % of all etiologies [12]. Supracondylar humerus fracture and forearm fracture were the most associated fractures with the development of compartment syndrome and VIC afterward [13]. Other rare causes mentioned in the literature [14-16] include intoxication, infusion of hypertonic dextrose extra venously, chemotherapy perfusion for therapy of malignant cancers, and following excision of congenital radioulnar synostosis. VIC has a wide clinical spectrum based on the degree of the nerve injury and the level of muscle necrosis. The signs and symptoms of compartment syndrome include the following: Pain (out of proportion to what one would expect, especially with passive stretch of the muscles). This is the most common complaint. Paresthesia, paralysis, pallor (pale color), poikilothermia (cold distal extremity compared to the contralateral side) and pulselessness. Patients with an ischemic contracture, in contrast to those with acute compartment syndrome, do not experience pain; instead, they have deformity of the wrist, hand, and fingers that causes the hand to have a claw-like appearance, decreased sensation, paleness of the skin, muscle weakness and loss (atrophy) and dysfunction brought on by the ischemia episode and the ensuing muscle scarring and fibrosis. The treatment of ischemic contracture depends on the severity of the condition and the underlying cause [17,18]. Mild ischemic contracture can be treated with splinting and hand therapy, while moderate ischemic contracture can be treated with surgical techniques, such as flexor tendons lengthening or tendons transfer. Severe ischemic contracture requires surgery, which can be graded according to the severity of the deformity. Max Page in 1923 stated that if the muscle bellies are spared, one can perform the release of muscle insertions, achieving excellent results [19]. This technique was later popularized by Scaglietti [20] and Gosset [21]. Since then, this technique has produced remarkable results as compared to infarcted muscle excision and muscle lengthening [22,23].Post-intervention care may include splinting and rehabilitation to optimize outcomes. Splints are used in rehabilitation to help maintain finger and wrist position and prevent further contracture. (Fig. 5).
Immediate identification of the compartment syndrome and its early treatment is mandatory to avoid its devastating consequences, such as VIC. Once the contracture sets in, the prognosis is always guarded, even after long and intensive physiotherapy and various restorative surgical techniques. Good functional outcomes were achieved in majority of moderate VIC’s operated with Max Page muscle sliding operation. We therefore recommend Max Page muscle sliding operation as the operation of first choice to treat moderate VIC of the forearm.
Proper assessment and surgical release of Volkmann’s Ischemic Contracture gives good functional outcome of hand
References
- 1. Volkmann R. Die ischaemischen muskellahmungen und kontracturen. Zentralbl Chir 1881;8:801-3. [Google Scholar] [PubMed]
- 2. Thomas JJ. Nerve involvement in the ischemic paralysis and contracture of Volkmann. Ann Surg 1975;57A:925-9. [Google Scholar] [PubMed]
- 3. Brooks B. Pathologic changes in muscle as a result of disturbances of circulation: An Experimental study of Volkmann’s ischemic paralysis. Arch Surg 1922;5:188-216. [Google Scholar] [PubMed]
- 4. Yamaguchi S, Viegas SF. Causes of upper extremity compartment syndrome. Hand Clin 1998;14:365-70, viii. [Google Scholar] [PubMed]
- 5. Khan F, Cheema TA, Bhatti ZI. Volkmann’s ischemic contracture; Post-circumferential contracture of the forearm. Prof Med J 2014;21:550-5. [Google Scholar] [PubMed]
- 6. Jan AU, Cheema TA, Buksh W, Shafiq M, Turi BH, Ullah F. Outcome of max page muscle sliding operation for the treatment of moderate Volkmann’s ischemic contracture of the forearm. J Pak Orthop Assoc 2020;32:136-40. [Google Scholar] [PubMed]
- 7. Dasgupta R, Ekka NM, Das A, Kumar V. Evaluation of clinical and venous blood parameters as surrogate indicators in assessing the need for fasciotomy in lower limb compartment syndrome. Int J Low Extrem Wounds 2021;23:403-11. [Google Scholar] [PubMed]
- 8. Kistler JM, Ilyas AM, Thoder JJ. Forearm compartment syndrome: Evaluation and management. Hand Clin 2018;34:53-60. [Google Scholar] [PubMed]
- 9. Newmeyer WL, Kilgore ES Jr. Volkmann’s ischemic contracture due to soft tissue injury alone. J Hand Surg Am 1976;1:221-7. [Google Scholar] [PubMed]
- 10. Maeckelbergh L, Colen S, Anné L. Upper arm compartment syndrome: A case report and review of the literature. Orthop Surg 2013;5:229-32. [Google Scholar] [PubMed]
- 11. Pasque CB, Hendrix C. Baseball related injuries: A case report on acute compartment syndrome of the forearm. Case Rep Orthop 2022;2022:5449913. [Google Scholar] [PubMed]
- 12. Alsaedi O, Alshahir AA, Alsuhaibani O, Beek A, Alduheim M, Alzahim A, et al. Etiology of trauma-related acute compartment syndrome of the hand: A systematic review. Cureus 2023;15:e38218. [Google Scholar] [PubMed]
- 13. Griffart A, Gauthier E, Vaiss L, Williams T, Mallard F, Le Nen D. Functional and socio-professional results of Volkmann syndromes after surgery. Rev Chir Orthop Traumatol 2019;105:287-91.</p> [Google Scholar] [PubMed]
- 14. <p>14. Reigstad A, Hellum C. Volkmann’s ischaemic contracture of the forearm. Injury 1980;12:148-50. [Google Scholar] [PubMed]
- 15. Eichler GR, Lipscomb PR. The changing treatment of Volkmann’s ischemic contractures from 1955 to 1965 at the Mayo clinic. Clin Orthop Relat Res 1967;50:215-23. [Google Scholar] [PubMed]
- 16. Chuang DC, Carver N, Wei FC. A new strategy to prevent the sequelae of severe Volkmann’s ischemia. Plast Reconstr Surg 1996;98:1023-31; discussion 1032-3. [Google Scholar] [PubMed]
- 17. Mirza TM, Taqi M. Volkmann contracture. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 18. Hovius SE, Ultee J. Volkmann’s ischemic contracture. Prevention and treatment. Hand Clin 2000;16:647-57. [Google Scholar] [PubMed]
- 19. Page C. An operation for the relief of flexion-contracture in the forearm. J Bone Joint Surg Am 1923;3:233-4. [Google Scholar] [PubMed]
- 20. Scaglietti O. Surgical treatment of Volkmann’s paralysis. Verh Dtsch Orthop Ges 1957;45:219. [Google Scholar] [PubMed]
- 21. Gosset J. Surgical de-insertion of the muscles of the anterior compartment of the forearm in the treatment of contractures and ischemic reactions. Ann Chir 1956;32:509-15. [Google Scholar] [PubMed]
- 22. Seddon HJ. Volkmann’s contracture: Treatment by excision of the infarct. J Bone Joint Surg 1956;32B:152-74. [Google Scholar] [PubMed]
- 23. Tsuge K. Treatment of established Volkmann’s contracture. J Bone Joint Surg Am 1975;57A:925-9. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2024 Beyond Tradition: “Figure of 8” Casting for Gartland Type 1 and Type 2A Pediatric Supracondylar Fractures of Humerus: Video Technique
October 1, 2024 Beyond Tradition: “Figure of 8” Casting for Gartland Type 1 and Type 2A Pediatric Supracondylar Fractures of Humerus: Video Technique September 1, 2024 Compartment Syndrome Following Intramedullary Nailing of the Tibia: A Case Report
September 1, 2024 Compartment Syndrome Following Intramedullary Nailing of the Tibia: A Case Report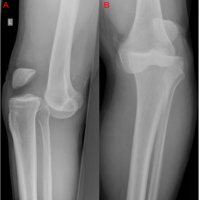 June 10, 2024 Low impact injury resulting in a Schenck type IV classified anterior kneedislocation as well as biceps femoris rupture: A Case Report
June 10, 2024 Low impact injury resulting in a Schenck type IV classified anterior kneedislocation as well as biceps femoris rupture: A Case Report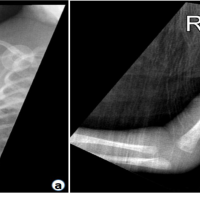 May 10, 2024 Neonatal Compartment Syndrome Secondary to a Failed Peripheral Inserted Central Catheter Insertion: A Case Report
May 10, 2024 Neonatal Compartment Syndrome Secondary to a Failed Peripheral Inserted Central Catheter Insertion: A Case Report