
Septic arthritis of the knee caused by Serratia marcescens in immunocompromised patients can present atypically and may contribute to pathological fractures, necessitating prompt surgical intervention and targeted antimicrobial therapy.
Dr. J S R G Saran, Department of Orthopaedics, M S Ramaiah University of Applied Sciences, Bengaluru, Karnataka, India. E-mail: jsaran868@gmail.com
Introduction: Septic arthritis is an acute condition of the joints that warrants an emergency procedure of joint arthrotomy with debridement, IV antibiotics postoperatively and commonly affects big joints, which include the hip, knee, and shoulder. Serratia marcescens causing septic arthritis is quite rare and is mainly seen in immunocompromised individuals, and very limited literature is present pertaining to the same.
Case Report: A 65-year-old male patient presented to the hospital with sudden inability to bear weight on his right lower limb, inability to flex the knee, which was associated with swelling of the knee, and the limb was externally rotated for 3 days. A fracture of the right neck of the femur was identified on X-ray of the pelvis with bilateral hips. There was no history of trauma. He is a known case of chronic kidney disease for 3 years and is also a known hypertensive and type 2 diabetes mellitus for 15 years, and is currently undergoing dialysis thrice per week. The affected knee was aspirated and was found to have S. marcescens infection, localized there itself; blood culture and intraoperative hip aspirate were negative for the same organism. He underwent right knee arthrotomy with synovectomy and was started on IV antibiotics based on the culture and sensitivity report.
Conclusion: Septic arthritis of the knee joint, along with pathological fracture of the neck of the femur in immunocompromised patients, has to be addressed and given special focus for diagnosis and treatment. Swelling of the knee with inability to flex and acute pain is a sign of septic knee and joint aspiration and antibiotic cover is the mainstay of the treatment, but in cases of acute septic knee, it will require knee arthrotomy with synovectomy and joint debridement.
Keywords: Serratia marcescens, pathological fracture of neck of femur, septic arthritis.
Septic arthritis is described as an emergent articular disease of the joints for which early diagnosis and surgical management with antibiotics has been the mainstay of the treatment. The first case of septic arthritis was reported in 1902 by Walter Whitehead in the knee, and later, further studies were conducted and research was done on the management [1]. It is mainly seen affecting large joint, which include the knee, hip, and shoulder. It can be caused by a variety of organisms, but predominantly includes bacteria, viruses, and fungi. About 75–80% of the cases are caused by Gram-positive cocci, of which Staphylococcus aureus has been at the pinnacle as the root cause, and about 15–20% of the cases are attributed to Gram-negative bacilli and are quite uncommon [2]. The latter has been attributed to be more commonly occurring in immunocompromised patients and causes extensive joint damage with higher chances of recurrence and would require a longer duration of treatment. Currently, we report a case of septic arthritis of the knee caused by Serratia marcescens in an immunocompromised senile patient with a pathological neck of femur fracture, and emphasize the fact that early detection and management of the condition give a better prognosis.
A 65-year-old male, known case of chronic kidney disease (CKD) for the past 3 years and currently undergoing hemodialysis 3 times per week, presented to the nephrology outpatient department for routine follow-up. He reported a 3-day history of difficulty lifting his right leg, along with swelling and pain in his right knee, and was referred to the orthopedics department for further evaluation. On presentation, the patient had an externally rotated right lower limb with apparent shortening, accompanied by pain and swelling in his right knee, his primary complaint. The knee pain was described as sudden in onset, progressively worsening, non-radiating, and non-referred. It was exacerbated by even minimal movement of the joint and alleviated by immobilization and bed rest. He also noted associated swelling in the knee. There was no history of trauma, fever, recent weight loss, or previous tuberculosis. The patient is also a known case of type 2 diabetes mellitus and hypertension for the past 15 years and is compliant with his prescribed medications. On examination, the right lower limb was noted to be externally rotated with an apparent shortening of approximately 0.5 cm. The knee was held in extension and exhibited diffuse tenderness and swelling, predominantly over the suprapatellar and parapatellar regions, along with a local rise in temperature. The joint appeared tense on palpation. Hip range of motion was restricted and painful, particularly with internal rotation. A straight leg raise test was possible up to 70°, though passive elevation beyond that was not feasible. Passive knee flexion was limited to 20° and was markedly painful, with active flexion not possible. The patient was hypertensive with a blood pressure of 148/92 mmHg, tachycardic at 102 beats/min, tachypneic at 22 breaths/min, and afebrile with a recorded temperature of 38.7°C. He maintained an oxygen saturation of 96% on room air. Laboratory investigations revealed a hemoglobin level of 8.4 g/dL, total leukocyte count of 8130 cells/mm3, and an elevated serum urea level of 102 mmol/L, consistent with his known CKD. Radiographic evaluation of the right hip and knee showed a pathological subcapital fracture of the femoral neck with no associated soft-tissue injury. While no definitive bony abnormalities were noted in the knee, there was significant soft tissue swelling and edema (Fig. 1).

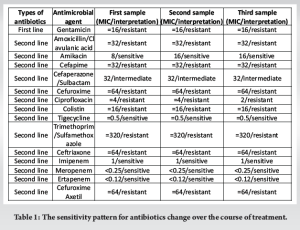
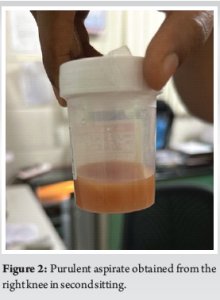
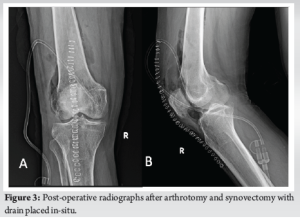
An initial aspiration of approximately 30 mL of synovial fluid was performed from the right knee on the day of presentation, which led to slight symptomatic relief. The aspirate was sent for culture and sensitivity testing, which after 48 h revealed S. marcescens, sensitive to amikacin and select carbapenem antibiotics. The patient was initiated on intravenous amikacin 500 mg twice daily and oral Faropenem 200 mg twice daily. Given the presence of a central venous catheter inserted at an outside hospital, which was suspected to be a potential source of infection, it was removed and replaced with a new central line under sterile conditions in the operating theatre. The patient initially showed clinical improvement and was discharged. However, 1 week later, he returned with a recurrence of the right knee swelling and symptoms similar to his initial presentation. He was taken to the operating theatre, where approximately 20 mL of purulent fluid was aspirated from the knee and 1 mL from the hip joint (Fig. 2). Both samples were sent for repeat culture and sensitivity testing. While the hip aspirate was sterile, the knee aspirate again showed heavy growth of S. marcescens. Notably, the minimum inhibitory concentration for amikacin had increased, indicating emerging resistance. Consequently, amikacin was discontinued. The patient subsequently underwent right knee arthrotomy with synovectomy and extensive joint lavage using 5 L of saline. A surgical drain was placed and intraoperative tissue and synovial fluid samples were sent for culture and sensitivity. Post-operative radiographs did not show any obvious abnormalities (Fig. 3). Intravenous meropenem 1 g twice daily was initiated and continued based on the updated sensitivity profile (Table 1) and continued for 6 weeks.
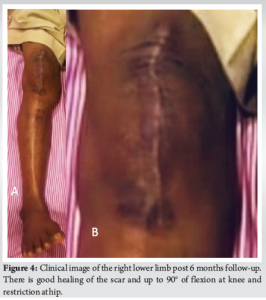
Postoperatively, the drain collected approximately 200 mL and was removed on the 2nd day. Regular dressing changes, physiotherapy, and progressive mobilization were commenced. At 2-month follow-up, the surgical wound had healed well with no signs of infection with no gaping, discharge, swelling, or fluid collection. The patient had regained a knee range of motion of up to 90° (Fig. 4). Regarding the pathological fracture of the femoral neck, a total hip replacement was planned. However, due to financial and personal limitations, the patient declined surgical intervention. The fracture is therefore anticipated to progress toward fibrous non-union.
S. marcescens is an opportunistic gram-negative bacillus, which belongs to the order of Enterobacteriales and family Enterobacteriaceae (Table 2) [3,4]. It was first identified as a cause of discoloration of the body of cornmeal mush by an Italian pharmacist, Bartolomeo Bizio. It is a motile organism that is widespread in the environment but rarely causes disease in humans. It is known to cause urinary tract infections, nosocomial pneumonia, surgical wound, and bloodstream infections in immunocompromised individuals and people who underwent recent surgical procedures [5]. The infections caused by this organism are usually nosocomial in nature. The incidence of this organism has been found to be increased over the past few years. Serratia species are generally found in a variety of climates, which include water and soil, but most commonly in healthcare settings [5]. Currently, 14 species of Serratia are recognized within the genus, eight of which are associated with human infection. Of the eight species implicated in clinical infection, S. marcescens, Serratia liquefaciens, and Serratia odorifera are best known to cause human infections [3,5]. Since our patient is a known case of CKD, he was predisposed to the infection due to his immunocompromised state, and the medications (steroids and immune suppressors) during dialysis further lowered his immunity. Since all the procedures done to him were under standard aseptic conditions and the surgical procedure was done in the OT, the most likely cause for the inoculation of the organism would be the central line present through the external jugular vein.
There have been few literatures regarding critically ill patients with septic joints secondary to hematogenous spread, and these patients had either central catheters or acquired urinary tract infections with cultures positive for Serratia [6]. In our patient, he had a central catheter but had no sepsis, blood culture was negative for the organism, erythrocyte sedimentation rate (ESR) and C-reactive protein were increased, but could be attributed to his chronic condition; it is very unlikely he was in sepsis.
Furthermore, in a study conducted by Khanna et al., where they had studied the cause of increase in frequency of isolation of S. marcescens from hospitalized patients, it was reported that the resistance for amikacin (71.4%), cefotaxime (71.4%), and gentamicin (85.7%) were very high when compared to carbapenem group of drugs (14.3%) [5]. In a case report done by Stock et al., it was found that Serratia species are naturally resistant to penicillin G, macrolides, clindamycin, linezolid, glycopeptides, and quinupristin/dalfopristin, first-generation cephalosporins, nitrofurantoin, colistin, and tetracyclines [7,8]. In our patient as well, the patient developed resistance to amikacin and was started on meropenem. In another case report done by Chewakidakarn et al., their patient had sustained trauma to the right hip previously and was diagnosed as a pathological neck of femur fracture secondary to hematological malignancy and intra-operatively found pus within the joint cavity, whose culture yielded S. marcescens [9]. In our patient, the limb was externally rotated on presentation and radiographs showed undisplaced neck of femur subcapital type of fracture, but with no prior history of trauma, most likely would be caused due to pathological fracture secondary to ongoing CKD or S. marcescens infection but the hip joint aspirate did not yield any such growth even though the knee of the same limb had heavy growth of the same. In the case report done by Hadid et al., it was a case of chronic osteomyelitis of distal tibia with secondary septic arthritis of knee whose culture was positive for the same organism in an immunocompetent patient for whom multiple washouts of the joint with antibiotic impregnated beads and prolonged course of intravenous antibiotics was done and was under a very close follow-up periodically [10]. Similarly, in our patient, after the initial joint aspirate showed moderate growth, immediately intravenous antibiotics were started and later tailored according to the culture-sensitivity pattern, and surgical arthrotomy of the knee with synovectomy was done. For our patient, regular follow-ups for 2 months were done, and there was no recurrence of collection in the joint. Moreover, the patient underwent regular hemodialysis sessions lasting for 4 h 3 times a week, and his blood sugars and hypertension were maintained within the physiological limits. The patient is symptomatically better and has achieved 0–90° range of motion at the knee actively as well and recovering well. His range of motion at right hip is recovering and he is able to partially bear weight on the limb at the 2 month follow up.
Septic arthritis in an immunocompromised patient is a complication and is to be treated as an emergency. Furthermore, the causative organism of the same being a Gram-negative bacillus itself is a poor prognosis and would require prolonged treatment with antibiotics since their response is lower and complications such as ankylosis, secondary osteomyelitis, flexion contracture, chronic effusion, and recurrent infections are more common. Hence, prompt treatment with antibiotics based on culture sensitivity pattern, mainly Carbapenem group of drugs is found to be very effective. Surgical arthrotomy of the joint with synovectomy and debridement and irrigation of the joint is of paramount importance.
Septic arthritis due to S. marcescens is rare but severe in immunocompromised patients. Timely joint aspiration, targeted antibiotics, especially carbapenems, and surgical arthrotomy with synovectomy are key to effective management and preserving joint function.
References
- 1.Whitehead W. The “open method” in septic arthritis of the knee. Br Med J 1902;2:155. [Google Scholar | PubMed]
- 2.Olut A, Tosun S, Ari A, Şeker B, Erkan H, Altay T. Posttraumatic septic arthritis due to Serratia marcescens: Case report and review of literature. Mediterr J Infect Microb Antimicrob 1970;6:13. [Google Scholar | PubMed]
- 3.Serratia Marcescens. Serratia Marcescens - Infectious Disease and Antimicrobial Agents. Available from: https://www.antimicrobe.org/b26.asp [Last accessed on 2024 Aug 06]. [Google Scholar | PubMed]
- 4.Integrated Taxonomic Information System - Report. ITIS. Available from: https://www.itis.gov/servlet/singlerpt/singlerpt?search-topic=tsn&search-value=958620#null [Last accessed on 2024 Aug 06]. [Google Scholar | PubMed]
- 5.Khanna A, Khanna M, Aggarwal A. Serratia marcescens- a rare opportunistic nosocomial pathogen and measures to limit its spread in hospitalized patients. J Clin Diagn Res 2013;7:243. [Google Scholar | PubMed]
- 6.Mahmoud SS, Odak S, Qazzafi Z, McNicholas MJ. Primary total knee arthroplasty infected with Serratia marcescens. BMJ Case Rep 2012;2012:bcr2012006179. [Google Scholar | PubMed]
- 7.Stock I, Burak S, Sherwood KJ, Gruger T, Wiedemann B. Natural antimicrobial susceptibilities of strains of ‘unusual’ Serratia species: S. Ficaria, S. Fonticola, S. Odorifera, S. Plymuthica and S. Rubidaea. J Antimicrob Chemother 2013;51:865-85. [Google Scholar | PubMed]
- 8.Stock I, Grueger T, Wiedemann B. Natural antibiotic susceptibility of strains of Serratia marcescens and the S. Liquefaciens complex: S. Liquefaciens sensu stricto, S. Proteamaculans and S. Grimesii. Int J Antimicrob Agents 2003;22:35-47. [Google Scholar | PubMed]
- 9.Chewakidakarn C, Nawatthakul A, Suksintharanon M, Yuenyongviwat V. Septic arthritis following femoral neck fracture: A case report. Int J Surg Case Rep 2019;57:167-9. [Google Scholar | PubMed]
- 10.Hadid H, Usman M, Thapa S. Severe osteomyelitis and septic arthritis due to Serratia marcescens in an immunocompetent patient. Case Rep Infect Dis 2015;2015:347652. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Surgical and Functional outcome of Infective Knee Operated with Arthrotomy
March 1, 2026 Surgical and Functional outcome of Infective Knee Operated with Arthrotomy February 1, 2026 Case Report on Steroid-induced Bilateral Femoral Head Osteonecrosis with Concomitant Hip Septic Arthritis in Primary Membranous Nephropathy
February 1, 2026 Case Report on Steroid-induced Bilateral Femoral Head Osteonecrosis with Concomitant Hip Septic Arthritis in Primary Membranous Nephropathy January 1, 2026 From Hip Effusion to Hemophilia: Unveiling the Cause of Pain in 6-Month-Old Infant. A Case Report
January 1, 2026 From Hip Effusion to Hemophilia: Unveiling the Cause of Pain in 6-Month-Old Infant. A Case Report January 1, 2026 The Hidden Threat: Polyarticular Septic Arthritis Unmasking Disseminated Melioidosis
January 1, 2026 The Hidden Threat: Polyarticular Septic Arthritis Unmasking Disseminated Melioidosis