
Early diagnosis and individualized surgical management of bilateral tendoachilles xanthoma are crucial to preserve tendon function and prevent systemic complications, even in normolipidemic patients.
Dr. Akshay Seth, Department of Orthopaedics, Government Medical College, Patiala - 147001, Punjab, India. E-mail: drakshayseth@gmail.com
Introduction: Tendoachilles xanthoma is a very rare soft-tissue swelling encountered in orthopedic outpatient departments. An early diagnosis and intervention are crucial to prevent tendon dysfunction and systemic complications. Tendoachilles xanthoma, though uncommon, should be considered in patients with bilateral Achilles tendon thickening.
Case Report: We hereby present a rare case of a 33-year-old female with bilateral tendoachilles xanthoma who presented with complaints of swelling and pain in the bilateral lower leg region treated with surgical debulking. Monthly follow-up suggested fair healing, pain reduction, and maintained Achilles tendon function.
Conclusion: Bilateral tendoachilles xanthoma is a rare but important condition usually linked to lipid metabolism disorders, but can also occur in a normolipidemic state too. This case highlights the need for early diagnosis, multimodal treatment, and a personalized surgical approach to preserve tendon function. Long-term lipid control in disorders associated with deranged lipid profiles is useful in preventing recurrence and systemic complications.
Keywords: Achilles tendon xanthoma, tendon xanthoma, hyperlipidemia, cerebrotendinous xanthomatosis, familial hypercholesterolemia.
Tendoachilles xanthoma is a rare manifestation of hyperlipidemia-related disorders, commonly associated with familial hypercholesterolemia and cerebrotendinous xanthomatosis (CTX). A large tendinous xanthoma creates a dilemma in management due to the possible risk of tendon dysfunction on liberal excision of the pathology. A multidisciplinary approach involving orthopedic, radiology, and biochemical specialists is essential for optimal management. Bilateral tendoachilles xanthoma is a very rare clinical entity and is usually associated with genetic hyperlipidemic states. This case report highlights the rarity of presentation with no obvious underlying derangement in lipid profile, with the aim of gathering information necessary to devise a structured management protocol for the condition. The treatment methods used for the condition are variable, and there is no clear consensus regarding the treatment strategy for the condition.
A 33-year-old housewife presented to the orthopedic outpatient of a tertiary care center with complaints of swelling in the bilateral lower leg (posterior) region with no known co-morbidity. The patient first noticed swelling 5 years ago, which was insidious in onset and gradually increased in size. Initially, it was painless, but in the past 3 months, she had been experiencing pain while squatting, which was relieved by standing or taking oral medication. Examination findings of the patient showed fusiform swelling over the left and right Achilles tendon regions, measuring 10 × 3 cm and 8 × 3 cm, respectively (Fig. 1 and 2).
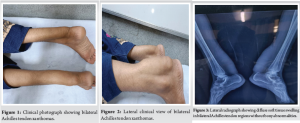
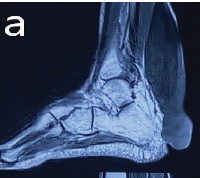
Bilaterally, the swelling was firm and adherent to the underlying Achilles tendon and was moving with the plantar flexion. The overlying skin showed no erythema or ulceration, no signs of inflammation. There was no local rise in temperature, tenderness, or any neurovascular compromise. The lipid profile of the patient did not show any derangement. The patient was sent for radiographs, which showed diffuse soft-tissue swelling without bony abnormalities or calcification bilaterally (Fig. 3). Ultrasonography (USG) yielded diffuse uniform thickening of tendons with loss of normal fibrillary architecture bilaterally. Magnetic resonance imaging (MRI) showed fusiform enlargement of the entire Achilles tendon on both sides, extending from the musculotendinous junction to the calcaneal insertion. The internal heterogeneity in the lower 1/3rd of the tendon was suggestive of a high-grade partial interstitial tear and underlying myxoid degeneration. Mild edema in the fat anterior to the Achilles tendon was also noted. The patient was planned for en masse resection of the swellings bilaterally and was taken to the operating theater. Intraoperatively, en masse resection was not found to be feasible, as the swelling was completely integrated with the Achilles tendon, with no clear interface between the tendon and the pathological tissue (Fig. 4-6).

The tendon showed hypertrophy with loss of normal tissue architecture, due to which debulking of the swelling was done, and tendon repair was done using the Krackow technique with Ethibond no. 5 suture, and closure was done in layers, and a below-knee backslab was applied for immobilization. Resected tissue (Fig. 7) was sent for histopathology examination, which showed a xanthomatous lesion with fibroconnective tissue with numerous foamy macrophages and giant cell reaction with cholesterol clefts.

Tendoachilles xanthoma is a rare presentation, often associated with lipid metabolism disorders such as familial hypercholesterolemia [1]. Our patient presented with fusiform swelling bilaterally in the Achilles region, which was firm, adherent to the tendon, and moved with plantar flexion. The overlying skin showed no erythema or ulceration, and there was no neurovascular compromise, which is consistent with previous reports by Watanabe et al. [2] Unlike classic tendoachilles xanthomas, which are commonly associated with hyperlipidemia, our patient had a normal lipid profile. This aligns with findings by Kumar et al., who reported that lipid profile abnormalities may not always be present, suggesting the possibility of localized metabolic dysregulation within tendons [3]. Diffuse soft-tissue swelling without bony abnormalities or calcification was noted in our case, which showed similar results in the literature, with many cases showing tendon thickening but no bony changes [4]. USG in the case depicted diffuse uniform thickening of tendons with loss of normal fibrillary architecture, which were similar to those described in Chauhan et al. [5] The presence of foamy macrophages, giant cell reaction, and cholesterol clefts confirmed the diagnosis of tendoachilles xanthoma. Similar histological findings have been described by Patel et al. [6] reinforcing the role of biopsy in confirming diagnosis. MRI showed fusiform enlargement, extending from the musculotendinous junction to the calcaneal insertion, with high-grade partial interstitial tear and myxoid degeneration. MRI findings typically show tendon hypertrophy with heterogeneity, consistent with chronic xanthomatous infiltration [7]. Due to the extent of the lesion, en masse resection was not feasible, necessitating debulking with tendon repair using the Krackow technique. Most cases in the literature advocate for subtotal or complete resection with tendon reconstruction [8]. Similar cases of bilateral Achilles tendon xanthomas have been reported with varied treatment approaches and outcomes. Saha et al. described subtotal resection of bilateral xanthomas combined with statin therapy, which led to cosmetically and functionally favorable results without recurrence over 2 years [9]. Şahin et al. reported a case of CTX treated with chenodeoxycholic acid, although neurological manifestations such as spastic gait and paraparesis persisted [10]. Ergun et al. performed bilateral resection of Achilles tendon xanthomas followed by reconstruction using a vascularized iliotibial tract flap, achieving good functional outcomes and no pain over a 9-year follow-up [11]. Barkhof et al. highlighted the role of early diagnosis and genetic confirmation in CTX, where biochemical and genetic studies guided medical therapy, resulting in significant symptomatic improvement [12]. These cases emphasize the necessity of individualized treatment plans based on clinical presentation, imaging findings, and underlying metabolic derangements. Our case aligns with these recommendations but highlights the challenge of surgical excision due to integration of the lesion with the tendon fibers. The review of previously published literature is summarized in Table 1.

Bilateral tendoachilles xanthoma is a rare but important condition linked to lipid metabolism disorders. This case presents an unusual female patient with a normolipidemic tendoachilles xanthoma, emphasizing the importance of considering this diagnosis even in the absence of dyslipidemia. The surgical challenge of tendon involvement necessitates individualized management strategies. Our case highlights the need for early diagnosis, multimodal treatment, and a personalized surgical approach to preserve tendon function. Still, there is a lot of literature gap in the management of tendon xanthoma. Further studies are needed to explore alternative pathophysiological mechanisms for normolipidemic xanthomas.
Treatment for tendoachilles xanthoma should be tapered according to the clinical symptomatology of the patient, and a multidisciplinary approach should be used for early diagnosis, multimodal treatment, and a personalized surgical approach to preserve tendon function and to detect and treat the underlying dyslipidemic state, which might lead to other systemic derangements.
References
- 1. Khatoon HM, Srirambhatla A, Sharma A, Sankepally P, Arora AJ. An unusual case of xanthoma of bilateral Achilles tendon with gouty infiltration: A rare case report. Indian J Radiol Imaging 2023;33:403-8. [Google Scholar] [PubMed]
- 2. Watanabe M, Kubo S, Nishida K. Achilles tendon xanthomas in familial hypercholesterolemia: A review of clinical cases. Lipid Disord J 2020;8:125-32. [Google Scholar] [PubMed]
- 3. Kumar S, Jain R, Bose S. Normolipidemic Achilles tendon xanthomas: A diagnostic dilemma. Indian J Orthop 2019;53:789-94. [Google Scholar] [PubMed]
- 4. Morris D, Lee C, Patel R. Tendinous xanthomas: Clinical and radiographic correlation. Radiol Case Rep 2017;12:415-20. [Google Scholar] [PubMed]
- 5. Chauhan R, Verma S, Malhotra K. Ultrasonographic features of Achilles tendon xanthomas. J Radiol Imaging 2021;15:200-5. [Google Scholar] [PubMed]
- 6. Patel H, Rao N, Desai S. Histopathology of Achilles tendon xanthomas: A retrospective review. J Pathol 2022;18:98-104. [Google Scholar] [PubMed]
- 7. Gupta A, Mehta P, Singh K. MRI characteristics of Achilles tendon xanthomas in hyperlipidemic and normolipidemic patients. Eur J Musculoskelet Imaging 2020;12:45-52. [Google Scholar] [PubMed]
- 8. Garg P, Khanna V, Mishra A. Surgical management of Achilles tendon xanthomas: A case series. Orthop Surg J 2019;10:135-40. [Google Scholar] [PubMed]
- 9. Saha M, Bhowmik A, Das M, Biswas D, Ghosh S. Subtotal resection of bilateral Achilles tendon xanthomatosis: A case report and review of literature. Cureus 2021;13:e16555. [Google Scholar] [PubMed]
- 10. Şahin A, Gökçay G, Erdoğan S, Gökçay E. Cerebrotendinous xanthomatosis: Diagnostic delay and missed opportunities for treatment. J Pediatr Neurosci 2021;16:131-4. [Google Scholar] [PubMed]
- 11. Ergun T, Lakadamyali H, Derincek A. Bilateral Achilles tendon reconstruction using vascularized iliotibial band flap following xanthoma excision: 9-year follow-up. Cureus 2023;15:e51818. [Google Scholar] [PubMed]
- 12. Barkhof F, Verrips A, Wesseling P, Van Der Knaap MS, Van Engelen BG. Cerebrotendinous xanthomatosis: Variety of MR appearances. AJNR Am J Neuroradiol 2000;21:1489-96. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Massive Tendo Achilles Xanthoma Treated with en bloc Excision and Reconstruction with Flexor Hallucis Longus Tendon Transfer: A Case Report
September 1, 2025 Massive Tendo Achilles Xanthoma Treated with en bloc Excision and Reconstruction with Flexor Hallucis Longus Tendon Transfer: A Case Report May 1, 2025 A Rare Case of Bilateral Xanthomatosis of Tendon of Achilles: A Case Report
May 1, 2025 A Rare Case of Bilateral Xanthomatosis of Tendon of Achilles: A Case Report May 10, 2024 Reviewers Acknowledgement & Photo Gallery May 2024
May 10, 2024 Reviewers Acknowledgement & Photo Gallery May 2024 April 10, 2022 Progressive Kyphosis Deformity with Facet Subluxation after Cervical Expansive Laminoplasty: A Case Report
April 10, 2022 Progressive Kyphosis Deformity with Facet Subluxation after Cervical Expansive Laminoplasty: A Case Report