
While performing the extraction of large fetuses with malpresentation in Cesarean Section, the Obstetrician should be vigilant for the development of any long bone fractures in neonates.
Dr. Nadeem Akhtar Qureshi, Department of Orthopedics, Futela Hospital, Rudrapur - 263153, Uttarakhand, India. E-mail: drnaq1308@gmail.com
Introduction: Neonatal Obstetric fractures are rare birth injuries that newborns sustained from trauma during delivery and birth process. Long bone fractures are common in vaginal breech deliveries. A cesarean section is considered a relatively safe and preferred mode of delivery of breech fetuses to prevent birth trauma and decrease the risk of fetal head entrapment; nevertheless, it can lead to femur fracture in newborn rarely.
Case Report: A 3915 g male child born at 38 weeks and 4 days of gestation to a primigravida aged 31 years by emergency Lower Segment Cesarean Section for Premature Rupture of Membrane with breech presentation. During extraction, the newborn sustained a fracture to his right femur shaft. X-rays confirmed the diagnosis. The fracture was treated successfully with a toe-groin cast for 25 days with complete healing.
Conclusion: As compared to vaginal breech delivery, cesarean section reduces the risk of traumatic birth injuries; however, it does not completely eliminate the possibility of birth injuries and long bone fractures in newborns. Orthopedic opinion must be sought, if the obstetrician and neonatologist suspect any birth trauma in difficult deliveries. Immobilization of the limb leads to complete healing of the fracture without any sequel.
Keywords: Neonatal obstetric fractures, cesarean section, breech presentation, birth injuries, femur fracture in newborn.
Breech presentation of fetuses accounts for 3–4% term pregnancies [1]. An incidence of 0.1% and 0.5% of long bone fractures among neonates born through cesarean section and vaginal delivery has been reported [1]. Vaginal breech delivery accounts for three-quarters of birth-related long bone fractures in newborns [2], fracture femur being the majority among them [3]. Thus, a cesarean section is considered to be safer and a common method of delivering a breech fetus in reducing birth-related fractures [4]. A large fetus, breech presentation, and a difficult delivery in a primigravida during cesarean section are associated with risk factors for birth-related femur fracture [5,6]. The risk of long bone fractures in a newborn is higher in emergency cesarean sections than in vaginal deliveries [7]. Although rare, case reports [2,3,4,5,6,7,8,9] and case series [10,11,12,13,14] of obstetric fractures involving the femur in neonates born through cesarean section for breech have been reported. We report a case of obstetric right femur fracture in a Large for gestational age baby born to a primigravida through cesarean section done in emergency for breech presentation.
A 31-year-old booked primigravida, with regular and normal antenatal care clinics, presented in the emergency room with premature rupture of membrane (PROM) with breech presentation at 38 weeks and 4 days period of gestation, underwent emergency cesarean section. She had normal initial antenatal scans. Her medical history was insignificant and negative for diabetes, hypertension, or any previous uterine surgery. The patient was offered Spinal anesthesia. An appropriate wider incision was made at the lower uterine segment. The fetus was extracted after catching hold of footling, extending and rotating the lower limbs to align the fetal pelvis anteroposteriorly, followed by application of fundal pressure on the uterus to deliver the rest of the baby with lateral flexion. The delivery was difficult due to the large size of the fetus and anhydroamnios secondary to PROM, a force was applied for the rotation of the limbs. However, the operating surgeon and assisting nurse didn’t hear any “crack” or “snap” during extracting the fetus. A 3915 g male infant, large for gestational age, was delivered and cried after birth. APGAR scores at 1 and 5 min were 8 and 9, respectively. On examination, the attending pediatrician noticed diffuse swelling and deformity in the right mid-thigh, restricted right leg movements, and excessive cry on palpation, which raised a high suspicion of a fracture shaft of the right femur in the neonate. A thorough clinical examination revealed no other abnormalities. An immediate orthopedic consultation was done. The right thigh was found to be swollen, externally rotated and shortened; bony crepitus of the femur was palpable with painful passive movements. Distal pulsations were intact. Anteroposterior and lateral view X-rays of the right thigh revealed a displaced spiral fracture of the middle-third shaft femur (Fig. 1). Bone structure and mineralization appeared normal. There was no blue sclera, other bone fractures or limb deformity, thus any possibility of osteogenesis imperfecta was ruled out. The baby’s right lower limb was immobilized with a 90–90 posterior splint and shifted to the neonatal intensive care unit. Paracetamol drops (12 mg/kg) three times a day was advised for pain relief. Parents were informed of this untoward complication and counseled.
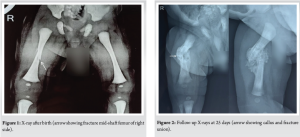
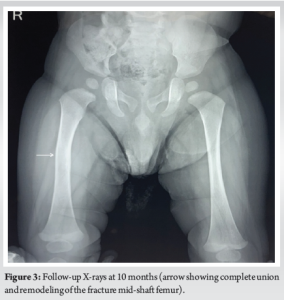
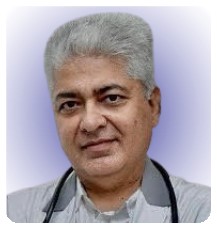
The next day, the baby was handed over to the mother and was kept on breastfeeding. After 5 days post-operative, both the mother and neonate were discharged and reviewed in the orthopedic outpatient department after 1 week, when the posterior splint was replaced with a toe-groin cast for another 2 weeks. On follow-up on the 25th day, a repeat X-ray showed abundant callus between fracture ends, and the cast was removed (Fig. 2). Clinical examination revealed no local tenderness and deformity with active, painless movements of both limbs, thus completing the treatment. At follow-up after 10 months, repeat X-ray shows complete healing of the fracture with no deformity and visible limb length discrepancy of the limb (Fig. 3).
Clavicle, humerus, and femur are the common sites of obstetric fracture [3]. Neonatal obstetric fracture involving the femur is rare [2,10] and represents the commonest lower limb fracture in them [3]. Pavone et al. reported birth-related fracture femur incidence of 0.89/1000 live births [11], which is slightly higher than the previously reported incidence of 0.17/1000 live births [12]. Various risk factors associated with femur fractures during cesarean section have been mentioned in literature, namely, large fetus with difficult extraction [3,10], preterm birth [8], prematurity [6], twin or multiple pregnancies [6,7], low birth weight, breech presentation or obstructed labor, osteogenesis imperfecta, disuse osteoporosis following immobilization and osteopenia of prematurity [10], malpresentation and abnormal lie [7], uterine fibroid [5,7]. Farikou et al. concluded that cesarean section for breech, primiparity, advance age of mother, and obstetric maneuvers as predisposing factors for femur fractures in newborn [5]. Kancherla et al. and Givon et al. reported 60% and 73% femur fractures in cesarean deliveries, respectively [10,13]; Toker et al. reported 70% birth-associated femoral fractures in babies born through cesarean section, and thus concluded that the risk of long bone fractures during birth markedly increases in cesarean section [14]. While spiral fracture of the mid-shaft femur is reported to be the most common pattern of injuries [5,10,12,13,14], others reported proximal-third or subtrochanteric femur fracture [3,6,7,11]. Application of sudden, forced, and excessive traction along with twisting and/or pulling maneuvers on the leg while delivering the fetus during cesarean section, produces torsional forces, which results in spiral fracture of the femur in newborns [10,15]. Small uterine incision providing limited space for maneuvering of the fetus during delivery, inadequate relaxation [10], and poor delivery techniques, such as improper handling of the fetus by one thigh during delivery of shoulders and arms, may result in birth fractures during cesarean section [6]. Thus, Jain and Belenski proposed avoiding traction on the extremities and making an appropriate extension of the uterine incision for smooth delivery of the babies in Cesarean section [15]. Capobianco et al. proposed a set of rules to prevent birth-related fractures in cesarean section, namely, adequate analgesia, application of delicate traction, and use of wider uterine incision for smooth extraction of fetus [9]. Large fetus with anhydroamnios secondary to PROM caused difficult extraction of the fetus, thus necessitating the application of force for rotating the limbs, which might have caused a fracture femur in our case. Management is mostly non-operative [8]. The choice of treatment adopted can vary according to the treating physician; however, the basic principle is strict immobilization of the fracture [10]. Common and recommended treatment methods reported in orthopedics literature for neonatal femur fracture include: Bryant’s skin traction [13], Gallow’s traction, Pavlik harness [12], toe-groin cast [10] or Hip-Spica cast [3,5,8], thigh to leg strapping [7] or thigh to abdomen strapping [6,10] and Splinting of the limb [15]. All treatment methods reported union in 3 weeks [13] to 4 weeks [10] without any complication, residual deformity, or limb length discrepancy, suggesting a good prognosis of birth-related long bones fractures in long-term follow-up [10,13]. A characteristic “crack” sound heard or felt during difficult extraction of newborn in cesarean section is pathognomic of birth fractures [9], and helps clinician to detect, diagnose early and to execute prompt management of fracture without any delay; however, cases of obstetric femur fractures have been reported where no crack was heard [4,6]. In our case, the crack was also not heard by the obstetrician during the extraction of the fetus and the diagnosis of a fracture femur was made clinico-radiologically by the attending pediatrician and orthopedician. The fracture involved the middle third of the shaft femur and was spiral. We adopted initial posterior splinting of the limb followed by a toe-groin cast, with a total of 25 days of immobilization, until the fracture becomes sticky and callus appears, resulting in complete healing of the fracture. From a medico-legal point of view, it is important to exclude the possibility of child abuse while evaluating neonatal fractures and birth injuries in newborns in case of delayed presentation to the clinician [4]. Parent’s counseling and building-up confidence in the mother is important. They should be explained regarding the good prognosis and complete healing of the fracture in the newborn without any sequel. She should be taught to carry out proper care and follow-up of the baby until the treatment gets completed. Although femur fracture in newborn during cesarean section is rare and relatively uncommon injury [3,5], a history of cesarean section does not rule out the possibility of a fracture [15]. Thus, neonates delivered in an emergency by cesarean section for breech presentation should be carefully evaluated by the attending pediatrician and monitored after birth [4] and a radiograph of the suspected limb must be sought.
Cesarean section in breech is safe in reducing the risk of skeletal birth injuries in newborns, although it never completely eliminates the possibility of long bone fractures. An obstetrician should be vigilant while performing an abdominal delivery of a breech in an emergency. Identifying high-risk mother and fetus, appropriate surgical techniques, and a high index of suspicion in neonates following difficult extraction of large fetuses in cesarean section, are effective in reducing the incidence of long-bone fractures in newborns. Obstetric neonatal fracture of long bone has an excellent prognosis and shows complete healing following immobilization without any sequelae.
Although rare, neonatal birth injuries involving long bone fractures can occur during cesarean section with malpresentation, which can be prevented by careful fetus extraction by an obstetrician. These fractures have an excellent prognosis and heal completely with conservative management.
References
- 1. Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willian AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: A randomized multicenter trial. Term breech trial collaborative group. Lancet 2000;356:1375-83. [Google Scholar] [PubMed]
- 2. Papi L, Gori F, Turco S, Perutelli A. Femoral fracture during cesarean section: A case of professional liability? Case presentation and review of the literature. Arch Clin Med Case Rep 2019;3:242-9. [Google Scholar] [PubMed]
- 3. Vasa R, Kim MR. Fracture of the femur at cesarean section: Case report and review of literature. Am J Perinatol 1990;7:46-8. [Google Scholar] [PubMed]
- 4. Kanai Y, Honda Y, Honda T, Sanpei M. Delayed birth-related femur fracture after cesarean section: A case report. AJP Rep 2018;8:e158-60. [Google Scholar] [PubMed]
- 5. Farikou I, Bernadette NN, Daniel HE, Aurelien SM. Fracture of the femur of a newborn after cesarean section for breech presentation and fibroid uterus: A case report and literature review. J Orthop Case Rep 2014;4:18-20. [Google Scholar] [PubMed]
- 6. Singla S, Sharma R, Sharma R, Bawa RS, Singh A, Sidhu NS, et al. Subtrochanteric femur fracture in neonates: A rare complication after breech presentation. J Orth Joint Surg 2020;2:79-81. [Google Scholar] [PubMed]
- 7. Vellingiri K, Venkataraman S, Shanthappa AH, Seenappa H. Femur shaft fracture in newborns: A report of two cases. Cureus 2021;13:e12504. [Google Scholar] [PubMed]
- 8. Bombah FM, Ngalame A, Essomba R, Boukar YE, Nkoa EZ, Eone DH. Obstetric fracture of the femur during cesarean section in a preterm baby: A case report. J Orthopedics and Orthopedic Surg 2021;2:22-4. [Google Scholar] [PubMed]
- 9. Capobianco G, Virdis G, Lisai P, Cherchi C, Biasetti O, Dessole F, et al. Cesarean section and right femur fracture: A rare but possible complication for breech presentation. Case Rep Obstet Gynecol 2013;2013:613709. [Google Scholar] [PubMed]
- 10. Kancherla R, Sankineani SR, Naranje S, Rijal L, Kumar R, Ansari T, et al. Birth-related femoral fracture in newborns: Risk factors and management. J Child Orthop 2012;6:177-80. [Google Scholar] [PubMed]
- 11. Pavone V, Vescio A, Montemagno M, De Cristo C, Lucenti L, Pavone P, et al. Perinatal femoral fracture: A ten-year observational case series study. Children (Basel) 2020;7:156. [Google Scholar] [PubMed]
- 12. Morris S, Cassidy N, Stephens M, McCormack D, McManus F. Birth-associated femoral fractures: Incidence and outcome. J Pediatr Orthop 2002;22:27-30. [Google Scholar] [PubMed]
- 13. Givon U, Sherr-Lurie N, Schindler A, Blankstein A, Ganel A. Treatment of femoral fractures in neonates. Isr Med Assoc J 2007;9:28-9. [Google Scholar] [PubMed]
- 14. Toker A, Perry ZH, Cohen E, Krymko H. Cesarean section and the risk of fractured femur. Isr Med Assoc J 2009;11:416-8. [Google Scholar] [PubMed]
- 15. Jain R, Bielski RJ. Fracture of lower femoral epiphysis in an infant at birth: A rare obstetrical injury. J Perinatol 2001;21:550-2. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2025 Intra-Ligamentous Pigmented Villonodular Synovitis of the Anterior Cruciate Ligament, a Case Report
April 1, 2025 Intra-Ligamentous Pigmented Villonodular Synovitis of the Anterior Cruciate Ligament, a Case Report May 6, 2019 Reviewers Acknowledgement & Photo-gallery May-June 2019
May 6, 2019 Reviewers Acknowledgement & Photo-gallery May-June 2019 December 10, 2023 Neglected Elbow Dislocation leading to Ankylosis of Elbow: A Case Report
December 10, 2023 Neglected Elbow Dislocation leading to Ankylosis of Elbow: A Case Report July 10, 2023 Case Report of an Osteochondral Lesion of the First Metatarsal Head in an Adolescent Patient Treated by Autograft Mosaicplasty: Surgical Technique and Decision-Making Rationale
July 10, 2023 Case Report of an Osteochondral Lesion of the First Metatarsal Head in an Adolescent Patient Treated by Autograft Mosaicplasty: Surgical Technique and Decision-Making Rationale