
Heterotopic ossification is a rare but important post-TKR complication that can impair mobility and requires early detection and appropriate management for better outcomes.
Dr. M S Karthik, Department of Arthroplasty, Sanjay Gandhi Institute of Trauma and Orthopedics, Bengaluru, Karnataka, India. E-mail: drkarthikms1@gmail.com
Introduction: Heterotopic ossification (HO) is a rare complication following total knee replacement (TKR), with an incidence ranging between 1% and 3%. This condition can lead to significant functional limitations, including immobility and pain, particularly when ossification impinges on adjacent structures.
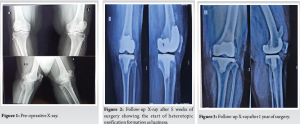
Case Report: We report the case of a 67-year-old female with grade 4 osteoarthritis of the left knee who underwent TKR following the failure of conservative management. Postoperatively, the patient developed stiffness and a reduced range of motion. Radiographic imaging at 5 weeks showed haziness in the anterior aspect of the femur at the upper border of the femoral implant, with gradual progression to distinct ossification by 3 months.
Results: The heterotopic bone formation was found to impinge on the quadriceps mechanism, limiting knee flexion but not preventing full extension. Conservative management involving physiotherapy and analgesics was pursued, and surgical excision was avoided initially. Over 1 year, the patient showed improvement in extension, although no significant improvement in flexion was observed. Surgical excision of the heterotopic bone was performed at the end of 1 year, followed by post-operative radiotherapy to prevent recurrence.
Conclusion: This case underscores the rarity of HO following TKR, particularly when it involves the quadriceps mechanism. It highlights the importance of early detection, close monitoring, and a stepwise treatment approach – starting with conservative therapy and escalating to surgical intervention when necessary. Post-operative radiotherapy can be considered in select cases to minimize recurrence.
Keywords: Heterotopic ossification, total knee replacement, quadriceps mechanism, knee stiffness, conservative management, surgical excision, radiotherapy.
Osteoarthritis (OA) is a chronic, progressive degenerative joint disease characterized by cartilage degradation, subchondral bone remodeling, and joint inflammation [1]. It is one of the leading causes of disability among the elderly, significantly affecting mobility and quality of life [2]. Grade 4 OA represents, according to the Kellgren–Lawrence classification, the most advanced stage of the disease, consisting of severe joint space narrowing with extensive osteophyte formation, subchondral sclerosis, and gross deformity [3]. Advanced OA, particularly grade 4, where the joint is destroyed, is treated by total knee replacement (TKR), which is the gold standard surgical treatment. Indications for TKR include intractable severe pain after conservative treatment, significant functional loss, such as inability to walk or climb stairs or perform activities of daily living, and significant deformities, including varus or valgus alignment [4]. The end result is to make the patient’s quality of life as pain-free, stable, and functional as a knee joint can be. Heterotopic ossification (HO) is an abnormal bone formation in non-osseous tissues, often following traumas, surgeries, or long immobilizations [5]. Although HO is more commonly documented following hip arthroplasty or spinal injuries, its incidence following TKR is very rare, estimated between 1% and 3% [6]. HO may result in sometimes serious complications, such as restricted joint movement and pain due to its size, location, and extent, although most cases are asymptomatic [5]. In the context of TKR, HO can pose additional challenges to patients by either interfering with prosthetic function or, as in this case, by impinging on adjacent structures such as the quadriceps mechanism.
A 67-year-old female with a history of advanced OA of both knees, the left more so than the right. The patient had worsening pain and impairment in function for the past 2 years, making it increasingly difficult for her to squat or sit cross-legged, as well as perform her daily activities. The patient had no relevant medical history, no previous surgeries, and no known risk factors for HO. The patient’s clinical and radiological evaluation confirmed grade 4 OA of the left knee, necessitating TKR (Fig. 1). Conservative management, including analgesics and physiotherapy, had failed to provide adequate symptom relief, prompting the decision to proceed with surgery.
Surgical procedure
A routine left TKR was performed on the patient. An initial midline incision and median parapatellar approach were conducted to expose the joint for surgery. Bone cuts were done in appropriate alignment using the Freedom Series Prosthesis Maxx, with all components designed to restore biomechanics in the knee. Proper soft-tissue balance, along with appropriate ligament tension, was exercised. The prosthesis was fixed in place with bone cement. The surgery was without complications, with no intraoperative complications.
Post-operative course
Initial post-operative recovery was uneventful, and the patient was discharged on standard rehabilitation protocol. However, at 3 weeks of follow-up, the patient started developing stiffness and reduced range of motion (ROM). Physical examination confirmed these limitations, and an X-ray taken at 5 weeks post-surgery revealed the initial hazy appearance of HO formation in the distal femur (Fig. 2). At the 3-month follow-up, the HO had progressed, and there was evidence of distinct radiographic ossification. The resulting abnormal bone growth was noted to impinge on the quadriceps mechanism, further restricting flexion at the knee. These findings notwithstanding, however, the patient could achieve full knee extension.
Diagnosis of HO
The HO was diagnosed based on radiographic findings at 5 weeks and 3 months postoperatively, with the ossification origin in the distal femur. Impingement of the HO on the quadriceps mechanism was identified as a main cause of restricted flexion and occasional pain.
Treatment and outcome
The patient underwent conservative management with regular physiotherapy to maintain joint mobility and analgesics for pain relief. Surgical excision of the ossified tissue was not performed to allow HO to mature. Gradual improvement in knee function over the following months was observed. At 1-year follow-up, full knee extension was obtained; however, restricted flexion was present with no significant improvement observed (Fig. 3 and 4). The patient was advised to undergo excision at the end of 1 year. Following excision, radiotherapy with a single cycle of 75cGy was given in the immediate post-operative period. Chemoprophylaxis with indomethacin 75 mg given once daily for 3 months and discontinued. The wound healed well, and the patient showed symptomatic improvement with a 20° increase in ROM during the initial post-operative period (Fig. 5). At 8 months post-excision, there is no radiographic evidence of recurrence (Fig. 6), and the range of knee flexion has further improved to 80°. The patient remains symptomatically more comfortable following the excision.



HO is the development of bone in tissues where it normally does not develop and, often, after surgical trauma, inflammation, or local tissue injury [5]. In TKR, surgical manipulation, disruption of the periosteum, and soft-tissue trauma can all set up an environment for ectopic bone formation, primarily through osteoinductive factors such as bone morphogenetic proteins and inflammatory cytokines. HO occurrence after TKR is less common, with the reported prevalence from 1% to 3%. The patient had limited knee flexion and pain on occasion from the HO impinging against the quadriceps mechanism, an extremely rare and unusual complication. Most patients have asymptomatic or very mild stiffness post-TKR, so this presentation was unique. Without identifiable predisposing factors, such as prior HO, trauma, or systemic conditions, the patient had severe functional limitations that demonstrate the unpredictable behavior of HO. Early detection is key in the management of HO, and this was exemplified by the progressive imaging findings in this case. There was a hazy appearance at 5 weeks post-onset that progressed to well-formed ossification at 3 months. These findings underscore the value of routine post-operative follow-up to detect complications early and intervene appropriately. Conservative management strategies range from physiotherapy, analgesics, and/or medications such as indomethacin or bisphosphonate to maintain mobility of the joint as well as limit further ossification [7]. Prophylactic radiotherapy offers a potential option to inhibit further ossification, but its application post-diagnosis remains debated. Current evidence supports its use within a narrow window-either preoperatively or immediately postoperatively-rather than after ossification has formed [8]. Immediate surgical excision of HO diagnosed early is generally not recommended, as immature ossification carries a higher risk of recurrence and bleeding. Waiting for the ossification to mature, typically over 6–12 months, allows for better demarcation of the mass and reduces the risk of surgical complications. Surgical excision is best reserved for cases of mature HO that cause significant pain or functional limitations, as it provides better outcomes and minimizes recurrence risks [9]. In this case, operative treatment was effective after a period of 1 year, so that the patient could obtain satisfactory recovery with full extension and increased flexion compared to pre-operative status (Fig. 5 and 7).

The rarity of HO post-TKR and its unusual involvement of the quadriceps mechanism have limited similar reports in the literature. Massaro et al. [10] emphasized the importance of early detection and individualized management strategies, whereas Zhang et al. [11] demonstrated the efficacy of arthroscopic debridement in improving ROM and knee function in symptomatic cases.
This case underscores the importance of vigilance in post-operative care following TKR, particularly for identifying rare complications such as HO. Routine imaging, patient education, and adherence to rehabilitation protocols are essential to optimizing outcomes. The rarity of this complication, especially with quadriceps impingement, highlights the need for awareness among clinicians to ensure timely diagnosis and tailored management.
Heterotopic ossification, though rare after total knee replacement, can significantly impair knee flexion when it involves the quadriceps mechanism. Early recognition through routine post-operative imaging and a stepwise approach – beginning with conservative management and escalating to surgical excision when needed – is key to optimizing functional outcomes. Post-operative radiotherapy may help prevent recurrence in selected cases.
References
- 1.Di Nicola V. Degenerative osteoarthritis a reversible chronic disease. Regen Ther 2020;15:149-60. [Google Scholar | PubMed]
- 2.Hawker GA, King LK. The burden of osteoarthritis in older adults. Clin Geriatr Med 2022;38:181-92. [Google Scholar | PubMed]
- 3.Kohn MD, Sassoon AA, Fernando ND. Classifications in brief: Kellgren-Lawrence classification of osteoarthritis. Clin Orthop Relat Res 2016;474:1886-93. [Google Scholar | PubMed]
- 4.Dieppe P, Basler HD, Chard J, Croft P, Dixon J, Hurley M, et al. Knee replacement surgery for osteoarthritis: Effectiveness, practice variations, indications and possible determinants of utilization. Rheumatology (Oxford, England) 1999;38:73-83. [Google Scholar | PubMed]
- 5.Dai GC, Wang H, Lu PP, Li YJ, Gao YC, Shi L, et al. Heterotopic mineralization (ossification or calcification) in aged musculoskeletal soft tissues: A new candidate marker for aging. Ageing Res Rev 2024;95:102215. [Google Scholar | PubMed]
- 6.Dalury DF, Jiranek WA. The incidence of heterotopic ossification after total knee arthroplasty. J Arthroplasty 2004;19:447-52. [Google Scholar | PubMed]
- 7.Subbarao JV, Garrison SJ. Heterotopic ossification: Diagnosis and management, current concepts and controversies. J Spinal Cord Med 1999;22:273-83. [Google Scholar | PubMed]
- 8.Ayers DC, Pellegrini VD Jr., Evarts CM. Prevention of heterotopic ossification in high-risk patients by radiation therapy. Clin Orthop Related Res 1991;263:87-93. [Google Scholar | PubMed]
- 9.Kaplan FS, Glaser DL, Hebela N, Shore EM. Heterotopic ossification. J Am Acad Orthop Surg 2004;12:116-25. [Google Scholar | PubMed]
- 10.Massaro M, Mela F, Esposito R, Maiorano E, Laskow G. Severe quadriceps heterotopic ossification after knee revision arthroplasty in a 42-year-old suffering from rheumatoid arthritis: A case report. Osteology 2022;2:161-5. [Google Scholar | PubMed]
- 11.Zhang DL, Zhang W, Ren YM, Zhao WJ, Sun HJ, Tian ZW, et al. Arthroscopic debridement improves range of motion for heterotopic ossification after total knee replacement: A retrospective cohort study. Sci Rep 2024;14:5882. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 January 3, 2019 Spinal Cord Injury Due to Cervical Disc Herniation without Bony Involvement Caused by Wrestling – A Case Report
January 3, 2019 Spinal Cord Injury Due to Cervical Disc Herniation without Bony Involvement Caused by Wrestling – A Case Report August 1, 2025 Histological Dedifferentiation in Recurrent Adamantinoma of the Tibia: A Case Report
August 1, 2025 Histological Dedifferentiation in Recurrent Adamantinoma of the Tibia: A Case Report July 1, 2025 Isolated Distal Ulna shaft fracture with Distal Radioulnar Joint dislocation or Reverse Galeazzi Pattern: A Case Report with Literature Review
July 1, 2025 Isolated Distal Ulna shaft fracture with Distal Radioulnar Joint dislocation or Reverse Galeazzi Pattern: A Case Report with Literature Review February 1, 2026 Deformity Correction in Ankylosing Spondylitis with Cervical Fracture: A Case Report
February 1, 2026 Deformity Correction in Ankylosing Spondylitis with Cervical Fracture: A Case Report