
Single-stage hybrid fixation offers an effective and safe solution for complex open trimalleolar ankle fractures with syndesmotic injury and posterior talar subluxation, promoting early stability and functional recovery.
Dr. Jeff Walter Rajadurai OR, Department of Orthopaedics, Madha Medical College and Research Institute, Chennai, Tamil Nadu, India. E-mail: jeffy.walter@gmail.com
Introduction: Trimalleolar ankle fractures, which involve syndesmotic damage and talar subluxation, are serious injuries that are complicated by open wounds. This article describes a novel single-stage hybrid fixation strategy designed to address these issues.
Case Report: A 65-year-old female was involved in a car accident and suffered a Grade IIIA open trimalleolar fracture-dislocation. Radiographs confirmed the syndesmotic disruption and posterior talar subluxation. She underwent emergency surgery that included open reduction and internal fixation of the medial and lateral malleoli, as well as the use of an ankle-spanning external fixator. Her surgical recovery went smoothly, with fast union and functional mobility restored.
Conclusion: This case shows that single-stage hybrid fixation can be a stable and successful approach for treating severe open ankle fractures with various anatomical disturbances.
Keywords: Ankle injuries, fracture fixation, external fixators, syndesmotic injuries, open wounds.
Trimalleolar ankle fractures are high-energy injuries involving disruption of the medial, lateral, and posterior malleoli. These fractures are frequently associated with posterior talar displacement and syndesmotic injury, which together can destabilize the ankle mortise and impair long-term function [1-3]. The management becomes more complex when the injury is open, particularly in Gustilo–Anderson Grade IIIA cases, where soft tissue compromise and infection risk pose significant challenges to definitive fixation [2]. Posterior malleolar fixation has been shown to contribute significantly to syndesmotic stability, reducing the need for additional hardware such as trans-syndesmotic screws [1,3]. In parallel, the role of hybrid fixation – combining internal hardware with external stabilization – is being explored in complex cases to simultaneously achieve mechanical stability and soft tissue preservation [4,5]. While some reports advocate staged fixation in such injuries [6], this approach may delay functional recovery and increase exposure to surgical morbidity. Therefore, a single-stage hybrid approach offers a potential solution for select patients by addressing both osseous and soft-tissue challenges in one surgical event. This report presents a case of an open trimalleolar fracture-dislocation with syndesmotic disruption and posterior talar subluxation, managed successfully using a novel single-stage hybrid fixation technique.
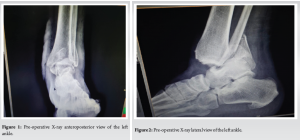
A 65-year-old previously healthy female was brought to the emergency room after a high-speed motor vehicle collision. She suffered an isolated right ankle injury with no history of trauma, systemic illness, or medication. She was a non-smoker with no comorbidities who worked in manual jobs. When the patient arrived, her right ankle was clearly deformed, with a 6 cm open wound across the medial malleolus and exposed bone. The ankle was unstable and had aberrant movement. There was no distal neurovascular impairment, and the capillary refill was intact. No symptoms of compartment syndrome were found. The injury was categorized as a Grade IIIA open fracture using the Gustilo–Anderson system. The initial plain radiographs (anteroposterior and lateral) revealed a trimalleolar fracture pattern: A lateral malleolar fracture, displaced medial and posterior malleolar fragments, posterior talar subluxation, and expanded syndesmosis (Fig. 1 and 2). Due to the urgency of the open injury, a computed tomography scan was performed. Basic blood work was unremarkable.
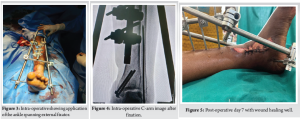
The patient was promptly transported to the surgery room. After extensive irrigation and debridement, the medial malleolus was reduced and internally fixed with two partially threaded 4 mm cancellous screws. The lateral malleolus was fastened with a 2.5 mm K wire. The posterior malleolus was found to be anatomically smaller. The syndesmotic stability was reviewed intraoperatively and determined to be satisfactory. To improve external stability and protect the soft tissues, an ankle-spanning external fixator with Schanz pins in the tibia and calcaneum was used (Fig. 3 and 4).
Following surgery, the patient received IV antibiotics for 5 days and oral antibiotics for 1 week. The wound healed satisfactorily (Fig. 5 and 6). She was kept non-weight bearing for 8 weeks. Serial radiography revealed bony union. The ankle-spanning external fixator with Schanz pins in the tibia and calcaneum and the fibular wire was moved after 2.5 months (Fig. 7). After 3 months, the patient was able to resume everyday activities and walk independently (Fig. 8). Her American Orthopedic Foot and Ankle Society score was 86, indicating a favorable functional result.


Open trimalleolar ankle fractures with syndesmotic rupture and posterior talar displacement are a challenge for orthopedic surgeons. Particularly in high-grade open wounds, these injuries test the orthopedic surgeon not only in terms of exact anatomical reduction but also in terms of safeguarding vulnerable soft tissues and reducing infection risks. Studies have also emphasized the importance of early soft-tissue coverage and stabilization in open ankle fractures to lower infection rates and improve union outcomes [7]. The uniqueness of this constellation of injuries, along with their degree, calls for a customized and quick intervention. In our situation, the internal biomechanical demands as well as the external soft-tissue considerations were addressed using a single-stage hybrid fixation technique. While an ankle-spanning external fixator gave more support without compromising soft-tissue integrity, this approach helped the medial and lateral malleoli and posterior fragment stabilize right away. The synergy of internal and external fixation in a single stage has been validated in polytrauma and open injury scenarios, promoting both mechanical stability and biological recovery [8]. Several treatment strategies for such injuries exist in the literature. With open trimalleolar fractures, Górski et al. showed effectiveness with Ilizarov external fixation alone [4]. Although this gave sufficient fracture alignment and wound treatment, the absence of internal fixation might affect long-term joint mechanics and articular congruency. Further, it has been shown that in high-energy ankle injuries, articular congruity restoration remains a key prognostic factor for post-traumatic arthritis and functional return [9]. Conversely, Kim and Park presented a hybrid method combining internal screws and suture-button constructions [5] for Danis–Weber type C fractures on the other end of the continuum. Although their approach helps to control confined fractures with syndesmotic injuries, it might not be the best in open situations when soft-tissue handling is critical. Xu et al. detailed a “floating ankle,” in which internal fixation comes later following exterior fixation [6]. Although suitable in unstable soft-tissue disorders, this approach can postpone rehabilitation, extend hospital stay, and call for more surgical visits. Biomechanical data directly guided the choice to correct the posterior malleolus. Gardner et al., who underlined the need for posterior stabilization in preserving ankle mortise congruency [1], concluded that fixation of the posterior fragment improves syndesmotic stability more effectively than trans-syndesmotic screws alone [3]. Our experience combines these ideas into one operational solution. We obtained union, conserved alignment, and promoted early rehabilitation without the need for artificial operations by combining internal fixation of all malleolar components – including the posterior fragment, with external fixation to minimize strain on soft tissues. To our knowledge, no published case reports a one-stage hybrid method treating an open trimalleolar fracture with syndesmotic disturbance and posterior talar displacement in the way reported. A recent systematic review by Vopat et al. discussed evolving concepts in syndesmotic injury management and called for more case-based innovations tailored to complex patterns [10]. This case emphasizes the possible advantages of a strong but precisely carried out hybrid approach. When soft-tissue conditions are appropriate, this can help to lower surgical load, improve stability, and produce positive results in even the most complicated fracture situations.
Open trimalleolar ankle fractures with syndesmotic damage and posterior talar subluxation are difficult to treat surgically. Nuance and balance are needed to restore anatomy while maintaining soft tissue. A single-stage hybrid fixation method allowed us to internally restore the bone architecture and externally fix the damaged soft-tissue envelope. The effective union, function restoration, and lack of problems in our patient demonstrate the potential of this comprehensive technique. This method reduces surgical procedures, infection risk, and recovery time. Our experience suggests that properly designed hybrid fixation may be a pragmatic and effective treatment for high-energy open ankle fractures with complicated anatomical abnormalities. Patient selection is still important.
More large case series and extended follow-up are needed to confirm these findings and improve surgical techniques for difficult fracture forms.
In carefully selected cases, a single-stage hybrid fixation approach combining internal fixation and external stabilization can successfully manage complex open trimalleolar ankle fractures with syndesmotic disruption and posterior talar subluxation, ensuring fracture stability, protecting soft tissues, and leading to favorable functional outcomes.
References
- 1. Gardner MJ, Brodsky A, Briggs SM, Nielson JH, Lorich DG. Fixation of posterior malleolar fractures provides greater syndesmotic stability. Clin Orthop Relat Res 2006;447:165-71. [Google Scholar]
- 2. Gawali SR, Kukale SB, Nirvane PV, Toshniwal RO. Management of fracture of posterior malleolus, trimalleolar fracture, fracture dislocations, and syndesmosis injury of ankle joint. J Foot Ankle Surg (Asia-Pacific) 2017;4:90-6. [Google Scholar]
- 3. Smith TO, Davies L, Hing CB. The effect of posterior malleolar fixation on syndesmotic stability: A biomechanical study. Bone Joint J 2013;95-B:1377-83. [Google Scholar]
- 4. Górski R, Wójcik B, Sibiński M. Open trimalleolar fractures treated with Ilizarov external fixator. Ortop Traumatol Rehabil 2019;21:449-56. [Google Scholar]
- 5. Kim GB, Park CH. Hybrid fixation for Danis-Weber type C fractures with syndesmosis injury. Foot Ankle Int 2021;42:137-44. [Google Scholar]
- 6. Xu H, Yang S, Li H. Staged treatment and internal fixation of floating ankle: A case report. Exp Ther Med 2021;22:1129. [Google Scholar]
- 7. Nanchahal J, Nayagam S, Khan U, Moran C, Barrett S, Sanderson F, et al. Standards for the Management of Open Fractures of the Lower Limb. London: British Orthopaedic Association/BAPRAS; 2009. [Google Scholar]
- 8. Henley MB. Initial stabilization of open fractures: The role of external fixation. Instr Course Lect 1997;46:513-22. [Google Scholar]
- 9. Hintermann B, Regazzoni P, Lampert C, Stutz G, Gächter A. Arthroscopic findings in acute fractures of the ankle. J Bone Joint Surg Br 2000;82:345-51. [Google Scholar]
- 10. Vopat BG, Vopat ML, Lubberts B, DiGiovanni CW. Current trends in the diagnosis and management of syndesmotic injury. Curr Rev Musculoskelet Med 2017;10:94-103. [Google Scholar]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2025 Comparative Evaluation of Functional Outcomes Following Surgical and Conservative Management of Distal Tibia Shaft Fractures: A Prospective Observational Study
July 1, 2025 Comparative Evaluation of Functional Outcomes Following Surgical and Conservative Management of Distal Tibia Shaft Fractures: A Prospective Observational Study December 1, 2025 Hook Plate Fixation of an Isolated Pisiform Fracture with a Small Proximal Fragment: A Case Report
December 1, 2025 Hook Plate Fixation of an Isolated Pisiform Fracture with a Small Proximal Fragment: A Case Report November 1, 2025 Atypical Transverse Midshaft Humerus Fracture in an Octogenarian: Surgical Nuances and Functional Outcome Following Locked Intramedullary Nailing
November 1, 2025 Atypical Transverse Midshaft Humerus Fracture in an Octogenarian: Surgical Nuances and Functional Outcome Following Locked Intramedullary Nailing November 1, 2025 Functional Outcome of Distal Third Tibial Fractures Treated by Posterior versus Medial Plating – A Prospective Comparative Study
November 1, 2025 Functional Outcome of Distal Third Tibial Fractures Treated by Posterior versus Medial Plating – A Prospective Comparative Study