
This case highlights that locking mechanism failure, though rare can be a cause of early revision. This case serves as a reminder for surgeons to be meticulous during the final locking of the polyethylene liner to the tibial baseplate. Proper preventive measures, such as thoroughly clearing all soft tissues and ensuring no interference with the locking mechanism, are essential to avoid such complications.
Dr. Chandan Mehta, Department of Orthopaedics, Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India. E-mail: drchandanmehta01@gmail.com
Introduction: Bilateral total knee arthroplasty (TKA) with a cruciate-retaining (CR) design is a widely performed procedure, but complications involving the prosthesis’s locking mechanism are rare. We present a case of locking clip dislodgement in a Zimmer Biomet Vanguard prosthesis, highlighting a rare cause of post-operative swelling and hardware impingement.
Case Report: A patient, 1 year after undergoing bilateral TKA, presented with a four-month history of medially prominent knee swelling. Clinical examination and radiographs revealed impinging hardware and confirmed the failure of the locking mechanism, with the locking clip visible as a dislodged entity. Following a negative work-up for infection, the patient was taken for revision surgery. The locking clip was found in the subcutaneous tissue, having buttonholed through the retinaculum. To facilitate access, the posterior cruciate ligament was released, a quadriceps snip was performed, and the anterior superficial medial collateral ligament was subperiosteally released. The original polyethylene liner was replaced with a new anterior stabilized (AS) polyethylene liner of the same thickness and secured with a new locking clip. Intraoperative cultures were negative. The post-operative course was uneventful, with the patient achieving full range of motion within 1 week.
Conclusion: This case report underscores that locking mechanism failure should be considered in the differential diagnosis of post-TKA knee swelling and pain. The use of an AS polyethylene liner with a new locking clip proved to be a successful revision strategy, leading to a favorable functional outcome.
Keywords: Total knee replacement, Locking mechanism failure, Cruciate retaining, Zimmer Biomet vanguard prosthesis
A successful locking mechanism between the Tibial baseplate and polyethylene liner is essential for favorable outcome of a design of total knee replacement (TKR) prosthesis. An inefficient locking mechanism will result in relative motion between the liner and the tibial baseplate even in the unloaded condition. Increased micro-motion between the polyethylene liner and tibial baseplate will result in backside wear of polyethylene and increased risk of osteolysis. Therefore, it is imperative to have an efficient locking mechanism that will keep this micro-motion to a minimum. The prosthesis used in the case report described below is the Zimmer-Biomet vanguard knee cruciate retaining (CR) design, which employs central dovetail locking mechanism which compresses the polyethylene bearing against the tray by utilizing an oversized titanium locking bar that forces the bearing against a 10° posterior boss [1]. The proposed advantage of this mechanism is that it allows for maintained thickness of the polyethylene insert on the peripheries, as the locking mechanism is kept anteriorly within the intercondylar area [1]. The failure of this locking mechanism has been described in a limited number of case reports, all of them were in the constrained or posterior stabilized designs. This was probably due to the increased forces on the locking mechanism arising from the constraintness of the prosthesis. To the best of our knowledge, previously only one such case has been reported in the CR design [2].
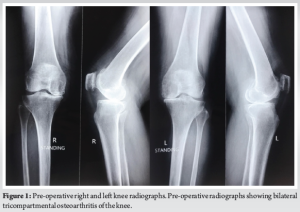
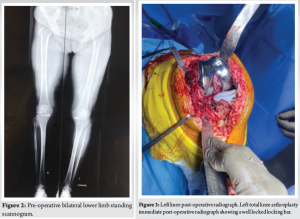
An 80-year-old female presented to our outpatient department with bilaterally painful knees, diagnosed to have bilateral tricompartmental knee osteoarthritis (Fig. 1 and 2) without any comorbidities. The patient was operated for bilateral TKR in staggered manner 2 weeks apart with the left side being operated first. Both the knees were operated with Zimmer-Biomet CR vanguard prosthesis with 10 mm polyethylene insert being used on both the sides (Fig. 3 and 4). The post-operative course was uneventful with patient achieving full range of motion (ROM) 0–120°. The follow-up of the patient at 3 and 6 months was unremarkable as well, with patient being able to carry out her daily activities unassisted.
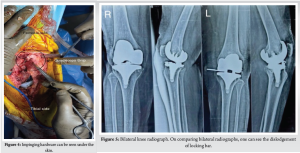
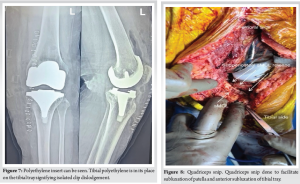
One year postoperatively patient presented with localized painless swelling over medial aspect of knee associated with palpation of hardware, which was first noticed by the patient 4 months back not associated with any trauma and has remained constant since then. On examination, the patient had mild discomfort – with maintained ROM up to 120°. There was a small, localized swelling over medial aspect of knee, which, on superficial palpation, revealed impinging hardware (Fig. 4). Radiographs (Fig. 5) demonstrated the backing out of the locking clip, which is inserted in a medio-lateral manner to keep the polyethylene insert in its place (linear locking mechanism using tongue and groove), with the polyethylene insert being in its place. Immediate post-operative radiographs and radiographs taken at follow-up were examined to confirm the correct initial position of the locking clip.
Laboratory investigations were done to rule out any possibility of infection. The laboratory parameters were within normal limits as follows:
1. Hemoglobin/total leukocyte count – 11.2/9600
2. Erythrocyte sedimentation rate – 20 mm/h
3. C-reactive protein – 8 mg/L.
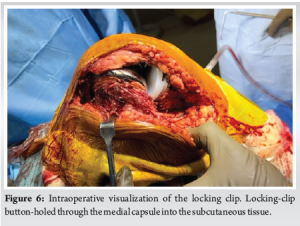
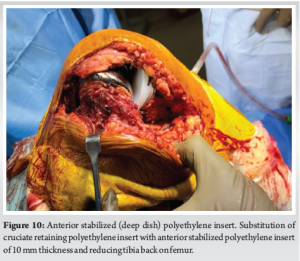
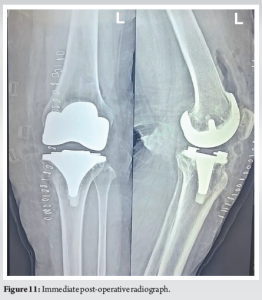
The patient was undertaken for surgery at the earliest possible time, so as to prevent complete perforation of skin and soft-tissue compromise. Medial para-patellar approach through the previous incision was undertaken. Intraoperatively, the locking clip was found to buttonhole through the medial capsule into the subcutaneous tissue (Fig. 6). The polyethylene insert was in its place (Fig. 7) on the tibial baseplate without any evidence of subluxation. The flexion and extension gaps were assessed and were found to be well balanced. The polyethylene insert was removed after subluxating Tibia and no significant wear was seen on either surface. Subluxation of tibia was facilitated by removing the posterior cruciate ligament, performing a quadriceps snip (Fig. 8) and subperiosteal release of anterior portion of superficial medial collateral ligament (Fig. 9) [3]. The CR polyethylene insert was removed and replaced with an anterior stabilizing or deep dish polyethylene insert of 10 mm (Fig. 9-11). Standard post-operative closure was performed. The post-operative course was uneventful with patient achieving full ROM at 1 week without any extension lag. Intraoperatively, samples were collected and sent for culture sensitivity which tested negative.

There are two types of locking mechanisms of polyethylene onto the tibial baseplate, peripheral and central, using a tongue-in-groove or Dovetail mechanism [4,5]. The Zimmer Biomet Vanguard knee involves central dovetail locking mechanism which compresses the polyethylene bearing against the tray by utilizing an oversized titanium locking bar that forces the bearing against a 10° posterior boss [1]. The proposed advantage of this mechanism is that it allows for maintained thickness of the polyethylene insert on the peripheries, as the locking mechanism is kept anteriorly within the intercondylar area [1]. To the best of our knowledge, only one such case has been reported of the failure of locking bar mechanism in a case of CR design of TKR prosthesis [2]. All other case reports of failure of locking mechanism have been reported in constrained knees or posterior stabilized knees [6-10]. This is considered because increase in constraintness of a prosthesis has been linked to an increase in micro-motion between the tibial baseplate and polyethylene insert leading to greater, thereby greater the chances of failure of locking mechanism. Locking mechanism failure can lead to subluxation or dissociation of the polyethylene. Two mechanisms are described: Anterior lift-off of the bearing in flexion, resulting in an anterior displacement and posterior lift-off in extension, with a posterior dislocation of the polyethylene [5,10]. Risk factors are malpositioning of the tibial component with anterior slope or varus, flexion–extension mismatch, deficiency of the extensor mechanism, or extensive posterolateral release [7]. These conditions are more often observed in revision knee arthroplasty than in primary total knee arthroplasty [7], hence the higher rates failure of locking mechanism. In our case, there is no evidence to suggest that there was any surgical error in locking of the components, because this failure occurred late in the post-operative period. Evidence from biomechanical models suggests that, if this were the reason, the loose locking bar would have backed out much sooner, as the patient was bearing weight normally in the post-operative period. Furthermore, none of the proposed risk factors were found to be present. The rarity of such an event, especially in the CR designs further makes it difficult to point toward any cause with utmost certainty. The limitation of this report is that the facilities were not available for the analysis of the retrieved polyethylene liner and the lockin bar, so as to rule out any manufacturing defect. The surgeon was an experienced in using vanguard CR prosthesis, thereby eliminating the possibility of any surgical error.
Introduction of modularity in TKR prosthesis is associated with its own disadvantages. Locking mechanism, though helps in reducing the backside wear, its failure even though rare can be a cause of early revision. Special attention should be paid while locking polyethylene liner onto the tibial baseplate so as to remove any error on the surgeon’s counterpart. As preventive measures, the surgeons are advised to clear all soft tissues before positioning the bearing and to make sure nothing interferes with the locking pin or the bearing.
The surgeons are advised to clear all soft tissues before positioning the bearing and to make sure nothing interferes with the locking pin or the bearing.
References
- 1. Available from: https://www.zimmerbiomet.com/content/dam/zimmer-biomet/medical-professionals/knee/vanguard-knee-system/vanguard-design-rationale-2537.1-US-en.pdf [Google Scholar] [PubMed]
- 2. Sharma A, Killampalli V, Patel A. Locking mechanism failure between tibial baseplate and polyethylene insert in cruciate retaining total knee arthroplasty. J Clin Orthop Trauma 2022;34:102013. [Google Scholar] [PubMed]
- 3. Łapaj Ł, Mroz A, Kokoszka P, Markuszewski J, Wendland J, Helak-Lapaj C, et al. Peripheral snap-fit locking mechanisms and smooth surface finish of tibial trays reduce backside wear in fixed-bearing total knee arthroplasty. Acta Orthop 2017;88:62-9. [Google Scholar] [PubMed]
- 4. Bhimji S, Wang A, Schmalzried T. Tibial insert micromotion of various total knee arthroplasty devices. J Knee Surg 2010;23:153-62. [Google Scholar] [PubMed]
- 5. Chaiyakit P, Petcharat B, Hongku N, Iawsuwan A. Complete release of the superficial medial collateral ligament in total knee arthroplasty. Arthroplast Today 2024;25:101301. [Google Scholar] [PubMed]
- 6. Thienpont E. Failure of tibial polyethylene insert locking mechanism in posterior stabilized arthroplasty. Knee Surg Sports Traumatol Arthrosc 2013;21:2685-8. [Google Scholar] [PubMed]
- 7. Chen CE, Juhn RJ, Ko JY. Dissociation of polyethylene insert from the tibial baseplate following revision total knee arthroplasty. J Arthroplasty 2011;26:339-e11-3. [Google Scholar] [PubMed]
- 8. Rapuri VR, Clarke HD, Spangehl MJ, Beauchamp CP. Five cases of failure of the tibial polyethylene insert locking mechanism in one design of constrained knee arthroplasty. J Arthroplasty 2011;26:976.e21-4. [Google Scholar] [PubMed]
- 9. Voskuijl T, van Riet P, Cals-Stegeman F, van der Heide A, Verdonschot N, van der Ven R. Insert dissociation after fixed bearing PS constrained Genesis II total knee arthroplasty. A case series of nine patients. Acta Orthop Belg 2016;82:331-7. [Google Scholar] [PubMed]
- 10. Soni M, Dhiman D. Disengagement of tibial insert locking pin in total knee arthroplasty – A rare failure case report. J Clin Orthop Trauma 2022;30:101918. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 Randomized Control Trial Comparing Effects of Tourniquets on Neurology and Functional Outcomes after Total Knee Arthoplasty
August 1, 2025 Randomized Control Trial Comparing Effects of Tourniquets on Neurology and Functional Outcomes after Total Knee Arthoplasty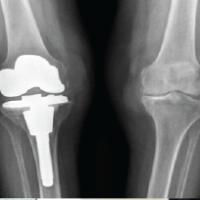 March 1, 2025 Total Knee Replacement Versus Osteosynthesis as Primary Treatment in Older Patients with Tibial Plateau Fracture
March 1, 2025 Total Knee Replacement Versus Osteosynthesis as Primary Treatment in Older Patients with Tibial Plateau Fracture October 1, 2024 Vascular Injury during Total Knee Replacement and Check List to Follow in its Management: Case Report
October 1, 2024 Vascular Injury during Total Knee Replacement and Check List to Follow in its Management: Case Report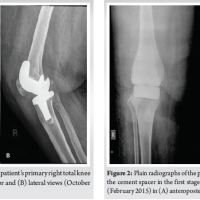 April 10, 2024 Concomitant Cement Spacer and Peri-spacer Fractures Seven Years After First-stage Revision Knee Arthroplasty: A Case Report
April 10, 2024 Concomitant Cement Spacer and Peri-spacer Fractures Seven Years After First-stage Revision Knee Arthroplasty: A Case Report