
The learning point from this article is that principles of early appropriate care should be followed in managing polytrauma patients with multiple fractures to guide the timing of definitive fracture fixation.
Dr. Bhashker Rai, Department of Orthopaedics, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India. E-mail: direct2bhaskar@gmail.com
Introduction: Polytrauma is defined as multiple severe injuries with an abbreviated injury scale ≥3 in two or more body regions, often resulting from high-energy trauma. Managing such cases, especially in adolescents with complex fractures, requires a well-coordinated, physiologically guided approach. This case report discusses the management of an 18-year-old female with multiple fractures, including the lower limb, upper limb, and pelvis, following a high-energy fall. Early appropriate care (EAC) was essential in guiding treatment decisions.
Case Report: An 18-year-old female fell from a height of 20 feet on June 19, 2022, and presented with pain and swelling over both arms, left hip, and thigh, along with an inability to bear weight. Clinical examination revealed a right humerus fracture, complex elbow dislocation (left side), a T-type acetabulum fracture, and a left femur shaft fracture. Initial resuscitation followed advanced trauma life support guidelines. On June 25, 2022, wound debridement and fracture stabilization of the right humerus were performed using an external fixator, and the left elbow dislocation was treated with closed reduction and K-wire fixation. The left humerus fracture was treated with open reduction and internal fixation, and retrograde femoral nailing was done for the left femur. On June 29, acetabular and pubic rami fractures were addressed using the modified stoppa approach. Post-operative rehabilitation focused on non-weight-bearing for 6 weeks and gradual strengthening exercises. After 2 years, the patient had regained full functional ability with a Harris Hip Score of 97 and satisfactory radiological results.
Conclusion: This case highlights the importance of EAC in polytrauma management. Timely interventions, appropriate fracture fixation, and structured rehabilitation led to excellent functional and radiological outcomes. A multidisciplinary approach is crucial in managing such complex trauma cases to optimize recovery.
Keywords: Polytrauma, early appropriate care, stoppa approach.
Polytrauma is defined as cases with an abbreviated injury scale ≥3 for two or more different body regions and one or more additional variables from five physiologic parameters (hypotension [systolic blood pressure ≤90 mmHg], unconsciousness [Glasgow coma scale score ≤8], acidosis [base excess ≤−6.0], coagulopathy [partial thromboplastin time ≥40 s or international normalized ratio ≥1.4], and age [≥70 years]) [1]. Due to the complexity of injuries, managing polytrauma in adolescents with multiple fractures, especially after high-energy falls, requires a well-coordinated approach. As per the principles of early appropriate care (EAC) in a polytrauma patient, treatment is based on physiologic and laboratory assessment, and the adequacy of resuscitation guides the timing of definitive fracture fixation [2]. This case report details the management of an 18-year-old female with a complex fracture of the lower limb, upper limb, as well as pelvi-acetabulum. In these kinds of patients with multiple fractures, prioritizing the order of definitive fixation is quite challenging for the treating surgeon [3]. It is very difficult to decide how many fractures to fix at 1 time as it depends on the patient’s overall condition, the complexity of fractures, and the available resources. The risk of prolonged surgery or anesthesia should always be considered against the potential benefits of early fixation while managing such cases. After an extensive literature review, we could not find any case report with such complex injuries in a patient after high-energy trauma.
An 18-year-old female fell from a height of 20 feet on June 19th, 2022 and presented with complaints of pain and swelling over the bilateral distal arm and elbow, pain over the left hip and thigh, and inability to bear weight. Clinical examination showed a 2 × 2 cm open wound over the right distal arm and tenderness over the bilateral distal arm and left mid-thigh and hip. Three-point relationship over the left elbow was distorted and the pelvic compression test was positive. Initial resuscitation was done as per the advanced trauma life support Protocol. Based on clinical and radiological evaluation patient was found to have multiple upper and lower limb fractures, which are:
- Open shaft of humerus fracture right side (AO12B2) (Fig. 1a)
- Complex elbow fracture-dislocation (terrible triad) with shaft humerus fracture (AO12A2) left side (Fig. 1b)
- T-type Acetabulum fracture on the left side with bilateral superior and inferior pubic rami fracture (Fig. 1c)
- Shaft of femur fracture left side (AO32A2) (Fig. 1d)
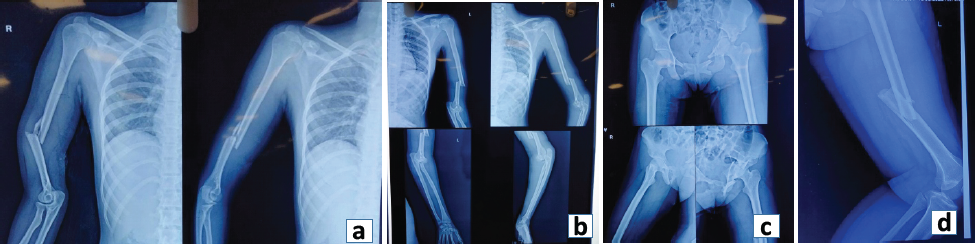
Figure 1: (a) Pre-operative X-ray showing the shaft of the humerus fracture right side (AO12B2), (b) Pre Op X-ray showing complex elbow fracture-dislocation (terrible triad) with shaft humerus fracture (AO12A2) left side, (c) T-type Acetabulum fracture left side with bilateral superior and inferior pubic rami fracture, (d) Shaft of femur fracture left side (AO32A2).
Management was planned as per the principles of EAC. On June 25th, 2022, the following fractures were managed under general anesthesia in the same sitting:
- Wound debridement and fracture stabilization of the right arm were done with an external fixator (Fig. 2a)
- For elbow dislocation, closed reduction and trans-olecranon fixation with two K-wires was done (Fig. 2b)
- Open reduction and internal fixation (ORIF) of the left humerus fracture was done with a limited-contact dynamic compression plate (LCDCP) through posterior approach (Fig. 2b)
- As the left acetabulum was also fractured along with the shaft of the femur, retrograde femur nailing was done.

Figure 2: (a): Post-operative X-ray showing stabilization of right humerus with an external fixator, (b) Post-operative X-ray showing trans-olecranon fixation of the left elbow and internal fixation of left humerus fracture with limited-contact dynamic compression plate. (c) Intra Op image showing acetabulum fracture fixation through Modified Stoppa Approach.
In the second sitting on June 29th, open reduction and pubic symphysis plating was done along with anterior column buttress plating through a modified Stoppa approach to address both the acetabulum and rami fracture simultaneously (Fig. 2c). On July 15th, 2022 the external fixator was removed from the right upper limb; pin sites were healthy. ORIF of humerus fractures were done with 4.5 mm LCDCP through a posterior approach. From the left elbow, K-wires were also removed, and above-elbow support was given for the next 6 weeks. The patient was advised to perform passive and active range of motion exercises in the right elbow and shoulder, and left hip and knee from the 1st post-operative day. The patient was advised to complete non-weight-bearing on the left lower limb for 6 weeks. After 6 weeks, partial weight-bearing was advised with walker support, the slab was removed and left elbow and shoulder range of motion exercises were started. After 3 months, complete weight-bearing was allowed. Active quadriceps, hamstrings, and hip abductors strengthening exercises were also advised. The patient was followed up at regular intervals for a period of 2 years to assess functional and radiological outcomes. After 6 months, the patient was able to do all her daily routine activities. The patient regained her pre-trauma level of activities by the end of 1 year. On the past visit at 2 years, the patient had satisfactory radiological (Fig. 3a and b) and functional outcomes (Fig. 4). Her Harris hip score was 97. The bilateral elbow range of motion was adequate without any instability.
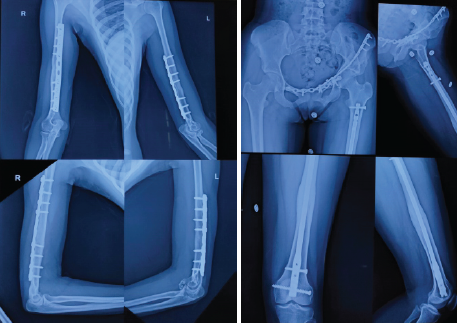
Figure 3: (a) Follow-up X-ray showing bilateral upper arm at 2 years. (b) Follow-up X-ray showing left-sided acetabulum and femur at 2 years.

Figure 4: Functional assessment at 2 years.
Written informed consent for publication of the research details and clinical images was obtained from the patient.
Managing polytrauma patients is challenging due to the lack of a clear consensus on the preferred approach [4]. This case report highlights the critical importance of EAC in managing such patients. Poly-trauma, by definition, involves multiple severe injuries to different body systems, often presenting in a critically unstable state. The patient’s survival in this case underscores how early, coordinated, and systematic interventions can drastically impact survival rates. In EAC, the timing of definitive fracture fixation is decided by the patient’s physiologic parameters [5]. In the management of poly-trauma, damage control orthopedics (DCO) also plays a pivotal role, especially in patients who present in a critically unstable state. The primary goal of DCO is to stabilize the patient physiologically before embarking on definitive surgical interventions [6]. The management of poly-trauma requires a multidisciplinary team approach. The integration of orthopedic surgeons, trauma surgeons, radiologists, anaesthetists, intensivists, and nurses, working together as a cohesive unit, is essential for optimizing patient care [7].
We anticipated the following challenges in this case:
- Optimization of the Patient’s physiologic state
- Management of complex elbow fracture-dislocation (terrible triad)
- Addressing acetabular and rami fractures simultaneously through the same approach
- Acetabulum Fracture with the shaft of the femur fracture on the same side
- Open humerus fracture on the right side.
Principles of EAC were followed to optimize patients’ physiologic state. Reduction and stabilization of the Elbow fracture-dislocation were done to allow soft tissues to heal properly. The modified stoppa approach can be used to address both acetabulum and rami fractures simultaneously when supplemented with a lateral window [8]. Studies have shown satisfactory outcomes in acetabulum fractures fixed using the modified stoppa approach [9]. We preferred the distal femoral nail for the shaft femur as the patient had ipsilateral acetabular and rami fractures. Few studies have reported that retrograde femoral nails can also be an effective alternative to external fixators as damage control devices [10]. More such cases should be reported for comparison of outcomes.
This case demonstrates the importance of EAC in managing polytrauma with multiple fractures. Timely and coordinated interventions lead to successful recovery, with the patient regaining pre-trauma function. This case report also highlights the need for effective, multidisciplinary care in complex trauma cases. In managing these types of cases, proper pre-operative evaluation and planning result in better outcomes. Post-operative rehabilitation plays a significant role in improving functional outcomes.
Early appropriate care is the cornerstone for managing polytrauma with multiple fractures, ensuring timely stabilization and recovery. A well-coordinated, multidisciplinary approach is a key to achieving optimal functional outcomes.
References
- 1. Rau CS, Wu SC, Kuo PJ, Chen YC, Chien PC, Hsieh HY, et al. Polytrauma defined by the New Berlin definition: A validation test based on propensity-score matching approach. Int J Environ Res Public Health 2017;14:1045. [Google Scholar] [PubMed]
- 2. Gupta B, Farooque K. Early total care to early appropriate care – what every anesthesiologist must know! J Anaesthesiol Clin Pharmacol 2023;39:3-10. [Google Scholar] [PubMed]
- 3. Devendra A, Nishith PG, Dilip Chand Raja S, Dheenadhayalan J, Rajasekaran S. Current updates in management of extremity injuries in polytrauma. J Clin Orthop Trauma 2021;12:113-22. [Google Scholar] [PubMed]
- 4. Massaga F, Washington LA, Ngayomela IH, Mwami AS, Shabhay A. Management of a road traffic accident poly-trauma patient in a limited regional resource hospital setting in Tanzania: Review of literature and case report. Int J Surg Case Rep 2023;110:108764. [Google Scholar] [PubMed]
- 5. Vallier HA, Wang X, Moore TA, Wilber JH, Como JJ. Timing of orthopaedic surgery in multiple trauma patients: Development of a protocol for early appropriate care. J Orthop Trauma 2013;27:543-51. [Google Scholar] [PubMed]
- 6. Volpin G, Pfeifer R, Saveski J, Hasani I, Cohen M, Pape HC. Damage control orthopaedics in polytraumatized patients- current concepts. J Clin Orthop Trauma 2021;12:72-82. [Google Scholar] [PubMed]
- 7. Jeong TS. A multidisciplinary approach to polytrauma management. Korean J Neurotrauma 2024;20:1-2. [Google Scholar] [PubMed]
- 8. Liu Y, Yang H, Li X, Yang SH, Lin JH. Newly modified stoppa approach for acetabular fractures. Int Orthop 2013;37:1347-53. [Google Scholar] [PubMed]
- 9. Kilinc CY, Acan AE, Gultac E, Kilinc RM, Hapa O, Aydogan NH. Treatment results for acetabulum fractures using the modified stoppa approach. Acta Orthop Traumatol Turc 2019;53:6-14. [Google Scholar] [PubMed]
- 10. Al Maskari S, Muzaffar R, Yaseen A. Retrograde femoral nails for emergency stabilization in multiply injured patients with haemodynamic instability. Trauma Case Rep 2020;29:100350. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 In Trauma Expect the Unexpected – A Case Report on Post-Traumatic Pancreatitis associated with Superior Mesenteric Artery Pseudoaneurysm in Spinopelvic fracture
November 1, 2025 In Trauma Expect the Unexpected – A Case Report on Post-Traumatic Pancreatitis associated with Superior Mesenteric Artery Pseudoaneurysm in Spinopelvic fracture October 1, 2025 A Unique Case of Bilateral Elbow Terrible Triad in a Polytrauma Patient: Associated Challenges in Management
October 1, 2025 A Unique Case of Bilateral Elbow Terrible Triad in a Polytrauma Patient: Associated Challenges in Management September 1, 2025 Neglected Isolated Lunate Dislocation in a Polytrauma Patient Presenting as Acute Carpal Tunnel Syndrome – A Case Report with Review of Literature
September 1, 2025 Neglected Isolated Lunate Dislocation in a Polytrauma Patient Presenting as Acute Carpal Tunnel Syndrome – A Case Report with Review of Literature May 1, 2025 Brachial Plexus Neuropraxia Post Open Reduction and Internal Fixation of Left Acetabulum Fracture
May 1, 2025 Brachial Plexus Neuropraxia Post Open Reduction and Internal Fixation of Left Acetabulum Fracture