
Non-union of talus fractures is uncommon but can occur with inadequate initial treatment, especially in displaced injuries. Early surgical intervention with anatomical reduction and stable fixation is crucial to ensure healing and restore function. ORIF with cannulated cancellous screws is an effective technique for achieving union in delayed cases.
Dr. Yogeshwar Agharkar, Department of Orthopaedics, Sree Balaji Medical College and Hospital, Chennai, Tamil Nadu, India. E-mail: yogeshwaragharkar1998@gmail.com
Introduction: Talus fractures are uncommon, accounting for <1% of all fractures, but they are clinically significant due to their high propensity for complications, such as avascular necrosis, post-traumatic arthritis, and non-union. The talus has a complex anatomy and a tenuous blood supply, making it particularly vulnerable to healing complications when not managed appropriately. Non-union of talus fractures is rare and often results from inadequate initial treatment, especially in displaced fractures that are managed conservatively.
Case Report: We report the case of a 34-year-old male who sustained a talar body fracture following a high-velocity road traffic accident. The patient was initially managed conservatively with immobilization but presented 6 months later with persistent pain, swelling, and difficulty in weight-bearing. Clinical examination and imaging, including computed tomography scan, revealed a non-union of the talar body fracture with sclerotic margins. Considering the chronicity and symptoms, surgical management was planned. The patient underwent open reduction and internal fixation (ORIF) through an anteromedial approach using two 4.0 mm cannulated cancellous screws. The fracture site was debrided, reduced anatomically, and fixed in a stable construct. Post-operatively, the patient was immobilized and kept non-weight-bearing, followed by a structured rehabilitation protocol.
Conclusion: At follow-up, the patient showed significant clinical improvement, with radiological union observed by 3 months and full return to daily activities by 6 months. This case underscores the importance of accurate diagnosis, appropriate treatment planning, and timely surgical intervention in managing talus fractures to avoid complications, such as non-union. ORIF using cannulated cancellous screws proved to be a safe and effective treatment modality, even in delayed presentations.
Keywords: Talus non-union, cannulated screw fixation, open reduction and internal fixation.
The talus is a key bone in the ankle joint involved in weight transmission from the leg to the foot. Fractures of the talus account for <1% of all fractures and are often associated with high-energy trauma, such as road traffic accidents (RTAs) [1]. The talus has a unique and precarious blood supply, primarily derived from branches of the posterior tibial, dorsalis pedis, and perforating peroneal arteries [2]. This limited vascularity, combined with the absence of muscular attachments, makes the talus particularly susceptible to complications, such as avascular necrosis (AVN), non-union, and post-traumatic arthritis [2,3]. Non-union of talus fractures is rare but clinically significant due to the risk of long-term pain, instability, and degenerative changes [4]. Timely diagnosis and appropriate surgical intervention are crucial for optimal outcomes [5].
A 34-year-old male presented to our outpatient department with complaints of chronic right ankle pain and difficulty bearing weight for the past several months. He gave a history of a high-velocity RTA 6 months ago, following which he was diagnosed with a talus fracture and managed conservatively with immobilization and non-weight-bearing protocol at another center. The patient resumed weight-bearing pre-maturely due to socioeconomic constraints. Clinical examination revealed mild swelling, tenderness over the anterolateral aspect of the ankle, and restricted range of motion. There was no evidence of neurovascular compromise. Plain radiographs of the ankle showed persistent fracture lines in the talar body region (Fig. 1).

Figure 1: Pre-operative X-ray of talus.
A computed tomography scan confirmed a non-union of the talar body fracture with sclerosed fracture margins and minimal displacement. Features of non-union of talus fracture with secondary degenerative changes with Secondary arthritis changes involving the talocalcaneal joint (Fig. 2).
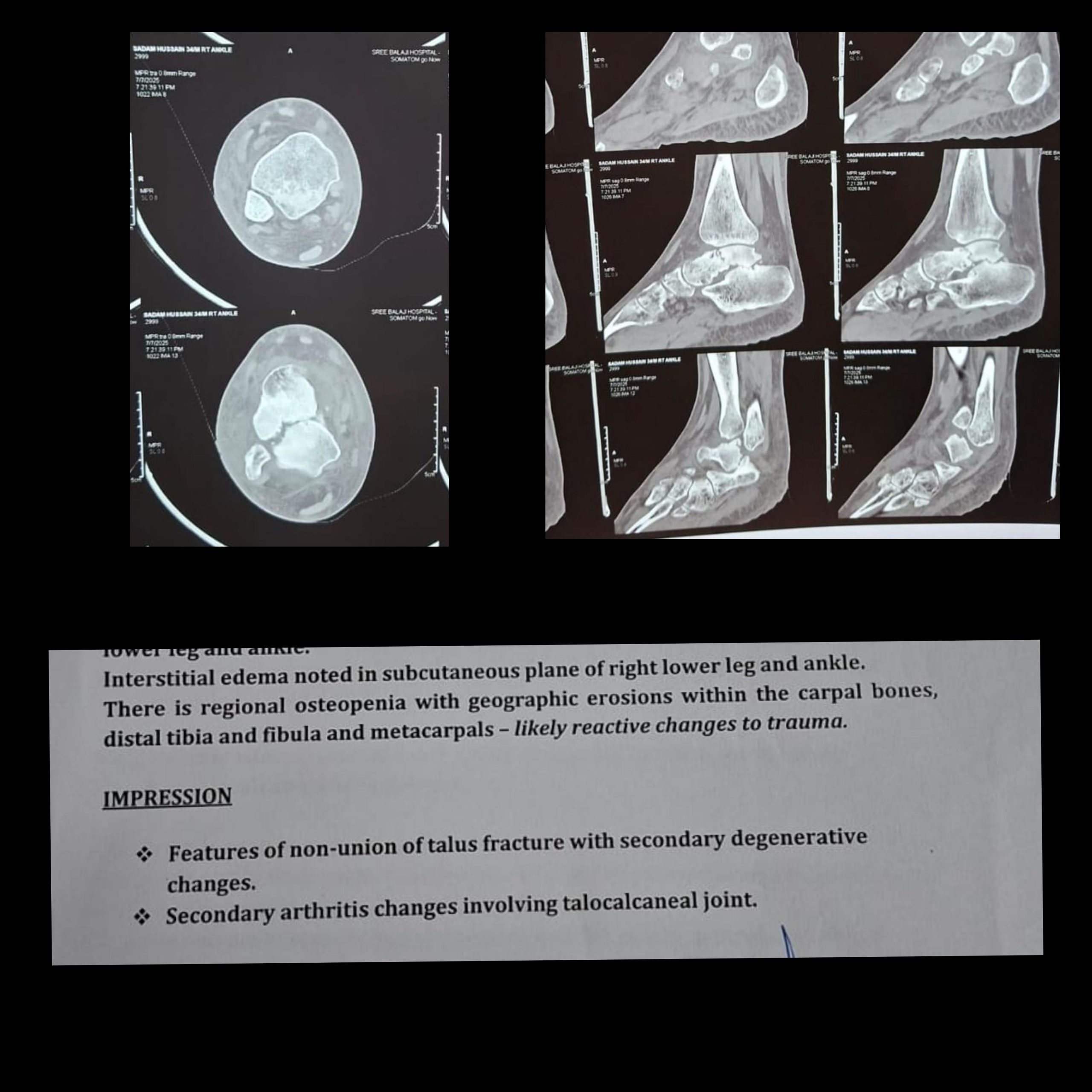
Figure 2: Pre-operative computed tomography scan.
Magnetic resonance imaging was suggestive of features of non-union of talus fracture with secondary degenerative changes. Secondary arthritis changes involving the talocalcaneal joint, with associated synovial inflammation. Injury to the deltoid ligament with high-grade strain with partial thickness tear in the anterior and posterior talofibular ligaments and calcaneofibular ligaments (Fig. 3).
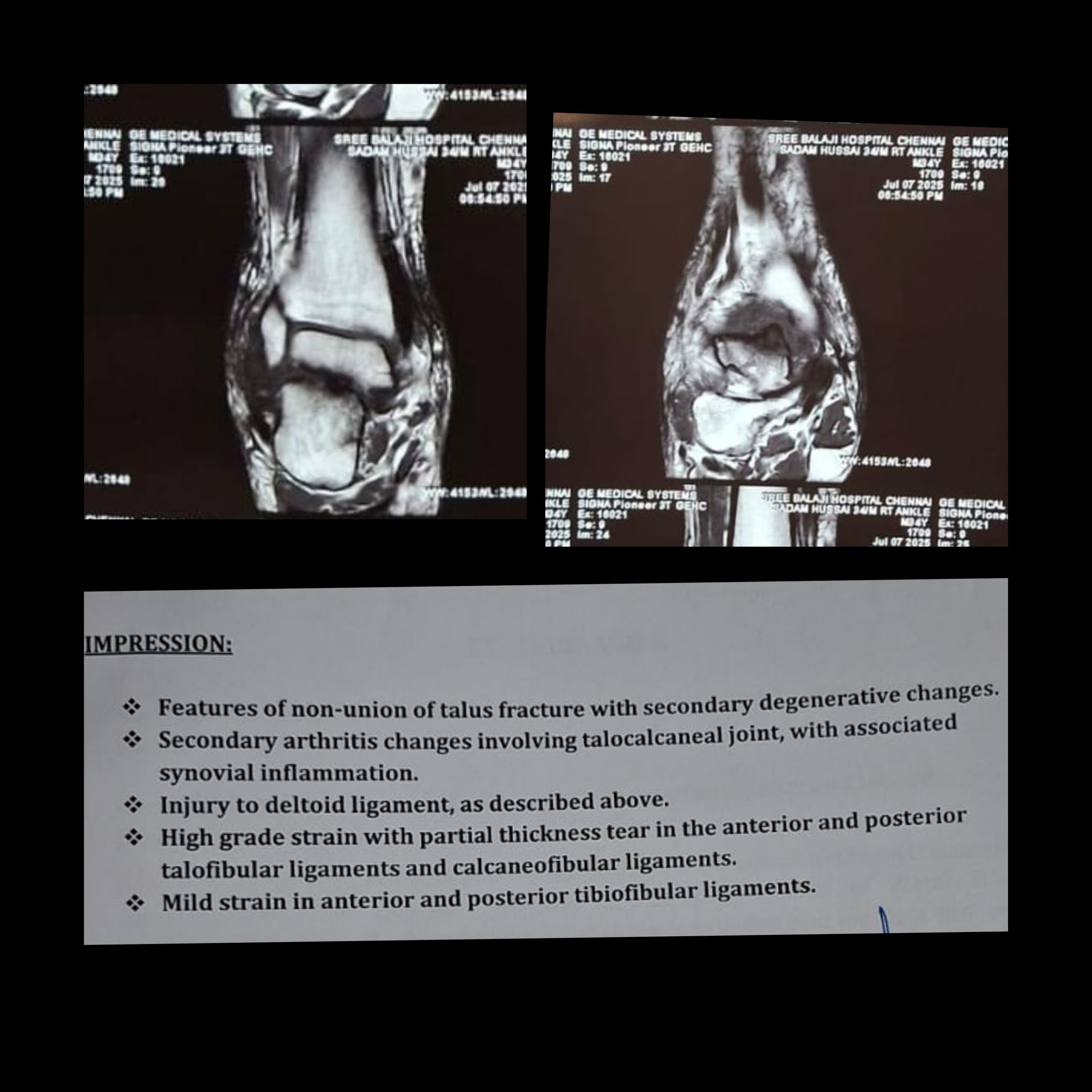
Figure 3: Pre-operative magnetic resonance imaging.
After detailed counseling, the patient was taken up for open reduction and internal fixation (ORIF) under spinal anesthesia. A standard anteromedial approach and anterolateral approach were used (Fig. 4).

Figure 4: Pre-operative clinical picture.
Fibrous tissue and sclerotic bone at the fracture site were debrided to healthy bleeding bone ends. Anatomical reduction was achieved, and fixation was done using two 4.0 mm cannulated cancellous screws inserted in a lag fashion under fluoroscopic guidance [6] (Fig. 5).

Figure 5: Intraoperative C-arm images.
Bone grafting was not required as adequate apposition and stability were achieved. The ankle was immobilized in a below-knee slab for 6 weeks with strict non-weight bearing. Gradual weight-bearing was initiated after radiological evidence of callus formation at 8 weeks. Range of motion exercises were started at 6 weeks post-operatively. At the 3-month follow-up, the patient reported significant pain relief and improved ankle mobility. Radiographs showed signs of union (Fig. 6).

Figure 6: Post-operative X-ray.
At 6 months, the patient was pain-free, fully weight-bearing, and had resumed daily activities.
Non-union of the talus is a rare but debilitating complication, often attributed to the bone’s poor vascularity and improper initial management [2,7]. The talus receives its blood supply from a network of arteries: The artery of the tarsal canal (branch of the posterior tibial artery), the artery of the sinus tarsi (branch of the dorsalis pedis or perforating peroneal artery), and the deltoid branch of the posterior tibial artery [2,8]. Displaced fractures can disrupt this delicate vascular network, significantly increasing the risk of AVN and non-union, particularly in the talar body and neck [3,9]. Conservative management in displaced fractures is generally not advised due to these risks [3]. Early surgical intervention with stable internal fixation helps restore the anatomy and preserves what remains of the blood supply [4]. ORIF with screw fixation remains the gold standard for treating non-union of talus fractures, allowing for restoration of anatomical alignment and mechanical stability [6,9]. In this case, debridement of the fibrous non-union and stable fixation with cannulated screws led to satisfactory union and functional recovery, with no clinical signs of AVN at follow-up.
This case highlights the importance of early recognition and appropriate surgical management of talar fractures. Conservative treatment in displaced fractures may lead to non-union. ORIF using cannulated cancellous screws is effective in achieving union and restoring function in delayed talus fracture cases.
Non-union of talus fractures is an uncommon but challenging complication often resulting from inadequate initial management. Open reduction and internal fixation with cannulated cancellous screws provides reliable union and good functional recovery, even in delayed cases.
References
- 1. Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-24. [Google Scholar] [PubMed]
- 2. Fortin PT, Balazsy JE. Talus fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:114-27. [Google Scholar] [PubMed]
- 3. Canale ST, Kelly FB Jr. Fractures of the neck of the talus. Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 2000;82:219-31. [Google Scholar] [PubMed]
- 4. Halvorson JJ, Winter SB, Teasdall RD, Scott AT. Talar neck fractures: A systematic review of the literature. J Foot Ankle Surg 2013;52:56-61. [Google Scholar] [PubMed]
- 5. Sanders DW, Busam M, Hattwick E, Edwards JR, Johnson KD. Functional outcomes following displaced talar neck fractures. J Orthop Trauma 2004;18:265-70. [Google Scholar] [PubMed]
- 6. Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J. Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-9. [Google Scholar] [PubMed]
- 7. Fitzpatrick DC, Doan JD, Wijdicks CA, et al. High energy injuries of the talus: Evaluation and surgical management. Foot Ankle Clin 2011;16:135-48. [Google Scholar] [PubMed]
- 8. Tornetta P, Creevy WR. Lag screw fixation of displaced talar neck fractures. Foot Ankle Int 2003;24:503-8. [Google Scholar] [PubMed]
- 9. Vallier HA. Fractures of the talus: State of the art. J Orthop Trauma 2015;29:385-92. [Google Scholar] [PubMed]
- 10. Karachalios T, Michail A. Surgical treatment of talar fractures: Current concepts. Injury 2004;35:142-52. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes
December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes October 1, 2025 Comparative Study of Minimally Invasive Plate Osteosynthesis Versus Open Reduction and Internal Fixation in the Treatment of Distal Fibular Fractures
October 1, 2025 Comparative Study of Minimally Invasive Plate Osteosynthesis Versus Open Reduction and Internal Fixation in the Treatment of Distal Fibular Fractures September 1, 2025 Anteromedial Tibia Plateau Fracture without Significant Ligamentous Injury Treated Successfully with Open Reduction and Internal Fixation: A Case Report
September 1, 2025 Anteromedial Tibia Plateau Fracture without Significant Ligamentous Injury Treated Successfully with Open Reduction and Internal Fixation: A Case Report July 1, 2025 Missed Volar Intercalated Segment Instability with Distal Radius Fracture: Challenges in Diagnosis, Surgical Management, and Clinical Outcome – Case Report
July 1, 2025 Missed Volar Intercalated Segment Instability with Distal Radius Fracture: Challenges in Diagnosis, Surgical Management, and Clinical Outcome – Case Report