
One-stage ACL reconstruction combined with medial opening wedge high tibial osteotomy addresses both instability and varus malalignment in a single procedure. Key technical pearls include creating the femoral and tibial tunnels before the osteotomy, positioning the plate posteromedially, and sequencing fixation steps to avoid tunnel–screw conflict, ensuring both graft integrity and osteotomy stability.
Dr. Dhruv A Shah, Department of Orthopaedic Surgeon, Namaha Hospital, Mumbai, Maharashtra, India. E-mail: dr.dhruvshah96@gmail.com
Introduction: Anterior cruciate ligament (ACL) deficiency in the presence of varus malalignment predisposes patients to accelerated medial compartment osteoarthritis (OA) and graft failure after isolated reconstruction. High tibial osteotomy (HTO) is an established method to realign the mechanical axis and offload the medial compartment. Performing ACL reconstruction (ACLR) and HTO in a single stage addresses both instability and malalignment simultaneously, minimizing the need for staged procedures and rehabilitation.
Technique: The procedure begins with diagnostic arthroscopy and femoral as well as tibial tunnel preparation before osteotomy, ensuring adequate knee hyperflexion. A hamstring graft is harvested and prepared, followed by a medial opening wedge HTO using a posteromedially placed osteotomy plate. Posterior screws are inserted first, leaving the anterior holes vacant until tibial tunnel identification. A metal dilator protects the tibial tunnel during anterior screw placement. The prepared graft is then passed, fixed with femoral and tibial cortical fixation or interference screws, and cancellous bone is packed into the tunnel to promote healing.
Conclusion: Single-stage ACLR with medial opening wedge HTO provides simultaneous correction of instability and malalignment in ACL-deficient varus knees. With careful surgical sequencing and technical modifications – especially early tunnel drilling and posteromedial plate placement – the procedure is safe, reproducible, and offers a practical solution for delaying OA progression while restoring knee stability.
Keywords: Joint preservation, knee, anterior cruciate ligament, high tibial osteotomy, osteotomy.
Anterior cruciate ligament (ACL) rupture is one of the most frequently encountered ligamentous injuries in orthopedic practice, especially in young, active individuals. Chronic ACL deficiency is often associated with varus alignment and progressive medial compartment degeneration, leading to increased joint instability and functional impairment. When such mechanical and structural abnormalities coexist, a combination of surgical procedures may be required to restore both joint stability and biomechanical alignment.
In the early 1990s, Neuschwander et al. and Noyes and Barber-Westin were among the first to propose simultaneous high tibial osteotomy (HTO) and ACL reconstruction (ACLR) as a viable single-stage solution for combined varus malalignment and ACL insufficiency. Their work laid the foundation for addressing alignment and instability concurrently, with promising early outcomes in terms of functional restoration and patient satisfaction [1,2].
In 1994, Dejour et al. expanded on this by emphasizing valgus-producing HTO to offload the medial compartment while addressing ligament deficiency, particularly in younger patients. Similarly, Lattermann and Jakob advocated the combined approach in selected individuals, particularly when instability was the primary complaint alongside degenerative changes [3,4].
Agneskirchner and Imhoff detailed the technical aspects of simultaneous ACLR and open-wedge HTO in a larger cohort, further validating this surgical approach. They emphasized the importance of careful pre-operative planning and intraoperative sequencing to avoid complications such as tunnel-plate interference or altered posterior tibial slope [5].
Despite these advancements, simultaneous ACLR-HTO remains technically demanding. A common concern is the potential interference between the tibial tunnel and osteotomy site or hardware, which can compromise graft fixation or tunnel integrity. Conventional sequencing often involves completing the osteotomy first, followed by arthroscopy and tunnel drilling. However, this approach risks hardware overlap with tunnel trajectories and difficulty in accurate tunnel positioning.
To mitigate these concerns, we propose a modified technique in which arthroscopic femoral and tibial tunnel drilling is completed before performing the medial open-wedge HTO. This sequence preserves optimal tunnel trajectory, avoids conflict with fixation hardware, and enables more controlled graft passage – especially when using suspensory devices or all-inside techniques. The technique aligns with evolving fixation strategies that prioritize bone preservation and precise tunnel orientation [6,7,8].
In this technical note, we describe our refined workflow for simultaneous ACLR and medial open-wedge HTO. We emphasize the rationale behind tunnel-first sequencing, detail the intraoperative steps, and outline key surgical tips to improve outcomes. We also provide a literature-based discussion contextualizing our approach within the existing body of evidence [1,2,3,4,5,6,7,8,9,10].
Indications
- ACL insufficiency with varus
- Age between 25 and 50
- Kellgren Lawrence Grade 1 and 2
- Revision ACL with secondary medial osteoarthritis (OA).
Contraindications
- Patients with concurrent lateral compartment OA
- Age above 50
- Multi-ligamentous injuries
- Patients unwilling to participate in the study.
Pre-operative long-leg standing radiographs are used to quantify varus deformity and plan correction. Magnetic resonance imaging is helpful in confirming ACL deficiency and assessing meniscal or chondral damage.
Patient positioning and setup
The procedure is performed under spinal or general anesthesia with the patient in a supine position on a radiolucent breakable orthopedic table. A high-thigh pneumatic tourniquet is applied to maintain a bloodless field. The operative leg is prepared and draped in a sterile fashion, allowing a full range of knee motion including hyperflexion. A lateral post is placed proximal to the knee to facilitate valgus stress application during the osteotomy phase. A C-arm is positioned contralaterally for optimal intraoperative fluoroscopic guidance.
A key intraoperative modification is the use of a breakable table, which enables intraoperative adjustment from flexion to extension during the switch between arthroscopic ACLR and osteotomy steps (Figs. 1 and 2).

Figure 1: Positioning with breakable table.

Figure 2: Empty notch showing deficient anterior cruciate ligament.
Arthroscopy and femoral tunnel preparation
Standard anterolateral viewing and anteromedial working portals are established. A diagnostic arthroscopy is performed to confirm ACL rupture and to assess the integrity of meniscal and chondral structures. Any intra-articular pathology, such as meniscal tears or loose bodies, is addressed at this stage.
With the knee hyperflexed (~120°), a transportal femoral tunnel is created using a flexible guidewire through the anteromedial portal. The tunnel is centered on the native ACL footprint on the lateral femoral condyle. A cannulated reamer matching the graft diameter is then used to ream the femoral tunnel to a depth of approximately 25–30 mm. A shuttle suture is passed through the tunnel to facilitate later graft passage.
Pearl
Performing femoral tunnel drilling at this stage is critical, as knee hyperflexion may be significantly limited following HTO due to osteotomy-related mechanical constraints (Fig. 3).

Figure 3: (a, b, c) showing femoral tunnel preparation and (d, e, f) showing tibial tunnel preparation.
Graft harvest and preparation
A vertical anteromedial incision is made approximately 1 cm medial and distal to the tibial tuberosity. The semitendinosus tendon (and gracilis if required) is harvested using a tendon stripper. Care is taken to avoid damage to the tibial tubercle or the planned proximal osteotomy site.
The tendon is quadrupled and prepared over two adjustable loop cortical buttons. The graft construct is pre-tensioned to 300 N for 2 min and checked for adequate length (minimum 6 cm for intra-articular and tunnel fill). The prepared graft is then kept in a moist sterile sponge until final passage (with or without antibiotic).
Tibial tunnel creation
Attention is turned to the tibial tunnel. A tibial ACL guide, set at 55°, is introduced via the medial portal and positioned at the center of the native ACL tibial footprint under arthroscopic visualization.
- A guidewire is drilled from the anterior cortex just medial to the tibial tuberosity, emerging at the prepared tibial ACL footprint.
- The tunnel is then reamed to match the graft diameter.
The resected cancellous bone from reaming is preserved to be packed into the tunnel at the end of the procedure.
Medial opening-wedge HTO
Through the same medial incision used for graft harvest, the subcutaneous tissue is dissected to expose the pes anserinus, which is retracted distally. The superficial medial collateral ligament is released subperiosteally and retracted posteriorly. A blunt retractor is placed posteriorly to protect the neurovascular structures during osteotomy (Fig. 4).

Figure 4: Incision and preparation for high tibial osteotomy.
Guidewire placement and osteotomy cuts
Two guidewires are inserted under fluoroscopy from the anteromedial tibial cortex ~5 cm below the medial joint line, aiming at the tip of the fibular head. This distal and posterior start point is purposefully chosen to avoid the tibial tunnel.
A biplanar osteotomy is then performed:
- A horizontal cut is made according to the surgeon’s preferred method by drilling holes with a drill bit and completing the osteotomy with the stacked osteotome technique or with an oscillating saw, parallel to the tibial slope, taking care to preserve a 1 cm lateral cortical hinge.
- An ascending anterior osteotomy cut, approximately 110° to the horizontal, is directed posterior to the patellar tendon insertion to prevent anterior tibial slope alteration and to maintain patellar height.
Osteotomy is gently opened using chisels or a calibrated wedge distractor to the predetermined correction angle (typically achieving 6–10 mm of opening based on mechanical axis planning). Alignment is verified by a long rod and fluoroscopic views to check the point of passage of the mechanical axis (Fig. 5).

Figure 5: (a and b) showing high tibial osteotomy guide wires in situ and (c and d) showing stacked osteotome technique.
Fixation with posteromedial plate
A C plate/TomoFix plate is used for osteotomy fixation and is placed on the posteromedial tibial cortex, rather than the traditional anteromedial location, to ensure unobstructed access for tibial tunnel graft passage.
- Posterior screws of the plate are inserted first to temporarily stabilize the osteotomy.
- To avoid convergence with the osteotomy screws, a metal dilator or cannulated sleeve is temporarily inserted into the tibial tunnel before placing the anterior screws of the osteotomy plate. This ensures the tunnel remains uncompromised during final screw insertion.
Pearl
Plate positioning is key – placing it too anteriorly can compromise the tibial tunnel, making drilling difficult or placing the graft at risk of impingement by screws. Placing a metal dilator in the tibial tunnel during anterior screws drilling avoids interference (Fig. 6).

Figure 6: (a and b) showing posterior fixation, (c and d) showing metal dilator inside tibial drill while anterior screw fixation.
Graft passage and fixation
The prepared graft is passed through the tibial tunnel into the femoral tunnel using the pre-placed shuttle sutures.
- The femoral cortical button is pulled through and flipped on the lateral cortex under direct arthroscopic visualization
- The graft is tensioned proximally to confirm secure femoral fixation
- With the knee in approximately 30° of flexion, the tibial end is tensioned and secured using an interference screw or cortical button, depending on surgeon preference.
The knee is cycled through a full range of motion to assess graft behavior and ensure there is no impingement or abnormal tension.
Finally, the preserved cancellous bone is packed into the tibial tunnel to reduce tunnel widening and promote biological incorporation.
The surgical field is thoroughly irrigated, hemostasis is secured, and all incisions are closed in layers using absorbable sutures. Sterile dressing is applied (Figs. 7 and 8, Table 1).

Figure 7: (a, b, c, d) showing final fluoroscopy shots and graft position with limb alignment.

Figure 8: Final post-operative X-rays showing anterior cruciate ligament with open wedge high tibial osteotomy.

Table 1: Technical modifications and key considerations
Simultaneous ACLR and HTO offers the advantage of addressing both instability and malalignment in a single-stage procedure, thereby reducing surgical morbidity, cost, and overall rehabilitation time, but remains technically challenging.
Neuschwander et al. and Noyes and Barber-Westin laid the groundwork by demonstrating that patients with combined ACL insufficiency and varus deformity could benefit significantly from a simultaneous procedure [1,2]. Their early observations were supported by Dejour et al., who advocated for valgus-producing osteotomy in ACL-deficient varus knees, particularly to reduce medial compartment load and improve functional outcomes [3]. Shortly after, Lattermann and Jakob emphasized that careful patient selection is crucial – especially in cases of chronic ACL deficiency with mild to moderate degenerative changes [4].
By 2002, Agneskirchner and Imhoff had published technical refinements to facilitate safer combined procedures. They highlighted key pearls such as preserving at least 1 cm of lateral cortex to avoid fractures and modifying plate positioning to accommodate tibial tunnels [5]. These modifications formed the basis for further technique adaptations.
One such adaptation is the technique we present here: performing ACL tunnel drilling before conducting the medial open-wedge osteotomy. This approach directly addresses concerns raised by multiple studies about tunnel-osteotomy interference. Performing tunnel drilling first ensures that tunnel orientation is anatomically correct and independent of metaphyseal distortion caused by osteotomy or implant placement.
Jin et al. published a prospective study involving 24 patients who underwent combined ACLR and open-wedge HTO. The authors reported significant functional improvements (Lysholm scores from 58 to 94), correction of the mechanical axis from a mean varus of 7° to a valgus of 1.2°, and maintenance of posterior tibial slope. However, some patients exhibited residual laxity and progression of OA, emphasizing the need for technical precision [7].
Recent biomechanical studies have reinforced the importance of posterior tibial slope in ACL graft strain and failure. Mal-reduction or excessive slope alteration during HTO may lead to anterior tibial translation and excessive graft load. This concern is echoed in technique-focused publications, including work by Toofan et al., who described simultaneous ACLR and HTO using double suspensory fixation. Their findings supported improved graft integrity and lower tunnel widening when suspensory fixation is used appropriately [8].
Performing tunnel drilling before osteotomy enables preservation of bone stock, prevents cortical violation, and facilitates anatomic graft passage – especially when using modern devices. It also allows safe planning of plate and screw placement without compromising graft integrity.
Nonetheless, our technique is not without limitations. It demands careful pre-operative planning, intraoperative fluoroscopy, and meticulous execution. Protecting the pre-drilled tunnels during osteotomy requires experience and precision. Furthermore, while theoretical advantages are clear, long-term comparative data are needed to validate clinical superiority over traditional methods.
Simultaneous ACLR with medial opening wedge HTO is a reliable, efficient technique for restoring knee stability while correcting varus malalignment. With meticulous attention to surgical sequence, tunnel orientation, and plate positioning, this combined procedure can provide durable outcomes, prevent graft overloading, and delay progression of medial compartment OA.
In ACL-deficient varus knees, combining ACLR with HTO in a single stage offers the dual advantage of correcting alignment and restoring stability, thereby improving function and reducing long-term degenerative risk. Careful execution of key technical steps – particularly tunnel drilling before osteotomy and posteromedial plate placement – ensures reproducible and safe outcomes.
References
- 1. Neuschwander DC, Drez D Jr., Paine RM. Simultaneous high tibial osteotomy and ACL reconstruction for combined genu varum and symptomatic ACL tear. Orthopedics 1993;16:679-84. [Google Scholar] [PubMed]
- 2. Noyes FR, Barber-Westin SD. High tibial osteotomy and ligament reconstruction in varus angulated, anterior cruciate ligament-deficient knees. A two- to seven-year follow-up study. Am J Sports Med 1993;21:2-12. [Google Scholar] [PubMed]
- 3. Dejour H, Neyret P, Boileau P, Donell ST. Anterior cruciate reconstruction combined with valgus tibial osteotomy. Am J Sports Med 1994;299:220-8. [Google Scholar] [PubMed]
- 4. Lattermann C, Jakob RP. High tibial osteotomy alone or combined with ligament reconstruction in anterior cruciate ligament-deficient knees. Knee Surg Sports Traumatol Arthrosc 1996;4:32-8. [Google Scholar] [PubMed]
- 5. Agneskirchner JD, Imhoff AB. Simultaneous ACL replacement and high tibial osteotomy: Indication, technique, results. Tech Knee Surg 2002;1:146-54. [Google Scholar] [PubMed]
- 6. Marriott KA, Birmingham TB, Kean CO, Hui C, Jenkyn TR, Giffin JR. Five-year changes in gait biomechanics after concomitant high tibial osteotomy and ACL reconstruction in patients with medial knee osteoarthritis. Am J Sports Med 2015;43:2277-85. [Google Scholar] [PubMed]
- 7. Jin C, Song EK, Jin QH, Lee NH, Seon JK. Outcomes of simultaneous high tibial osteotomy and anterior cruciate ligament reconstruction in anterior cruciate ligament deficient knee with osteoarthritis. BMC Musculoskelet Disord 2018;19:228. [Google Scholar] [PubMed]
- 8. Toofan H, Tabatabaei Irani P, Ghadimi E, Firoozabadi MA, Mortazavi SM. Simultaneous arthroscopic anterior cruciate ligament reconstruction using double suspensory technique and medial open-wedge, high tibial osteotomy. Arthrosc Tech 2022;11:e2357-64. [Google Scholar] [PubMed]
- 9. Lubowitz JH, Schwartzberg R, Smith P. Randomized controlled trial comparing all-inside anterior cruciate ligament reconstruction technique with anterior cruciate ligament reconstruction with a full tibial tunnel. Arthroscopy 2013;29:1195-200. [Google Scholar] [PubMed]
- 10. Mayr R, Smekal V, Koidl C, Coppola C, Eichinger M, Rudisch A, et al. ACL reconstruction with adjustable-length loop cortical button fixation results in less tibial tunnel widening compared with interference screw fixation. Knee Surg Sports Traumatol Arthrosc 2020;28:1036-44. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2025 Combined Arthroscopic Anterior Cruciate Ligament Reconstruction and Distal Femoral Osteotomy in a Patient of Bilateral Genu Valgum – A Rare Case Report
February 1, 2025 Combined Arthroscopic Anterior Cruciate Ligament Reconstruction and Distal Femoral Osteotomy in a Patient of Bilateral Genu Valgum – A Rare Case Report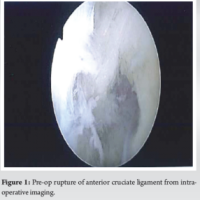 July 10, 2024 Bilateral Anterior Cruciate Ligament Reconstruction with All-Inside Technique for Adolescent: A Review of the Literature and Case Report
July 10, 2024 Bilateral Anterior Cruciate Ligament Reconstruction with All-Inside Technique for Adolescent: A Review of the Literature and Case Report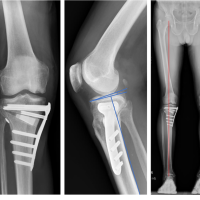 December 10, 2022 Medial Meniscus Posterior Root Reconstruction and Open-Wedge High Tibial Osteotomy for Medial Meniscus Posterior Root Tear with Varus Knee: A Case Report
December 10, 2022 Medial Meniscus Posterior Root Reconstruction and Open-Wedge High Tibial Osteotomy for Medial Meniscus Posterior Root Tear with Varus Knee: A Case Report March 1, 2026 Femoral-Sided Avulsion Fracture Treated with a Novel Arthroscopic Physeal-Sparing Method in a Skeletally Immature Patient
March 1, 2026 Femoral-Sided Avulsion Fracture Treated with a Novel Arthroscopic Physeal-Sparing Method in a Skeletally Immature Patient