
Aneurysmal bone cyst of the talus is exceptionally rare; it ABC usually involves metaphyseal regions of long bones. Percutaneous polidocanol sclerotherapy offers an excellent conservative modality, allowing sequential outpatient injections while avoiding the complications of open curettage and bone grafting.
Faisal Harun, Department of Orthopaedic Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. E-mail: dr.faisalharun@gmail.com
Introduction: Aneurysmal bone cysts (ABCs) are most commonly found in the metaphysis of long bones but are reported to have been found in other locations as well. While presentation of a swelling in a short bone is unlikely to be an ABC, the possibility should be kept in mind, especially with supporting radiological findings.
Case Report: In this case report, we present the case of a young female who presented to us with complaints of pain and swelling over the dorsal aspect of her right foot. Radiological investigations pointed toward a diagnosis of ABC of the talus bone, which was confirmed on histopathological examination. The patient was managed conservatively using percutaneous polidocanol injection and was relieved of her symptoms soon after.
Conclusion: Although ABC is most commonly found in long bones, it can be considered a differential in other bones as well. Sclerotherapy may be considered over curettage as a treatment modality due to its numerous advantages.
Keywords: Aneurysmal bone cyst, talus, sclerotherapy, polidocanol.
Aneurysmal bone cysts (ABCs) are a benign lesion of the bone that can occur in any bone, but it is more commonly located in the metaphysis of long bones, especially weight-bearing ones [1]. The most common sites are the distal femur, proximal tibia, proximal humerus, and spine. It is more common in females and usually occurs during the second decade of life [2]. Although quite rare, ABCs may occur in other bones as well. Such a case is presented in the case report, where a young female with painfully swelling over the dorsum of her foot was diagnosed as a case of ABC of talus and was managed conservatively using sclerotherapy by percutaneous polidocanol injection, with complete relief of symptoms.
A 32-year-old female presented with complaints of pain and swelling in the dorsum of her foot. The swelling was insidious in onset and was noticed by the patient while bathing and was the size of a pea. It was associated with pain, which was insidious in onset, dull aching in nature, mild to moderate in intensity, with no aggravating or relieving factors, not radiating to any other site, and not relieved by rest. There was no history of trauma as well. Clinical examination revealed the swelling to be hard, attached to the underlying structure, not attached to the overlying skin, non-mobile, non-tender and with no erythema or local rise of temperature. There was no appreciable change in size since the patient had first noticed the swelling. X-rays and magnetic resonance imaging (MRI) were advised to the patient for the same and conservative management was advised (Fig. 1, 2).
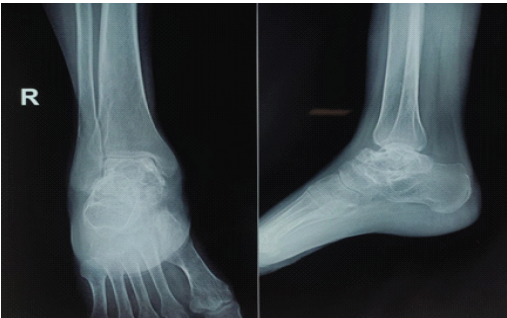
Figure 1: Radiograph of right foot of the patient in anteroposterior and lateral view, showing multiple cystic lesions of the talus.
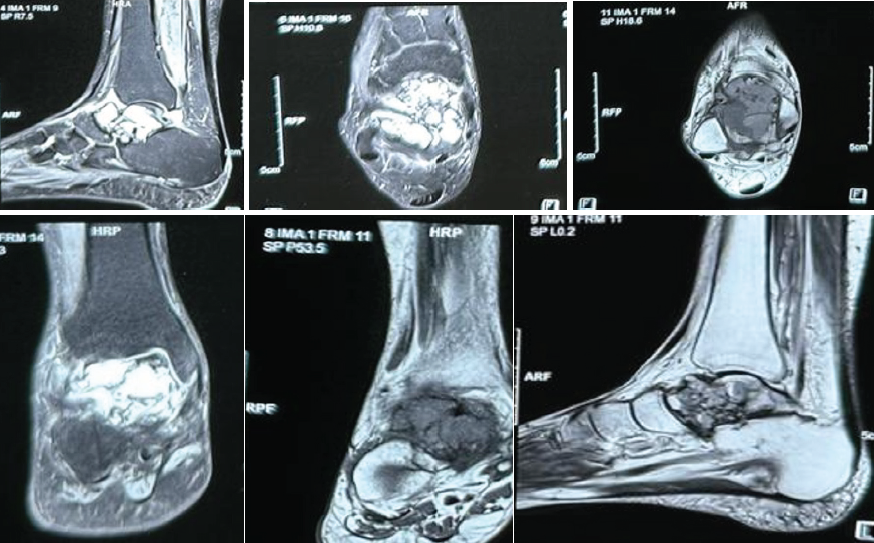
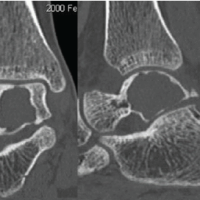
Figure 2: Magnetic resonance imaging of the right foot showing large irregular multiloculated expansile cystic lesion measuring approximately 4.1 × 3.1 × 2.2 cm, involving the talar dome and neck reaching up to the anterior articular surface. The lesion appears as heterogeneously hyperintense on T2/short tau inversion recovery images and iso to hypointense on T1-weighted image with multiple intrinsic thick enhancing septae causing loculation with multiple intrinsic blood-fluid level.
X-Rays of the foot of the patient showed a lytic lesion of the right talus bone. A contrast-enhanced MRI was also advised, which showed a large irregular multiloculated expansile cystic lesion, measuring approximately 4.1 × 3.1 × 2.2 cm, involving the talar dome and neck reaching up to the anterior articular surface. The lesion appeared as heterogeneously hyperintense on T2/Short tau inversion recovery images and iso to hypointense on T1-weighted images with multiple intrinsic thick enhancing septae causing loculation with multiple intrinsic blood-fluid levels, suggestive of ABC, and histopathological and clinical correlation was advised. Upon follow-up, image-guided fine needle aspiration cytology (FNAC) and biopsy of the patient were done. The FNAC was suggestive of few scattered multinucleated giant cells along with few degenerated cells against hemorrhagic background, likely a benign lesion (Fig. 3). The biopsy result reported fragmented bone tissue with hemorrhagic cystic spaces lined by osteoclastic giant cells and mononuclear cells with mild anisonucleosis with two possible differentials: Giant cell tumor and ABC, both being quite rare in the talus.
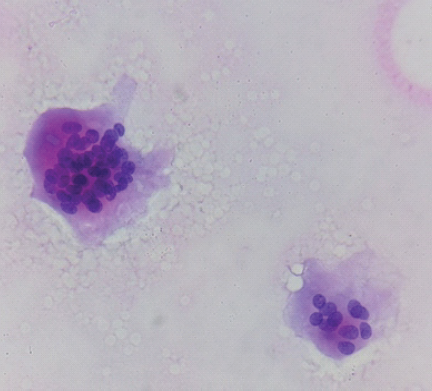
Figure 3: Fine needle aspiration cytology smears showing scattered multinucleated giant cells in a hemorrhagic background.
For differentiating between the two, immunohistochemistry of the sample was advised. Two markers were considered, namely Ki67 and S100. Ki67 is a cell proliferation marker that corresponds to a nuclear non-histone protein expressed by cells in the proliferative phase. There is a good relationship between Ki67 staining and mitotic count. Ki67 along with proliferating cell nuclear antigen marker is used for the evaluation of proliferative activity in paraffin-embedded material. S100 is a calcium-binding protein composed of different combinations of alpha and beta subunits. It is present in the nucleus and cytoplasm of glial and Schwann cells, melanocytes, chondrocytes, adipocytes, and myoepithelial cells. All tumors derived from these cells are positive for S100. It has both nuclear and cytoplasmic localization and the main use is in the evaluation of peripheral nerve sheath and melanocytic tumors. The results came out to be an 8–10% positive for Ki67 and no immunoreactivity with S100 favoring the differential diagnosis of ABC (Fig. 4).
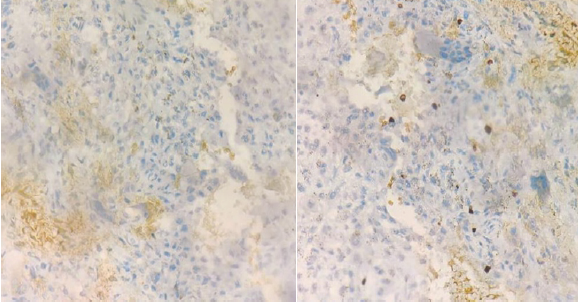
Figure 4: Immunohistochemistry images, showing (a) Ki67 positive and (b) S100 and H3G34W negative slides.
On follow-up, fluid from the lesion was aspirated under image guidance, and polidocanol injection was administered percutaneously at a dose of 3 mL/kg. The patient was advised full weight bearing along with oral analgesics and antibiotics. The patient showed improvement in pain and a decrease in the size of swelling 1 month later (Fig. 5). The polidocanol injection was repeated twice after a period of 6 months. After 2 years of follow-up, the patient had resolution of the swelling and minimal pain (Fig. 6).

Figure 5: 2-month follow-up radiograph of the right foot of the patient in anteroposterior and lateral view, showing sclerosis of the talus.
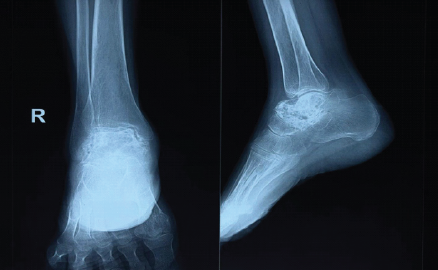
Figure 6: 2-year follow-up radiograph of the right foot of the patient in anteroposterior and lateral view, showing sclerosis of the talus.
ABC is a benign cystic lesion of bone with blood-filled spaces separated by septations containing fibroblasts, osteoclast-type giant cells, and reactive woven bone [2]. ABC usually occurs in the first two decades and has no sex predilection, although some studies report more incidence in females. The prevalence is 1.4 cases/100,000 individuals/year. It most commonly affects the long bones, especially the metaphysis region of the femur and tibia [1,3]. Although rare, ABCs have been located in all the parts of foot, including the talus [4]. Within the talus itself, the most common tumor is intra-osseous ganglion cysts [5]. On X-rays, it appears as an expansile, lytic bone lesion of the metaphyseal region with cortical thinning and subperiosteal new bone formation. Characteristic findings in MRI are multiple fluid-fluid levels and soft tissue expansion, while solid soft tissue component within the lesion is suggestive of secondary ABC [6]. Biopsy is routinely used for the confirmation of the lesion and is considered the diagnostic gold standard [7]. The treatment modalities for ABC range from bone curettage, en bloc, excision, arterial embolization, bone marrow injections, intralesional steroid injections, radiation therapy, cryotherapy, denosumab injection, and sclerotherapy [2]. What complicates the treatment is the fact that recurrence of ABCs may be as high as 90% in a 2-year follow-up period [8]. Bone curettage supplemented with bone grafting is the most common modality practiced, but rates of recurrence are quite high, ranging from 10%-30% [9,10]. En bloc resection, though associated with the lowest rates of recurrence, is not always feasible due to anatomical constraints as well as the high level of associated deformity. Given its cost-effectiveness and minimal invasive approach, sclerotherapy is feasible, cosmetically appealing, and economical for the patient as well [2]. The limitations of this case report reside in the need for a long period of follow-up for the long-term complications, such as osteoarthritis, as no such complaints were present in this patient after 2 years. Moreover, there have been concerns regarding post-procedural collapse of the talus; however, no such incidence has been reported in the literature following the use of Polidocanol in the management of ABC of the lower limbs.
ABCs, though unlikely, can occur in places other than the long bones of the body. Immunohistochemistry may help confirm the diagnosis when other modalities fail to. The condition can be managed using various methods, ranging from radical techniques such as en bloc resection to conservative methods such as injection of sclerosing agents. The location and extent of the lesion may be considered while choosing the treatment modality.
This article highlights the possibility of aneurysmal bone cyst being the cause of bony swellings in locations apart from long bones and the management options in such cases.
References
- 1. Kumar D, Kumar S, Kumar D, Patel BM, Kumar A, Kumar S, et al. Sclerotherapy for aneurysmal bone cyst: A single-center experience. Cureus 2021;13:e18469. [Google Scholar] [PubMed]
- 2. Leithner A, Windhager R, Lang S, Haas OA. Aneurysmal bone cyst. A population based epidemiologic study and literature review. Clin Orthop Relat Res 1999;363:176-9. [Google Scholar] [PubMed]
- 3. Fletcher CD, Unni KK, Mertens F. World Health Organization Classification of Tumours. Pathology and of Tumours of Soft Tissue, Genetics. Lyon: IARC Press; 2002. [Google Scholar] [PubMed]
- 4. Pollandt K, Werner M, Delling G. Tumoren des fussskeletts – ein erfahrungsbericht des hamburger-knochentumorregisters [Tumors of the footbones- a report from the Hamburg bone tumor registry]. Z Orthop Ihre Grenzgeb 2003;141:445-51. [Google Scholar] [PubMed]
- 5. Sharma S, Gupta P, Sharma S, Singh M, Singh D. Primary aneurysmal bone cyst of talus. J Res Med Sci 2012;17:1192-4. [Google Scholar] [PubMed]
- 6. Boubbou M, Atarraf K, Chater L, Afifi A, Tizniti S. Aneurysmal bone cyst primary about eight pediatric cases: Radiological aspects and review of the literature. Pan Afr Med J 2013;28:15. [Google Scholar] [PubMed]
- 7. Puthoor D, Francis L, Ismail R. Is sclerotherapy with polidocanol a better treatment option for aneurysmal bone cyst compared to conventional curettage and bone grafting? J Orthop 2021;25:265-70. [Google Scholar] [PubMed]
- 8. Batisse F, Schmitt A, Vendeuvre T, Herbreteau D, Bonnard C. Aneurysmal bone cyst: A 19-case series managed by percutaneous sclerotherapy. Orthop Traumatol Surg Res 2016;102:213-6. [Google Scholar] [PubMed]
- 9. Topouchian V, Mazda K, Hamze B, Laredo JD, Pennecot GF. Aneurysmal bone cysts in children: Complications of fibrosing agent injection. Radiology 2004;232:522-6. [Google Scholar] [PubMed]
- 10. Guibaud L, Herbreteau D, Dubois J, Stempfle N, Bérard J, Pracros JP, et al. Aneurysmal bone cysts: Percutaneous embolization with an alcoholic solution of zein – series of 18 cases. Radiology 1998;208:369-73. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report
September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report October 1, 2024 Sclerotherapy as a Primary or Salvage Procedure for Aneurysmal Bone Cyst: A Case Report
October 1, 2024 Sclerotherapy as a Primary or Salvage Procedure for Aneurysmal Bone Cyst: A Case Report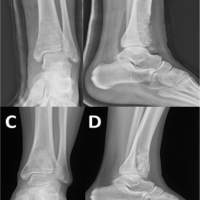 June 10, 2024 Response of Recurrent Aggressive Aneurysmal Bone Cyst of Distal Tibia to Denosumab Treatment
June 10, 2024 Response of Recurrent Aggressive Aneurysmal Bone Cyst of Distal Tibia to Denosumab Treatment January 10, 2021 A Rare Case of Aneurysmal Bone Cyst – Navicular Bone Treated by Intralesional Sclerotherapy Agent Polidocanol
January 10, 2021 A Rare Case of Aneurysmal Bone Cyst – Navicular Bone Treated by Intralesional Sclerotherapy Agent Polidocanol