
The “J Technique” is a novel, arthroscopic anchorless transosseous rotator cuff repair that eliminates the cost of suture anchors, offering a significant economic advantage without compromising biomechanical stability.
Dr. Abdulla Harafan, Department of Orthopaedics, Malabar Medical College, Kozhikode, Kerala, India. E-mail: abdullaharafan123@gmail.com
Introduction: Rotator cuff tears are a common cause of shoulder disability, often requiring surgical repair. The high cost of suture anchors presents a significant economic burden, driving the need for cost-effective alternatives like transosseous repairs. This paper details a novel arthroscopic anchorless technique utilizing an anterior cruciate ligament (ACL) jig with the “J Technique” to provide a biomechanically sound and economically advantageous solution.
Case Report: We present a technique for arthroscopic anchorless rotator cuff repair (RCR). Standard arthroscopic portals are established. An ACL jig is introduced to guide the creation of a precise transosseous tunnel in the greater tuberosity using a 4.5 mm cannulated reamer. Suture strands (FiberWire and FiberTape) are passed through the tunnel and the rotator cuff tendon. The sutures are tied with SMC sliding knots, strategically placing the post to ensure knots settle at the lower tunnel exit, forming an inverted “J” configuration that secures the tendon to its footprint.
Conclusion: The arthroscopic anchorless “J Technique” using an ACL jig is a reproducible and cost-effective surgical alternative for RCR. It provides robust fixation, minimizes hardware-related risks, and prevents subacromial impingement through strategic knot management, offering a valuable option for surgeons seeking to control costs without compromising stability.
Keywords: Arthroscopy, rotator cuff, anterior cruciate ligament jig, J technique, anchorless repair, transosseous, cost-effective.
Rotator cuff tears are a common orthopedic pathology causing significant shoulder pain and disability, particularly in individuals over 50 years of age, with surgical intervention often necessitated for full-thickness tears that do not respond to conservative management [1]. While various surgical techniques have been developed for rotator cuff repair (RCR), including single-row and double-row fixation methods, many approaches are challenged by high material costs, particularly those relying on suture anchors [2,3]. However, the economic burden of these implants can be substantial, driving the exploration of alternative, more affordable strategies like transosseous repairs [1,4]. While transosseous cuff repair techniques have shown promise in reducing costs, their widespread adoption has sometimes been limited by the need for specialized jigs or technical difficulties that increase surgical time [5]. This paper details an arthroscopic anchorless RCR utilizing an anterior cruciate ligament (ACL) jig and a novel “J technique,” which offers a cost-effective and biomechanically sound alternative to conventional anchor-based repairs by eliminating the need for expensive implants while simplifying the transosseous drilling process. This technique aims to provide a robust repair that is comparable in strength to double-row anchor repairs, but at a significantly lower cost due to the elimination of anchor implants [1]. The utilization of an ACL jig in this context significantly streamlines the transosseous tunnel creation, offering an accessible and repeatable method for achieving the necessary bone bridge for suture passage. This technical note describes the procedural steps of this arthroscopic anchorless RCR, emphasizing its advantages in terms of cost-efficiency and biomechanical stability.
The surgical technique commences with the patient positioned in the lateral decubitus position, followed by the establishment of standard arthroscopic portals to facilitate diagnostic evaluation and subsequent repair [6]. After a comprehensive diagnostic arthroscopy, typically performed through the standard posterior viewing portal, the surgeon evaluates the extent of the rotator cuff tear and any associated pathologies. We then proceed to clear the subacromial space thoroughly, ensuring optimal visualization of the massive rotator cuff tear to be addressed (Fig. 1).
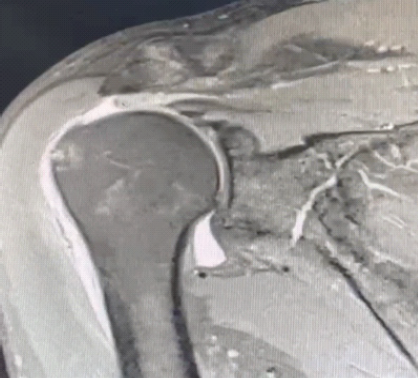
Figure 1: Magnetic resonance imaging showing full-thickness tear of supraspinatus and infraspinatus tendon with grade 2 retraction.
An ACL jig, equipped with a tip aimer, is then meticulously introduced through the lateral portal, with a far lateral portal subsequently created to precisely guide the bullet of the ACL jig for accurate tunnel placement. A beath pin is then drilled with precision to ensure its exit at the humeral ridge, establishing the exact trajectory for the subsequent reaming process (Fig. 2).

Figure 2: Beath pin drilled through anterior cruciate ligament jig.
Over this beath pin, a 4.5 mm cannulated reamer is meticulously utilized to create a bone tunnel, through which a Prolene shuttle loop is subsequently passed and retrieved into the joint, facilitating suture management (Fig. 3 and 4).
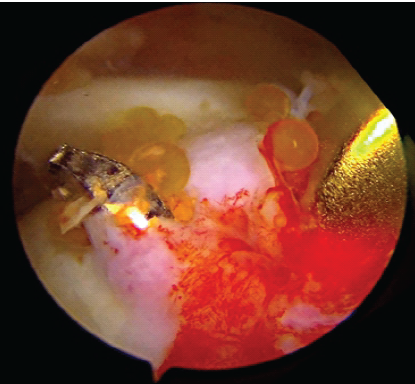
Figure 3: Beath pin exiting at humerus ridge.
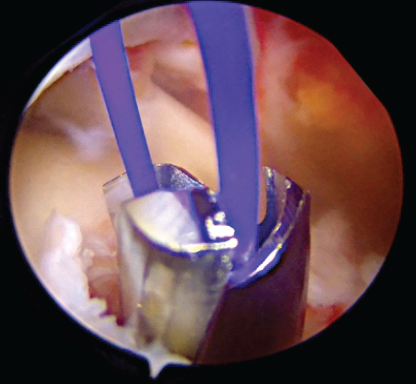
Figure 4: Prolene loop shuttle.
This loop is then used to pass the definitive sutures, which are strategically arranged to create a strong construct for tendon reattachment. For cost-effectiveness, one FiberWire and one FiberTape are bifurcated, yielding four individual strands. Hence, in total, we now have two FiberTapes and two FiberWires in the tunnel [7,8]. Using the FirstPass device, four distinct bites are taken in succession through the cuff tissue to ensure broad and secure fixation [7]. From the far lateral portal, a knot pusher is then meticulously employed to shuttle each suture end into the joint, after which the sutures are retrieved through the lateral portal. Each suture is then tied sequentially using SMC sliding knots, ensuring that the thread(FiberWire/FiberTape) exiting inferiorly is maintained as the post for the SMC sliding knot so that the knot will be at the lower tunnel exit, preventing any subacromial knot impingement. The final FiberWire configuration distinctly resembles an inverted “J,” thereby securely reapproximating the rotator cuff to its anatomical footprint and completing the fixation [1,6,9,10] (Fig. 5 and 6).
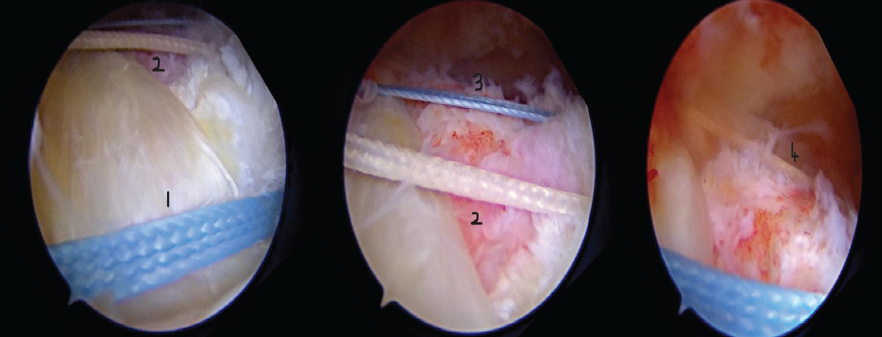
Figure 5: Final repair.
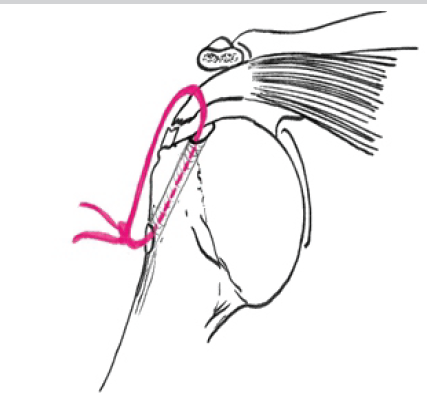
Figure 6: Illustration showing inverted J configuration of suture.
The J technique optimizes tendon-to-bone contact and provides a stable repair construct, which is crucial for promoting healing and preventing retear. This transosseous repair method, by avoiding anchors, minimizes hardware-related complications and potentially reduces overall operative time and cost, a significant advantage over conventional anchor-based techniques [1]. The strategic placement of the knots at the lower tunnel exit, as opposed to the subacromial region, further minimizes the risk of impingement and subsequent irritation [11]. This approach also enhances the biological environment for healing by maximizing tendon-bone contact without the interposition of foreign materials associated with traditional anchors and associated anchor-related complications [7].
This cost-effective and biomechanically sound technique offers a promising alternative to traditional anchor-based repairs, especially given the rising costs of surgical implants [1]. The “J technique” specifically addresses concerns regarding the economic burden of RCR by eliminating the need for expensive suture anchors, while still aiming for robust biomechanical stability comparable to or exceeding that of double-row anchor constructs [12]. This method emphasizes a transosseous approach, which has historically demonstrated favorable biological healing environments due to broader tendon-to-bone contact and compression, potentially leading to improved rates of tendon healing [7]. Furthermore, by leveraging an ACL jig for precise tunnel creation, the technique mitigates the technical challenges often associated with transosseous repairs, making it more reproducible and accessible to a broader range of surgeons [1]. This innovative approach also minimizes the potential for implant-related complications, such as anchor pull-out or chondral damage, which can occur with conventional methods. Indeed, the absence of hardware further reduces the risk of infection and avoids foreign body reactions, thereby improving patient outcomes and potentially shortening recovery times [13]. Moreover, the reduced hardware inventory streamlines the surgical workflow and can lead to significant cost savings in healthcare systems [14]. The J technique, while innovative, warrants further biomechanical and clinical investigation to rigorously compare its long-term efficacy and re-tear rates against established anchor-based repairs [2]. While double-row repairs typically exhibit superior biomechanical properties compared to single-row repairs, the cost implications and long-term efficacy of various techniques remain subjects of ongoing debate [15]. However, our technique, by creating a strong construct with multiple sutures inside the tunnel and an inverted J configuration, aims to restore normal biomechanics and facilitate healing of the delaminated rotator cuffs, similar to transosseous equivalent repairs [7,16,17]. The economic burden of traditional arthroscopic RCRs, largely driven by the high cost of suture anchors, necessitates exploration of such cost-effective alternatives [2].
The arthroscopic anchorless RCR with ACL jig using the “J Technique” is a reproducible, cost-effective, and biomechanically viable surgical alternative. It effectively addresses the economic concerns associated with anchor-based repairs while providing robust fixation and minimizing implant-related complications. This technique is a promising option for surgeons aiming to provide high-quality care while controlling costs.
This arthroscopic anchorless “J Technique” provides orthopedic surgeons with a reliable and cost-effective method for rotator cuff repair by utilizing a common ACL jig to create a transosseous tunnel, eliminating the need for expensive suture anchors and avoiding subacromial knot impingement through strategic suture management.
References
- 1. Hafez MR, El Shewy MT, El-Singergy AA, Hashem MO, Zawam SH. Arthroscopic Modified Trans-Osseous Rotator Cuff Repair Using the Giant Needle Technique and Racking Hitch Knot. Research Square [Preprint]; 2023. [Google Scholar] [PubMed]
- 2. Rhode BA, Rhode WS. Cost comparison of rotator cuff repair between double and triple loaded anchors. MOJ Orthop Rheumatol 2016;4:00161. [Google Scholar] [PubMed]
- 3. Su-Bao D, Zhang B, Luo H, Liu Y, Chen-Li R, Zou Y, et al. Single knotless-anchor with two ethicon 2# for Ellman grade III bursal-side partial thickness rotator cuff tears: A cadaveric biomechanical study and short-term clinical evaluation. BMC Musculoskelet Disord 2023;24:701. [Google Scholar] [PubMed]
- 4. Yan Y, Chen C, Fang C, Yu G, Wu D, Wang YM, et al. The Y-loop for double-row rotator cuff repair: An all-arthroscopic technique. Arthrosc Tech 2025;11:103860. [Google Scholar] [PubMed]
- 5. Burns KA, Robbins L, LeMarr AR, Childress AL, Morton DJ, Wilson ML. Rotator cuff repair with knotless technique is quicker and more cost-effective than knotted technique. Arthrosc Sports Med Rehabil 2019;1:e123-30. [Google Scholar] [PubMed]
- 6. Sanders B. Novel reusable transosseous tunnel based soft tissue repair techniques about the shoulder: A rational, value based approach. MOJ Orthop Rheumatol 2016;5:00164. [Google Scholar] [PubMed]
- 7. Oishi S, Agranovich O, Zlotolow D, Wall L, Stutz C, Pajardi G, et al. Treatment and outcomes of arthrogryposis in the upper extremity. Am J Med Genet C Semin Med Genet 2019;181:363-71. [Google Scholar] [PubMed]
- 8. Büyükdoğan K, Koyuncu Ö, Eren İ, Birsel O, Fox MA, Demirhan M. Arthroscopic knotless separate layer transosseous equivalent repair of delaminated rotator cuff tears. J Shoulder Elbow Surg. 2021;30:e447. [Google Scholar] [PubMed]
- 9. Dyrna F, Voß A, Pauzenberger L, Obopilwe E, Mazzocca AD, Castagna A, et al. Biomechanical evaluation of an arthroscopic transosseous repair as a revision option for failed rotator cuff surgery. BMC Musculoskelet Disord 2018;19:240. [Google Scholar] [PubMed]
- 10. Dimmen S, Owesen C, Lundgreen K, Jenssen KK. No difference in clinical outcome after rotator cuff repair performed within or later than 3 months after trauma: A retrospective cohort study. Knee Surg Sports Traumatol Arthrosc 2022;31:672.-80. [Google Scholar] [PubMed]
- 11. Mo X, Shen J, Jiang W, Zhang X, Zhou N, Wang Y, et al. Percutaneous endoscopic lumbar diskectomy for axillar herniation at l5-s1 via the transforaminal approach versus the interlaminar approach: A prospective clinical trial. World Neurosurg 2019;125:e508-14. [Google Scholar] [PubMed]
- 12. Ju CI. Technical considerations of the transforaminal approach for lumbar disk Herniation. World Neurosurg 2020;145:597-611. [Google Scholar] [PubMed]
- 13. Hironaka Y, Morimoto T, Motoyama Y, Park YS, Nakase H. Surgical management of minimally invasive anterior lumbar interbody fusion with stand-alone interbody cage for l4-5 degenerative disorders: Clinical and radiographic findings. Neurol Med Chir (Tokyo) 2013;53:861-9. [Google Scholar] [PubMed]
- 14. Gad AM, Zawam SH. Arthroscopic biceps tenodesis using press-fit bony plug: A case series study. Int Orthop 2024;48:785-92. [Google Scholar] [PubMed]
- 15. Fedorka CJ, Etges AP, Best MJ, Liu HH, Zhang X, Sanders B, et al. Defining the cost of arthroscopic rotator cuff repair: A multicenter, time-driven activity-based costing and cost optimization investigation. J Bone Joint Surg Am 2025;107:9-15. [Google Scholar] [PubMed]
- 16. Derwin KA, Sahoo S, Zajichek A, Strnad G, Spindler KP, Iannotti JP, et al. Tear characteristics and surgeon influence repair technique and suture anchor use in repair of superior-posterior rotator cuff tendon tears. J Shoulder Elbow Surg 2019;28:227-36. [Google Scholar] [PubMed]
- 17. Solomon DJ. Editorial commentary: Cost associated with arthroscopic rotator cuff repair can be largely controlled by the surgeon. Arthroscopy 2021;37:1084-5. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Superior Capsular Reconstruction Using Biceps Tendon Autograft with Novel Biceps Tenodesis Arthroscopic Fixation: A Case Report
November 1, 2025 Superior Capsular Reconstruction Using Biceps Tendon Autograft with Novel Biceps Tenodesis Arthroscopic Fixation: A Case Report December 10, 2023 Osteonecrosis of the Humeral Head Following Arthroscopic Repair of Rotator Cuff Tears: A Case Report
December 10, 2023 Osteonecrosis of the Humeral Head Following Arthroscopic Repair of Rotator Cuff Tears: A Case Report March 1, 2026 Femoral-Sided Avulsion Fracture Treated with a Novel Arthroscopic Physeal-Sparing Method in a Skeletally Immature Patient
March 1, 2026 Femoral-Sided Avulsion Fracture Treated with a Novel Arthroscopic Physeal-Sparing Method in a Skeletally Immature Patient March 1, 2026 Clinical Outcome of Arthroscopic Anterior Cruciate Ligament Reconstruction with Simultaneous Meniscus Repair
March 1, 2026 Clinical Outcome of Arthroscopic Anterior Cruciate Ligament Reconstruction with Simultaneous Meniscus Repair