
A staged orthoplastic approach using vascularized fibular grafting and tibiocalcaneal arthrodesis enables effective limb salvage in complex distal tibial atrophic pseudoarthrosis.
Dr. David Mayorga Naranjo, Department of Ortophedics and Traumatology, Hospital Universitari i Politécnic La Fe, Valencia, España. E-mail: drdavidmayorga@gmail.com
Introduction: Tibial pseudoarthrosis is an uncommon but serious complication following high-energy trauma, particularly in complex distal tibial fractures such as pilon fractures. Atrophic pseudoarthrosis, characterized by avascular bone ends and a lack of biological activity, is often associated with risk factors such as smoking, soft-tissue damage, and multiple surgical interventions. Its management is particularly challenging, requiring a tailored approach that restores both mechanical stability and the biological environment for bone healing. Orthoplastic strategies have emerged as essential in cases with significant bone loss and compromised soft-tissue coverage.
Case Report: We present the case of a 42-year-old male, a chronic smoker, who sustained a comminuted pilon fracture and fibular shaft fracture following a fall. Initial management included external fixation, followed by open reduction and internal fixation, and subsequent application of a hexapod fixator due to delayed healing. Persistent non-union and soft tissue compromise led to multiple reconstructive procedures, including autologous bone grafting and an anterolateral thigh free flap. Eleven months after the initial injury, the patient was referred to our orthoplastic unit. Diagnostic studies confirmed atrophic pseudoarthrosis of the distal tibia. A two-stage surgical approach was undertaken: First, debridement and placement of an antibiotic-impregnated cement spacer; second, tibiocalcaneal arthrodesis with an intramedullary nail and reconstruction using a contralateral free fibular flap. Post-operative recovery was favorable, with early signs of consolidation and good functional outcomes.
Conclusion: This case underscores the importance of a multidisciplinary, staged approach in managing complex tibial pseudoarthrosis. Orthoplastic collaboration enables successful limb salvage by addressing both osseous and soft tissue challenges, optimizing conditions for definitive bone healing and functional restoration.
Keywords: Atrophic pseudoarthrosis, orthoplastic surgery, tibiocalcaneal arthrodesis.
Tibial pseudoarthrosis is a rare but severe complication following high-energy trauma to the lower extremity, particularly in fractures involving the distal tibial metaphysis, such as pilon fractures. It represents a significant clinical challenge due to its multifactorial etiology, including biological, mechanical, and systemic contributors that interfere with normal bone healing [1]. Atrophic pseudoarthrosis, in particular, denotes a non-viable state of the bone ends and is typically associated with poor vascularity, soft-tissue damage, and comorbid conditions such as smoking or infection. Management requires not only a thorough understanding of bone biology and biomechanics but also a comprehensive and multidisciplinary treatment strategy that addresses both skeletal and soft tissue deficits [1,2].
Orthoplastic approaches, which integrate orthopedic and plastic surgical expertise, have gained increasing relevance in the treatment of complex non-union and limb salvage procedures. These allow for simultaneous skeletal reconstruction and soft tissue coverage, which is especially critical in cases with segmental bone loss and compromised vascularized envelopes [2,3].
In this report, we present a complex case of distal tibial atrophic pseudoarthrosis in a smoker, managed with staged surgical debridement, hexapod fixation, vascularized bone transfer, and tibiocalcaneal arthrodesis, highlighting the key principles and advantages of a multidisciplinary approach.
A 42-year-old male, smoker, with no known drug allergies, sustained a comminuted pilon fracture of the left tibia and a diaphyseal fracture of the left fibula (Fig. 1) after falling from a ladder from a height of approximately 1.5 m. He initially underwent emergency surgery with closed reduction and placement of a monolateral external fixator on the tibia.

Figure 1: Initial bone injury of the patient. Anteroposterior and lateral radiographs of the left ankle showing a highly comminuted distal tibial (pilon) fracture associated with a diaphyseal fracture of the fibula. The articular surface is severely disrupted with significant metaphyseal bone fragmentation, consistent with a high-energy mechanism of injury following a fall from height. These findings mark the starting point of a complex course requiring multiple surgical interventions.
Four weeks later, a second surgical procedure was performed to remove the external fixator, achieve internal reduction of the fractures, and perform osteosynthesis with an anteromedial tibial plate. In addition, a Kirschner wire was inserted in the fibular malleolus.
Six weeks postoperatively, due to a lack of consolidation, a hexapod external fixator was applied to the tibia. Three months afterward, given a soft-tissue defect and delayed bone healing, another surgery was performed: removal of the hexapod fixator, placement of an autologous iliac crest bone graft, and soft-tissue coverage using an anterolateral thigh (ALT) free flap.
Due to persistent non-union 11 months later, the patient was referred to the orthoplastic surgery unit of our institution.
Upon admission, the patient was afebrile. An ALT flap was present on the anterior aspect of the left ankle, and the foot appeared edematous and in an equinus position (Fig. 2). The posterior tibial pulse was palpable.

Figure 2: Clinical appearance of the leg upon arrival at our hospital. Photographs of the patient’s left lower limb on admission, 11 months after initial trauma, and several prior surgeries. The anterolateral thigh free flap covering the anterior ankle is clearly visible, with signs of chronic inflammation and soft-tissue distortion. The foot is in an equinus position, and the leg appears edematous, reflecting the long-standing soft tissue compromise and biomechanical imbalance.
At final follow-up, clinical examination confirmed complete correction of the equinus deformity, achieving a stable plantigrade foot after tibiocalcaneal arthrodesis. The patient was able to ambulate independently with full weight-bearing and without pain, allowing satisfactory functional performance in daily activities.
Laboratory tests showed a C-reactive protein level of 5.1 mg/L and fibrinogen of 556 mg/dL. Plain radiographs revealed a pseudoarthrosis of the distal tibia with a bone defect measuring approximately 5.5 cm. Computed tomography confirmed the presence of atrophic pseudoarthrosis (Fig. 3).

Figure 3: Plain radiograph (top) and computed tomography (CT) scan (bottom) images of the tibial pseudoarthrosis. Imaging studies confirm atrophic pseudoarthrosis of the distal tibia. Radiographs show loss of cortical continuity and absence of callus formation. The CT scans (coronal and sagittal views) highlight a segmental bone defect of approximately 5.5 cm with sclerotic bone ends and a narrowed medullary canal, typical of avascular, biologically inactive pseudoarthrosis. These findings guided the decision for a staged orthoplastic reconstruction.
Following complementary diagnostic studies, a diagnosis of atrophic pseudoarthrosis of the distal tibia was established. The case was evaluated jointly by orthopedic and trauma surgery, plastic surgery, and infectious diseases departments.
In the first surgical stage, the pseudoarthrosis site was debrided, intraoperative samples were collected for culture (to rule out infection), and a gentamicin-impregnated cement spacer was placed. All intraoperative cultures were negative, with no growth of either Gram-positive or Gram-negative organisms. The patient was discharged 10 days later with oral antibiotic therapy: Ciprofloxacin 750 mg twice daily and linezolid 600 mg twice daily for 6 weeks. All intraoperative cultures were negative.
Upon completion of antibiotic treatment, a second surgical procedure was performed: Tibiocalcaneal arthrodesis using an intramedullary nail, and reconstruction of the segmental tibial defect with a contralateral free fibular flap.
The post-operative course was favorable. Bone densitometry revealed low bone mineral density for age, prompting rheumatology consultation and initiation of calcium and Vitamin D supplementation at discharge. During outpatient follow-up, the patient reported no pain, and ankle mobility was functionally dependent on forefoot motion. The patient was able to ambulate independently without assistive devices, achieving satisfactory functional mobility for daily activities. Furthermore, he showed good evolution of the flap and progressive radiographic signs of bone healing (Fig. 4).

Figure 4: Radiographic follow-up at 3 months after tibiocalcaneal arthrodesis and contralateral free fibular flap reconstruction. Anteroposterior and lateral views demonstrate stable alignment and fixation with an intramedullary nail spanning from the tibial shaft into the calcaneus. The transferred fibular graft is visible within the tibial defect zone, showing early signs of integration. There are no signs of hardware loosening or infection, and the bone–graft interface exhibits early consolidation, indicating a favorable post-operative evolution.
Tibial pseudoarthrosis remains one of the most complex and challenging complications in orthopedic and trauma surgery. Its management requires a comprehensive understanding of the biological, mechanical, and systemic factors involved in bone healing, along with an individualized and often multidisciplinary therapeutic strategy [1,2]. The case presented involves atrophic pseudoarthrosis of the distal tibia following a comminuted pilon fracture, requiring multiple surgical interventions. Major risk factors contributing to the non-union in this patient included smoking, fracture complexity, compromised local vascularization, and multiple surgeries. Smoking, in particular, is associated with vasoconstriction, reduced oxygen supply, and impaired osteoblastic activity, which collectively hinder osteogenesis [1].
The distinction between hypertrophic (viable) and atrophic (non-viable) pseudoarthrosis is critical for treatment planning. In atrophic pseudoarthrosis, as in this case, the primary challenge is biological; thus, treatment must address both mechanical stability and the promotion of a biologically conducive environment for healing [1,2,4].
Hexapod external fixators offer significant advantages in managing such injuries, including precise three-dimensional corrections and progressive mechanical stimulation of osteogenesis. However, in the context of major bone defects and compromised soft-tissue coverage, complex reconstructive strategies become necessary [5].
In this case, a multidisciplinary approach was essential. Collaboration among orthopedic and trauma surgery, plastic surgery, and infectious diseases allowed comprehensive planning: Beginning with debridement and culture sampling, followed by reconstruction using a free osteomyocutaneous fibular flap from the contralateral leg. Such procedures are technically demanding and are best performed in centers with dedicated orthoplastic units. Ultimately, tibiocalcaneal arthrodesis with an intramedullary nail provided a stable and definitive solution in the setting of a non-functional ankle and multiple prior surgeries, also enabling early weight-bearing.
Free vascularized fibular flaps provide excellent functional outcomes in tibial pseudoarthrosis, with reported union rates ranging from 74% to 100% and a high proportion of patients achieving pain-free weight-bearing. When combined with ankle arthrodesis, particularly in cases with distal tibial bone loss and joint destruction, the flap offers reliable structural support and promotes fusion, enabling stable limb preservation. Although some degree of joint stiffness or reduced range of motion may persist, most patients regain functional independence and report high satisfaction due to successful limb salvage and durable arthrodesis [6,7,8,9,10].
This case underscores the value of an integrated and coordinated approach in managing complex pseudoarthroses, with objectives extending beyond bone union to include preservation of function and restoration of soft tissue integrity.
This case illustrates the complexity and therapeutic demands of atrophic tibial pseudoarthrosis, particularly when accompanied by significant bone loss and soft tissue compromise. Successful management depends on a staged, patient-specific strategy that incorporates infection control, mechanical stability, biological stimulation, and soft-tissue reconstruction.
This article highlights the clinical value of a multidisciplinary orthoplastic approach in successfully managing complex distal tibial atrophic pseudoarthrosis with severe bone and soft-tissue loss.
References
- 1. Fortuin F, Burger M, Ferreira N. Contemporary management of aseptic diaphyseal tibia non-unions – a systematic review. Orthop Traumatol Surg Res 2022;108:102990. [Google Scholar] [PubMed]
- 2. Piccolo PP, Ben-Amotz O, Ashley B, Wapner KL, Levin LS. Ankle arthrodesis with free vascularized fibula autograft using saphenous vein grafts: A case series. Plast Reconstr Surg 2018;142:806-9. [Google Scholar] [PubMed]
- 3. Wallace AB, Devitt SM, Kreitz TM, Raikin SM, Greaney PJ Jr. Free vascularized fibular graft for distal tibial and ankle arthrodesis. J Reconstr Microsurg Open 2016;1:111-6. [Google Scholar] [PubMed]
- 4. Pineda S, Hasan O, Shah M. Delayed union and nonunion following fractures of the tibia. J Am Acad Orthop Surg 2020;28:e92-101. [Google Scholar] [PubMed]
- 5. Fraga Lavía K, Bermejo Segú O, Ruzafa E, Barrantes S, Tramunt Monsonet C, Llop Corbacho A. First-ever ankle arthrodesis with the Capanna technique in an infected open fracture. JPRAS Open 2023;39:157-63. [Google Scholar] [PubMed]
- 6. Khan MI, Aslam N, Qureshi A, Baig MA, Azeem S. Functional outcomes of free vascularized fibular graft in tibial bone defects. J Pak Med Assoc 2022;72:1096-100. [Google Scholar] [PubMed]
- 7. Van Veen T, Hedengran A, Rahbek O, Damsgaard TE. Functional outcomes of vascularized fibula transfer for reconstruction of large tibial defects: A long-term follow-up. Microsurgery 2024;44:35-42. [Google Scholar] [PubMed]
- 8. Li X, Xu H, Liu Y, Zhang W, Chen J. Orthoplastic reconstruction of infected tibial nonunion using free vascularized fibular graft: Functional outcomes and complications. J Plast Reconstr Aesthet Surg 2024;77:652-60. [Google Scholar] [PubMed]
- 9. Roukis TS, Kang RB. Vascularized pedicled fibula onlay bone graft augmentation for complicated tibiotalocalcaneal arthrodesis with retrograde intramedullary nail fixation: A case series. J Foot Ankle Surg 2016;55:857-67. [Google Scholar] [PubMed]
- 10. Noorlander-Borgdorff MP, Alkemade E, Van Der Sluis WB, De Jong T, Driessen C, Giannakópoulos GF, et al. Long-term results and patient-reported outcomes after vascularized fibular graft use in the treatment of post-traumatic bone defects of femur shaft and tibia: A retrospective cohort and cross-sectional survey study. J Plast Reconstr Aesthet Surg 2024;98:144-57. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 10, 2022 Osteoid Osteoma of Talus – A Rare Occurrence Mimicking Ankle Arthritis: A Case Report
February 10, 2022 Osteoid Osteoma of Talus – A Rare Occurrence Mimicking Ankle Arthritis: A Case Report November 1, 2025 Functional Outcome of Arthroscopic Single-row Rotator Cuff Repair Using the PENN Shoulder Score – A Prospective Cohort Study
November 1, 2025 Functional Outcome of Arthroscopic Single-row Rotator Cuff Repair Using the PENN Shoulder Score – A Prospective Cohort Study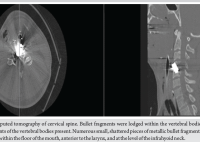 July 10, 2024 Migration of Bullet Fragment 11 Years after Initial Gunshot Wound leads to Cervical Prevertebral Abscess: A Case Report
July 10, 2024 Migration of Bullet Fragment 11 Years after Initial Gunshot Wound leads to Cervical Prevertebral Abscess: A Case Report April 20, 2015 Arthroscopy Assisted Percutaneous Fixation of Ideberg Type Iii Glenoid Fractures
April 20, 2015 Arthroscopy Assisted Percutaneous Fixation of Ideberg Type Iii Glenoid Fractures