
The combination of latissimus dorsi and teres major tendon transfer (LDTM) with middle trapezius tendon transfer (MTT) can improve shoulder function by providing dynamic stability in patient with anterior superior irreparable rotator cuff tear with anterior superior subluxation.
Dr. Chang Hee Baek, Department of Orthopaedic Surgery, Yeosu Baek Hospital, 50, Yeoseo 1-ro, Yeosu-si, Jeollanam-do, Republic of Korea. E-mail: yeosubaek@gmail.com
Introduction: Anterior superior irreparable rotator cuff tears (ASIRCTs) are a challenging clinical condition, especially in younger patients and those with high functional demands. Various surgical options, including tendon transfers, aim to restore shoulder stability and function in the absence of a viable rotator cuff.
Case Report: A 54-year-old male fisherman with a history of failed rotator cuff repair presented with persistent shoulder pain and significantly limited range of motion (ROM). Radiographic and magnetic resonance imaging findings confirmed ASIRCT with anterior superior subluxation of the humeral head. The patient underwent a combined latissimus dorsi and teres major transfer along with an arthroscopically assisted middle trapezius tendon transfer.
Conclusion: The patient demonstrated substantial functional improvement at 1 year, with increased ROM, strength, and patient-reported outcomes. Radiographic evaluation showed reduced humeral subluxation and stable transferred tendon integration. This dual tendon transfer approach offers a viable surgical option for restoring shoulder function in patients with severe ASIRCTs.
Keywords: Tendon transfer, irreparable rotator cuff tears, anterior superior irreparable rotator cuff tears, latissimus dorsi and teres major transfer, middle trapezius tendon transfer.
Anterior superior irreparable rotator cuff tears (ASIRCTs) represent a significant clinical challenge, particularly in younger patients with high functional demands and in active elderly individuals seeking to preserve joint mobility and function [1]. A variety of surgical treatment options have been described in the literature, including arthroscopic partial repair with or without patch augmentation, superior capsular reconstruction (SCR), isolated latissimus dorsi (LD) transfer with or without teres major (TM), balloon spacers, and reverse total shoulder arthroplasty (RTSA) [2]. However, outcomes associated with these techniques remain unpredictable and varied. The anterior LD and TM transfer has emerged as a promising surgical intervention for managing irreparable subscapularis tears [3]. This technique restores transverse force coupling by synergistically utilizing the biomechanical properties of the LD and TM muscles, resulting in improved dynamic stability of the shoulder joint [3,4]. In addition, the LDTM tendon transfer exerts a downward traction on the humeral head and establishes a robust line of pull, contributing to enhanced functional outcomes, including strength restoration and increased active range of motion (ROM) [4]. Nonetheless, pre-operative anterior superior escape has been shown to negatively impact post-operative outcomes, even after tendon transfer procedures [3]. For cases involving isolated irreparable supraspinatus tears, arthroscopically assisted middle trapezius tendon (MTT) transfer has demonstrated favorable outcomes [5]. This approach provides dynamic stabilization to the glenohumeral joint and serves as a mechanical spacer within the subacromial space, thereby mitigating superior translation of the humeral head and improving joint biomechanics [6]. These advancements underscore the potential of targeted tendon transfer procedures to address the unique challenges posed by ASIRCTs, offering a viable pathway for functional recovery in this patient population.
Case description
A 54-year-old right-handed male, employed as a heavy labor, presented to our clinic with persistent right shoulder pain and severely restricted ROM. The patient had undergone an initial rotator cuff repair 5 years prior, followed by a revision surgery 3 years ago due to a retear. At the time of presentation at our clinic, the patient experienced severe pain with visual analogue scale (VAS) of 7, and exhibited pseudoparalysis, characterized by forward elevation (FE) limited to 30°, abduction (ABD) to 30°, external rotation at the side (ERS) to 30°, and internal rotation (IR) to the buttock level. Functional assessment scores indicated significant functional impairment and dissatisfaction, with a constant score of 46/100, University of California-Los Angeles (UCLA) score of 17/35, and American Shoulder and Elbow Surgeons (ASES) score of 47/100. Radiographic evaluation revealed no signs of glenohumeral joint arthritis but demonstrated anterior humeral subluxation and superior translation of the humeral head (Fig. 1a and b) in magnetic resonance imaging (MRI), there was a recurrent tear of the revision rotator cuff repair, with the supraspinatus tendon medially retracted to the glenoid margin (Patte [7] stage 3) (Fig. 1c). In addition, there was an irreparable subscapularis tear classified as Lafosse et al. [8] stage 4, with severe atrophy and advanced fatty infiltration graded as Goutallier et al. [9] stage 4 (Fig. 1d). Given the patient’s active lifestyle and reluctance to pursue arthroplasty, a decision was made to perform a dual reconstruction. This involved anterior LDTM transfer along with an arthroscopically assisted MTT transfer to address the ASIRCT.

Figure 1: Preoperative imaging of the right shoulder. (a) Pre-operative radiograph shows no evidence of glenohumeral arthritis, but (b) anterior humeral subluxation is observed (white arrow). Pre-operative magnetic resonance imaging reveals (c) a retracted, retorn supraspinatus tendon (white asterisk) in the coronal plane, and (d) severe atrophy with significant fatty infiltration of the subscapularis muscle (red asterisk).
Surgical procedure
The surgery was performed under general anesthesia and comprised two distinct procedures: Arthroscopically assisted MTT transfer and anterior LDTM transfer. The patient was initially positioned in the lateral decubitus position for the MTT transfer, and upon its completion, repositioned to the beach chair position for the LDTM transfer. Both procedures adhered to standardized surgical protocols described in previously published literature [10,11] and were performed within the same anesthetic session.
Arthroscopically assisted MTT transfer
First, a fascia lata autograft, measuring 5 cm × 15 cm, was harvested from the ipsilateral thigh to serve as an interpositional graft that connects the middle trapezius muscle and humerus. The graft was folded to achieve the desired thickness, reinforced with acellular dermal matrix, and secured with #2 non-absorbable sutures (Fig. 2a). To harvest the middle trapezius, an incision was made above the scapular spine. After dissecting through the skin and subcutaneous tissue, the middle trapezius muscle was exposed. The tendon was detached along the scapular spine, with care taken to avoid the acromioclavicular joint. The lateral portion of the tendon was isolated from the underlying supraspinatus fascia and prepared using #2 non-absorbable sutures (Fig. 2b). The supraspinatus insertion site was prepared by debridement with a shaver and burr, and two triple-loaded suture anchors were placed at the medial edge of the footprint. Using arthroscopic guidance, the graft was passed through the supraspinatus outlet into the subacromial space and secured at the footprint using a double-row suture bridge technique with additional three knotless anchors (Fig. 2c). The distal end of the graft was attached to the middle trapezius muscle with the patient’s arm positioned in ABD (Fig. 2d).

Figure 2: Middle trapezius tendon transfer (a) Prepared interpositional graft using a fascia lata autograft (white arrow), augmented with acellular dermal matrix (red arrow). (b) Harvested the middle trapezius muscle (white asterisk). (c) Arthroscopic view showing the interpositional graft (red arrow) being fixed to the supraspinatus footprint. (d) Final appearance of the interpositional graft (red asterisk) securely fixed to the middle trapezius muscle.
Anterior LD and TM transfer
The standard deltopectoral approach was employed with the incision extending from the coracoid process to the inferior border of the pectoralis major (PM) tendon. Soft tissue tenodesis of the long head of the biceps tendon was performed. After careful dissection, the PM muscle was retracted to expose the LDTM tendon insertion at the humerus. The LDTM tendons were harvested as a single unit without separating the LD and TM components (Fig. 3a). The harvested tendon was augmented with acellular dermal matrix and prepared with non-absorbable sutures using a Krakow technique (Fig. 3b) Adhesions were carefully released to prevent radial nerve injury, and the tendon was passed beneath the PM muscle toward the greater tuberosity (GT). When transferring the LDTM tendon to the humerus, the arm was positioned in full internal rotation and 45° ABD. The tendon was fixed approximately 2 cm distal to the GT and lateral to the bicipital groove using a knotless anchor (Fig. 3c). For additional fixation, a triple-loaded suture anchor was placed beneath the tendon, and two knotless anchors were used to compress the tendon against the humerus with a double row suture bridge configuration. Finally, impingement-free rotation was confirmed.

Figure 3: Latissimus dorsi (LD) and teres major (TM) tendon transfer (a) Harvested LDTM tendon (white asterisk) grasped with two long forceps. (b) Augmented LDTM tendon using acellular dermal matrix (red asterisk). (c) Final appearance of the completed LDTM transfer (red asterisk).
Post-operative rehabilitation
During the first 4 weeks post-operatively, the patient’s arm was immobilized in a 45° ABD brace. Continuous passive motion exercise was performed during the first 4 weeks. After 4 weeks, the brace was discontinued, and the patient initiated active-assisted ROM exercises aimed at progressively restoring shoulder mobility. At 3 months post-operatively, strengthening exercises were introduced in all directions to enhance muscle function and joint stability. However, heavy manual labor and sports activities were strictly prohibited until 6 months post-operatively to ensure proper healing and tendon integration.
Post-operative outcome
At the 1-year post-operative follow-up, the patient expressed high satisfaction with the surgical outcomes. The patient’s pain improved to a VAS of 2, and functional assessment scores demonstrated significant improvement, with a Constant score of 77/100, a UCLA score of 31/35, and an ASES score of 87/100. The ROM also showed marked enhancement, with FE and ABD both increasing to 130°, ERS improving to 50°, and IR to back reaching the L3 vertebral level. Radiographic evaluation revealed no progression of glenohumeral joint arthritis, while pre-operative anterior humeral subluxation and superior translation of the humeral head were notably reduced (Fig. 4 a and b). Post-operative MRI at 1 year confirmed the intact integrity of both the LDTM transfer and the MTT transfer, with no signs of graft failure. No complications were reported during the post-operative period (Fig. 4c and d).

Figure 4: Post-operative imaging of the right shoulder. (a) Post-operative radiograph demonstrates no progression of glenohumeral arthritis, and (b) reduced anterior humeral subluxation (white arrow). Post-operative magnetic resonance imaging confirms an intact transferred tendon for (c) the middle trapezius transfer (red arrow) and (d) the latissimus dorsi and teres major transfer (white arrow).
ASIRCTs represent a particularly challenging clinical entity, especially in younger patients who seek to preserve shoulder function for their active lifestyles, as well as in older individuals with intact cartilage who wish to maintain highly demand activity without resorting to more invasive procedures, such as RTSA [2]. These tears, especially when involving the subscapularis, can lead to significant functional impairment and the damage to the rotator cuff musculature often leads to an unbalanced shoulder, resulting in altered biomechanics that place stress on the glenohumeral joint [12]. This imbalance can lead to pain, weakness, loss of motion, and, in some cases, progressive joint instability [13]. RTSA is often considered a last-resort solution for cases with severe functional deficits, but it is not always the best option, particularly for active individuals who wish to avoid a prosthetic joint replacement [14]. Furthermore, RTSA may be associated with concerns regarding the longevity of the implant, mechanical failure, and the potential for complications, such as infection, instability, or loosening [14,15]. Moreover, RTSA is typically not considered ideal in the absence of glenohumeral arthritis, as it may not fully restore functional strength, particularly for younger patients who may experience early implant failure [15]. Numerous alternative surgical approaches have been investigated to address the unique challenges of ASIRCTs. These techniques aim to restore dynamic stability and function by either augmenting or substituting for the deficient musculature. Approaches, such as arthroscopic partial repair (with or without augmentation), margin convergence, muscle advancement, and SCR have been widely employed [2]. Although these techniques can yield satisfactory results in some cases, they often fall short in providing long-term stability, especially in cases with significant muscle atrophy and fatty infiltration [16,17]. Partial repairs and SCR may restore static stability, but they fail to replace the dynamic role of the rotator cuff in shoulder motion, limiting improvements in strength and overall function [16,17,18]. Tendon transfer surgeries represent an effective solution for managing irreparable rotator cuff tears, especially in cases where the remaining rotator cuff tissue is in poor condition [19]. Tendon transfer techniques offer dynamic biomechanical support and can help to restore shoulder function by rebalancing the forces acting across the glenohumeral joint [19]. In cases where the subscapularis tendon is irreparably damaged, tendon transfers provide a means of restoring the necessary stabilization to the anterior and superior aspects of the shoulder joint. One promising approach for managing these complex cases is the anterior LDTM transfer. The synergy between the LD and TM tendons allows for effective joint stabilization by replicating the action of the subscapularis tendon, particularly in terms of depressing the humeral head and restoring internal rotation strength [4]. Biomechanical studies have shown that the LD and TM muscles work together to provide a stable and functional alternative to the damaged subscapularis [4]. The LD tendon, with its large muscle mass and line of pull, helps stabilize the humeral head, while the TM tendon contributes to the humeral head depression, enhancing the effectiveness of the transfer [20]. The success of the LDTM transfer for ASIRCTs is further supported by cadaveric studies, which have demonstrated that this combined tendon transfer significantly reduces both superior and anteroinferior translations of the humeral head [4,20]. These studies have also shown that the LDTM transfer is superior in reducing subacromial contact pressures compared to isolated LD tendon transfers, making it an attractive option for patients with substantial rotator cuff deficiency and glenohumeral instability. The MTT transfer has biomechanical properties that are similar to the supraspinatus muscle, which plays a crucial role in stabilizing the glenohumeral joint [6]. MTT transfer aims to provide dynamic stabilization to the joint while also preventing superior migration of the humeral head, a common complication in patients with rotator cuff deficiencies [6]. The use of an interpositional graft, such as fascia lata, further enhances the efficacy of MTT transfer by acting as a spacer within the subacromial space [10]. This spacer effect prevents superior migration of the humeral head and contributes to better joint mechanics. This approach addresses both the structural and functional deficits seen in patients with ASIRCTs by improving the biomechanics of the shoulder joint and stabilizing the humeral head. Studies on MTT transfer have demonstrated favorable clinical outcomes, particularly in cases with irreparable supraspinatus tears [10,21]. These studies have shown that MTT transfer can restore humeral head stability, reduce subacromial contact pressure, and improve both active ROM and strength [5,21]. Furthermore, MTT transfer has been shown to maintain its efficacy over an extended follow-up period, providing sustained improvements in both patient-reported outcomes and clinical scores [5]. In our case, the combination of LDTM and MTT tendon transfers yielded significant improvements in both functional outcomes and joint stability. The synergy between these two tendon transfer procedures allowed for the restoration of a dynamic force couple, which is essential for maintaining proper humeral head positioning during shoulder motion. By addressing both the anterior and superior deficiencies (via the LDTM and MTT transfers, respectively), the dual reconstruction improved shoulder biomechanics, alleviated pain, and enhanced strength and ROM. At 1 year post-operatively, the patient demonstrated significant improvements in functional scores, including the constant, UCLA, and ASES scores. The ROM in FE, ABD, ERS, and IR to back showed marked enhancement. Furthermore, radiographic imaging revealed no progression of glenohumeral arthritis, and the previously noted anterior humeral subluxation and superior translation were significantly reduced. The combined LDTM and MTT tendon transfers, by restoring dynamic stability, may also delay or prevent the need for more invasive procedures, such as RTSA, particularly in young patients who wish to preserve their native shoulder joint. Several limitations should be considered. First, the extended operative time required for dual tendon transfer surgeries increases the risk of complications, such as infection, blood loss, and anesthesia-related issues. The complexity of the procedure demands a high level of technical skill, and surgeons must be proficient in both arthroscopic techniques and open tendon transfers. In addition, harvesting the fascia lata autograft for the MTT transfer introduces another layer of complexity, with potential donor site morbidity. Given that this study is based on a single patient, further research is needed with more patients to assess the long-term outcomes of dual tendon transfers for ASIRCTs. Larger cohort studies and randomized controlled trials comparing dual tendon transfer with other surgical options, such as RTSA or SCR, will be crucial in determining the most effective management strategies for ASIRCTs.
The dual tendon transfer approach, combining LDTM transfer and MTT transfer, provides an effective solution for managing ASIRCTs. This technique restores shoulder stability, improves ROM, and reduces pre-operative anterior superior humeral subluxation. In the case presented, the patient showed significant functional improvement at 1-year follow-up, offering a promising alternative to more invasive procedures, such as RTSA, especially for active individuals with ASIRCTs but without arthritis.
Combined tendon transfers, including LDTM transfer with MTT transfer, offer a promising solution for restoring shoulder stability and function in patients with ASIRCTs. This technique can significantly improve outcomes and delay or avoid the need for more invasive procedures, such as RTSA in active individuals without arthritis.
References
- 1. Dang A, Davies M. Rotator cuff disease: Treatment options and considerations. Sports Med Arthrosc Rev 2018;26:129-33. [Google Scholar] [PubMed]
- 2. Oh JH, Park MS, Rhee SM. Treatment strategy for irreparable rotator cuff tears. Clin Orthop Surg 2018;10:119-34. [Google Scholar] [PubMed]
- 3. Baek CH, Kim JG, Baek GR. Outcomes of combined anterior latissimus dorsi and teres major tendon transfer for irreparable anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2022;31:2298-307. [Google Scholar] [PubMed]
- 4. Baek GR, Kim JG, Nakla AP, Kwak D, Chung MS, McGarry MH, et al. Latissimus dorsi and teres major tendon transfer for irreparable anterosuperior rotator cuff tear improves kinematics and internal rotation compared to latissimus dorsi tendon transfer. Arch Orthop Trauma Surg 2023;143:4731-9. [Google Scholar] [PubMed]
- 5. Baek CH, Kim JG. Outcomes of arthroscopic-assisted middle trapezius tendon transfer for isolated irreparable supraspinatus tendon tears: Minimum 2-year follow-up. Arch Orthop Trauma Surg 2023;143:2547-56. [Google Scholar] [PubMed]
- 6. Moroder P, Akgün D, Lacheta L, Thiele K, Minkus M, Maziak N, et al. Middle trapezius transfer for treatment of irreparable supraspinatus tendon tears- anatomical feasibility study. J Exp Orthop 2021;8:5. [Google Scholar] [PubMed]
- 7. Patte D. Classification of rotator cuff lesions. Clin Orthop Relat Res 1990;254:81-6. [Google Scholar] [PubMed]
- 8. Lafosse L, Jost B, Reiland Y, Audebert S, Toussaint B, Gobezie R. Structural integrity and clinical outcomes after arthroscopic repair of isolated subscapularis tears. J Bone Joint Surg Am 2007;89:1184-93. [Google Scholar] [PubMed]
- 9. Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res 1994;304:78-83. [Google Scholar] [PubMed]
- 10. Baek CH, Kim BT, Kim JG. Arthroscopic-assisted middle trapezius transfer using an achilles tendon allograft in treatment of isolated supraspinatus irreparable rotator cuff tears in lateral decubitus position. Arthrosc Tech 2024;13:102976. [Google Scholar] [PubMed]
- 11. Baek CH, Kim BT, Kim JG. Combined anterior latissimus dorsi and teres major tendon transfer (aldtm) for irreparable anterosuperior rotator cuff tears. JBJS Essent Surg Tech 2024;14:e23.00060. [Google Scholar] [PubMed]
- 12. De Rus Aznar I, Ávila Lafuente JL, Hachem AI, Díaz Heredia J, Kany J, Elhassan B, et al. Tendon transfers for the management of irreparable subscapularis tears. Bone Joint J 2024;106-B:970-7. [Google Scholar] [PubMed]
- 13. Shepet KH, Liechti DJ, Kuhn JE. Nonoperative treatment of chronic, massive irreparable rotator cuff tears: A systematic review with synthesis of a standardized rehabilitation protocol. J Shoulder Elbow Surg 2021;30:1431-44. [Google Scholar] [PubMed]
- 14. Burden EG, Batten TJ, Smith CD, Evans JP. Reverse total shoulder arthroplasty. Bone Joint J 2021;103-B:813-21. [Google Scholar] [PubMed]
- 15. Kennedy J, Klifto CS, Ledbetter L, Bullock GS. Reverse total shoulder arthroplasty clinical and patient-reported outcomes and complications stratified by preoperative diagnosis: A systematic review. J Shoulder Elbow Surg 2021;30:929-41. [Google Scholar] [PubMed]
- 16. Katthagen JC, Bucci G, Moatshe G, Tahal DS, Millett PJ. Improved outcomes with arthroscopic repair of partial-thickness rotator cuff tears: A systematic review. Knee Surg Sports Traumatol Arthrosc 2018;26:113-24. [Google Scholar] [PubMed]
- 17. Werthel JD, Vigan M, Schoch B, Lädermann A, Nourissat G, Conso C, et al. Superior capsular reconstruction – a systematic review and meta-analysis. Orthop Traumatol Surg Res. 2021;107:103072. [Google Scholar] [PubMed]
- 18. Baek CH, Kim BT, Kim JG, Kim SJ. Mid-Term outcome of superior capsular reconstruction using fascia lata autograft (at least 6 mm in thickness) results in high retear rate and no improvement in muscle strength. Arthroscopy 2024;40:1961-71. [Google Scholar] [PubMed]
- 19. Li X, Galvin JW, Zalneraitis BH, Gasbarro G, Parada SA, Eichinger JK, et al. Muscle tendon transfers around the shoulder: Diagnosis, treatment, surgical techniques, and outcomes. J Bone Joint Surg Am 2022;104:833-50. [Google Scholar] [PubMed]
- 20. Elhassan B, Christensen TJ, Wagner ER. Feasibility of latissimus and teres major transfer to reconstruct irreparable subscapularis tendon tear: An anatomic study. J Shoulder Elbow Surg 2014;23:492-9. [Google Scholar] [PubMed]
- 21. Kandeel AA. Middle trapezius tendon transfer for augmentation of in situ superior capsular reconstruction-reinforced partial rotator cuff repair: Short-term outcomes of a prospective cohort study. Orthop J Sports Med 2023;11:23259671221147537. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Flexor Tendon Injuries in Zone 3: A Comprehensive Review and Case Report on Flexor Digitorum Profundus Rupture of the Middle Finger
December 1, 2025 Flexor Tendon Injuries in Zone 3: A Comprehensive Review and Case Report on Flexor Digitorum Profundus Rupture of the Middle Finger November 1, 2025 Combined Anterior Latissimus Dorsi and Teres Major Tendon Transfer for Anterosuperior Irreparable Rotator Cuff Tears in One-Arm Patients: A Case Report
November 1, 2025 Combined Anterior Latissimus Dorsi and Teres Major Tendon Transfer for Anterosuperior Irreparable Rotator Cuff Tears in One-Arm Patients: A Case Report February 1, 2025 Medial Epicondyle Fracture Dislocation, Multiple Failed Reductions, and a Median Nerve Entrapment: A Case Report
February 1, 2025 Medial Epicondyle Fracture Dislocation, Multiple Failed Reductions, and a Median Nerve Entrapment: A Case Report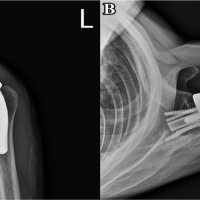 June 10, 2024 Pectoralis Major Transfer For Anterior Recurrent Dislocation of Reverse Total Shoulder Arthroplasty: A Case Report
June 10, 2024 Pectoralis Major Transfer For Anterior Recurrent Dislocation of Reverse Total Shoulder Arthroplasty: A Case Report