
Deep-seated lipomas occurring in the muscle and periosteum are rare and exhibit heterogeneous fat signals on magnetic resonance imaging unlike classical lipomas. They closely mimic atypical lipomatous tumors or well-differentiated liposarcoma and need to be meticulously examined on MRI, histopathological and by immunohistochemistry for MDM2 and CDK4 expression.
Dr. Narendran Pushpasekaran, 2/231-5, Ponnandi Gounder Street, Alaghapuram Periyapudur, Salem - 636016, Tamil Nadu, India. E-mail: drnaren247ortho@gmail.com
Introduction: Lipomas arising from the muscle and bone are uncommon and remain unnoticed till giant size. Major concern is to differentiate from atypical lipomatous tumors (ALTs) which have propensity to recur or differentiate to liposarcomas. Through this case report, we review the intramuscular lipomas involving muscles of shoulder girdle and the current concepts in imaging and histopathological examination to differentiate deeply seated lipomas from ALTs.
Case Report: A 47-year-old female was evaluated for a painless swelling that gradually increased in size in the right shoulder and upper arm for 8 months. Magnetic resonance imaging (MRI) showed lipomatous lesions in the biceps tendon of size 7 × 5 cm but expressed heterogeneous fat signals on suppression sequence. The biopsy revealed mature adipocytes with occasional fibrous septa that contained mixed inflammatory cells. Due to equivocal findings with ALT, immunohistochemical staining for murine double minute 2 (MDM2) homolog expression was performed but negative. There was no recurrence of the lesion and patient had no functional impairment.
Conclusion: Intramuscular lipomas that grow to giant size can exhibit heterogeneous fat signals in MRI and need to be looked for ALTs or well-differentiated liposarcoma through histopathological examination. Staining for MDM2 homolog and cyclin-dependent kinase-4 expression that are typical for ALTs is necessary when histopathological findings are indeterminate.
Keywords: Intramuscular lipoma, Atypical lipomatous tumors, Immune-histopathological staining, Murine double minute-2, cyclin-dependent-kinase-4.
Lipomas located deep to the subcutaneous fascia in the muscles and bone are rare and constitute <1% of its occurrence. These deep-seated lipomas are usually distributed in thigh, trunk or neck and tend to grow large in size (>5 cm) before any cosmetic discomfort, functional impairment, or neurovascular compression [1,2,3]. Again, giant lipomas in deeper locations closely mimic atypical lipomatous tumors (ALTs) or well-differentiated liposarcoma and must be evaluated through radiological, histopathological, and immune-histochemical staining due to its propensity for liposarcomas [4]. Through this case, we report a rare occurrence of intramuscular lipoma in the shoulder girdle and review the current concepts in evaluating the deep-seated lipomas for ALTs.
A 67-year-old female with complaints of painless swelling that progressively increased in size in the right shoulder and proximal arm for the past 8 months examination showed a palpable mass of size 8 × 5 cm non-tender with smooth surface and in the deeper planes of the shoulder girdle, mobile with firm consistency. All the shoulder movements were preserved. Plain radiographs of the right shoulder and arm were normal. Ultrasonogram showed an echogenic lesion with fluid collection in the biceps muscle plane and anterior aspect of the upper third of right arm. Magnetic resonance imaging (MRI) of the right shoulder and arm showed a well-defined space-occupying lesion of size 25 × 33 × 60 mm in the long head of biceps muscle with incomplete rupture of long head of biceps tendon at the level of supra glenoid tubercle (Fig. 1).
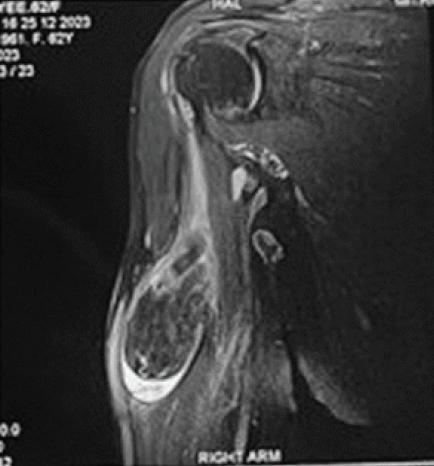
Figure 1: Magnetic resonance imaging of the right shoulder coronal section showing a space occupying lesion in long head of biceps. Proton density fat saturation image showing a well-defined ovoid hypointense lesion of size 6.4 cm × 3.2 cm with mild fluid seen around the mass likely of lipoma.
The lesion showed iso-intensity with fat in T1-weighted images and suppression with heterogeneous signals on T2-weighted images (Fig. 2).
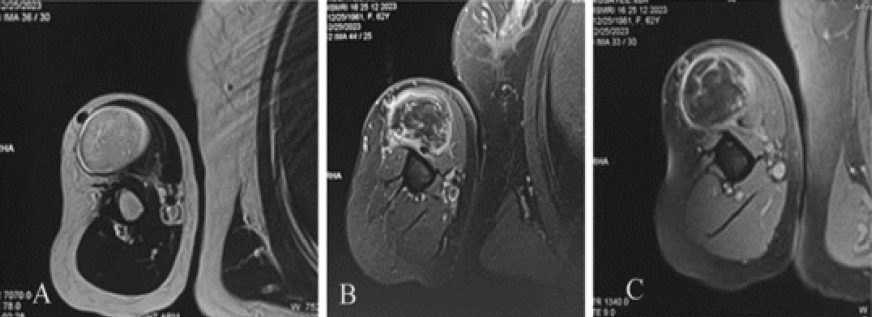
Figure 2: Axial sections of magnetic resonance imaging of the right shoulder. T2-weighted axial sequence showing a well-defined space occupying lesion isointense with subcutaneous fat and thin hypointense streaks suggestive of lipomatous lesion and minimal fibrous septae. (a) T1 fat suppression post-contrast axial sequence showing hypointense lesion in long head of biceps tendon with heterogeneous enhancement and fibrous septa enhancement along with a smooth peripheral capsule enhancement (b and c). Fine-needle aspiration cytology of the swelling showed fat globules with inflammatory cells; hence, an excision biopsy was planned. Under general anesthesia and interscalene block with patient in beach chair position, a deltopectoral approach was performed and the mass was found within the long head of biceps tendon without any infiltration to adjacent structures. Diagnostic shoulder arthroscopy was performed and the rupture was found at the proximal attachment of the long head of biceps tendon and tenotomy was completed. The biceps tendon was excised distally at the level of conjoint tendon. The excised mass with tendon was of size 6.5 × 4.5 centimeters and firm in consistency. The cut surface appeared yellow tan with densely packed contents with septations. Histopathological examination showed mature adipocytes with mixed inflammatory cells in the septa exhibiting a granulomatous septal panniculitis like picture and negative for murine double minute 2 (MDM2) expression (Fig. 3).
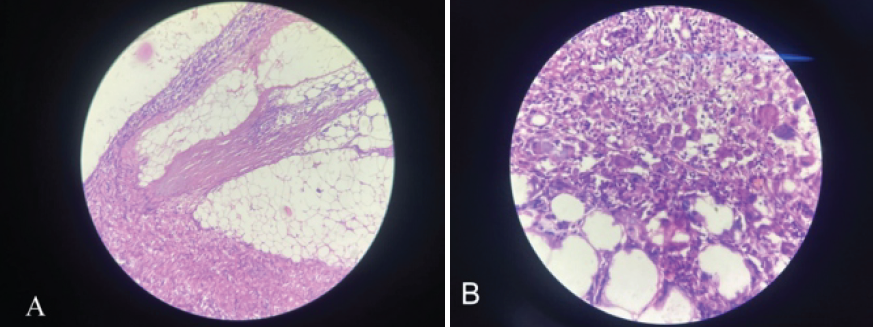
Figure 3: Histopathological examination of the excised mass from long head of biceps. Low power view showing mature adipocytes and few fibrous septae containing mixed inflammatory cells and lymphoid aggregates. Fibrinoid necrosis was observed and no abnormal micro vascularity around the sepate (hematoxylin and eosin stain, 10× magnification). (a) High-power view showed multinucleate giant cells in the fibrous septae. No spindle cells or lipoblasts were seen (b).
The post-operative event was uneventful and the patient had full range of motion movements of the shoulder and elbow with sufficient elbow flexion strength as with the opposite limb. She had no recurrence of the swelling over the follow-up period of 2 years.
Intramuscular lipomas are uncommon and these deep-seated lipomas constitute <1% of total occurrence of lipomas. Intermuscular or infiltrating lipoma and lipomas arising from bone or parosteal lipomas have also been reported [1]. Typically distributed in the muscles of trunk, neck, thigh and rarely the shoulder girdle of which lipomas of supraspinatus, infraspinatus, subscapularis, triceps, and biceps muscles have been reported in literature [3,5,6]. Located beneath the subcutaneous fascia, they are asymptomatic and tend to grow large in size before causing any dysfunction or Cosmetic notice [2]. Hence, MRI is the preferred modality of choice to investigate these lesions. The characteristic attenuation of intralesional signal intensity in fat suppression sequences favors the diagnosis of lipoma; however, various studies recommend sequences with contrast to study lesions larger than 5 cm in size or giant lipomas to observe the morphology (infiltrative/well defined) and features of liposarcoma (early filling of contrast) [7]. Lahrach et al. reported a lipoma of size 7 cm in the biceps brachi in a 50-year-old female on MRI which showed homogeneous signals within the lesion and capsulated [6]. Similarly in our case, a diagnosis was obtained on MRI only with the characteristic attenuation features of lipoma of giant size in the muscle belly of biceps and extending into the long head of biceps tendon but fat suppression images did not show homogeneity and the lesion exhibited heterogeneous enhancement on contrast admission. Differentiating lipomas from ALT on MRI sequences has been researched in recent literature [7,8,9]. Moran et al. analyzed 79 lipomatous lesions and observed that lesions of size 8 cm or less with homogeneous fat signals and without any septae or non-fat nodules are likely to be lipomas and all such lesions were MDM2 negative on immune histochemistry. However, larger sized lesions with heterogeneous fat signals, presence of sepate >2 mm, and non-fat nodules within lesions were likely to be atypical lipomatous lesions and showed positivity for MDM2 gene expression on biopsy immunohistochemistry [9]. Although in our case, heterogeneous fat signals with mild septations were observed, there were no nodules and the excised specimen did not show MDM2 expression, thereby confirming a lipoma. The parameters looked in the biopsy and histopathological examination to differentiate lipomatous lesions are the adipocyte morphology and nuclei, presence of septa that contain spindle cells and lipoblasts and the microvascularity in and around the septa [10]. Lipoblasts occur in all forms of lipomatous tumors and alone does not contribute to differentiating the lesions as the adipocyte morphology and nucleoli appear similar in lipoma, the key to identify the septa of >2 mm thickness and its spindle cell arrangement form the key to identify ALTs [11]. However, some set of lipomatous lesions have inadequate septae formation making differentiation a major concern and need for cytogenetic analysis [12]. At present, gene expression for MDM2, cyclin-dependent kinase 4 (CDK4), p16, cluster differentiation (CD) 31, and CD 36 through fluorescence or cytochrome in situ hybridization have been evaluated for differentiating lipoma, ALTs, and liposarcomas [12,13]. Deacu et al. evaluated 112 lipomatous lesions with immunohistochemical staining for gene expressions and observed that MDM2 and CDK4 were expressed in ALTs in more than 50% samples. Tumor microvascularization and CD34 were consistent for liposarcomatous and associated lesions. Adding to histopathological features, immunohistochemical staining improved the differentiate rate for lipomas, ALTs, and liposarcomas by 100%, 93.8%, and 100%, respectively [13]. In our case, the pathological examination showed the presence of fibrous septa that contain more of mixed inflammatory cells and scattered vessels featuring a septal panniculitis such as inflammation and not ALTs. We believe that instability of long head of biceps tendon secondary to tear caused tenosynovitis and that the pre-existing intratendinous lesion of adipocytes with fibrous septa featured a septal panniculitis such as inflammation on histopathological examination.
Intramuscular lipoma of muscle of the shoulder girdle is rare with the biceps reported more frequently. As with deep-seated lipomas, they grow to giant size and mimic ALTs. Lesions expressing heterogeneous fat signals and septations on MRI should be evaluated on histopathological examination for ALT and immunohistochemical staining for MDM2 and CDK4 expression increases the chances of differentiating the lipomatous lesions.
Intramuscular lipomas are usually diagnosed on MRI and when the exhibit uncharacteristic intralesional findings such as heterogeneity or sepate, excision biopsy, and immunohistochemical staining for ALTs must be performed which have a propensity for recurrence and liposarcoma.
References
- 1. McTighe S, Chernev I. Intramuscular lipoma: A review of the literature. Orthop Rev (Pavia) 2014;6:5618. [Google Scholar] [PubMed]
- 2. Hasan SS, O’Loughlin JP, Sorger JI. A large intermuscular shoulder lipoma causing pain and weakness in an 87-year-old patient: A case report. JSES Int 2020;5:154-7. [Google Scholar] [PubMed]
- 3. Elbardouni A, Kharmaz M, Salah Berrada M, Mahfoud M, Elyaacoubi M. Well-circumscribed deep-seated lipomas of the upper extremity. A report of 13 cases. Orthop Traumatol Surg Res 2011;97:152-8. [Google Scholar] [PubMed]
- 4. Johnson CN, Ha AS, Chen E, Davidson D. Lipomatous soft-tissue tumors. J Am Acad Orthop Surg 2018;26:779-88. [Google Scholar] [PubMed]
- 5. Park HW, Jo H, Moon SH, Baek S. Painful intramuscular lipoma of the infraspinatus: Unusual location and presentation. Orthopedics 2016;39:e370-3. [Google Scholar] [PubMed]
- 6. Lahrach K, El Kadi KI, Mezzani A, Marzouki A, Boutayeb F. An unusual case of an intramuscular lipoma of the biceps brachii. Pan Afr Med J 2013;15:40. [Google Scholar] [PubMed]
- 7. Chernev I, Petit-Clair N. Magnetic resonance imaging characteristics of intramuscular lipomas. Sao Paulo Med J 2015;133:64-6. [Google Scholar] [PubMed]
- 8. Brisson M, Kashima T, Delaney D, Tirabosco R, Clarke A, Cro S, et al. MRI characteristics of lipoma and atypical lipomatous tumor/well-differentiated liposarcoma: Retrospective comparison with histology and MDM2 gene amplification. Skeletal Radiol 2013;42:635-47. [Google Scholar] [PubMed]
- 9. Moran LM, Li Cai CY, Ramirez A, Royuela A. Differentiation of atypical lipomatous tumors from lipomas: Our experience with visual analysis of conventional magnetic resonance imaging. J Imaging 2025;11:47. [Google Scholar] [PubMed]
- 10. Nagano S, Yokouchi M, Setoguchi T, Ishidou Y, Sasaki H, Shimada H, et al. Differentiation of lipoma and atypical lipomatous tumor by a scoring system: Implication of increased vascularity on pathogenesis of liposarcoma. BMC Musculoskelet Disord 2015;16:36. [Google Scholar] [PubMed]
- 11. Asano Y, Miwa S, Yamamoto N, Hayashi K, Takeuchi A, Igarashi K, et al. A scoring system combining clinical, radiological, and histopathological examinations for differential diagnosis between lipoma and atypical lipomatous tumor/well-differentiated liposarcoma. Sci Rep 2022;12:237. [Google Scholar] [PubMed]
- 12. Weschenfelder W, Koeglmeier KL, Weschenfelder F, Spiegel C, Malouhi A, Gassler N, et al. Atypical lipomatous tumours vs. Lipomas: A multimodal diagnostic approach. Diagnostics (Basel) 2025;15:1538. [Google Scholar] [PubMed]
- 13. Deacu M, Bosoteanu M, Enciu M, Cozaru GC, Cojocaru O, Baltatescu GI, et al. The predictive role of the histopathological scoring system in adipose tumors-lipoma, atypical lipomatous tumor, and liposarcoma. Diagnostics (Basel) 2023;13:3606. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2022 Fourth-Generation Ceramic Head Fracture in Dual Mobility Total Hip Arthroplasty: A Case Report
January 10, 2022 Fourth-Generation Ceramic Head Fracture in Dual Mobility Total Hip Arthroplasty: A Case Report May 10, 2022 Return to Football after a Cervical Disk Arthroplasty: A Case Report
May 10, 2022 Return to Football after a Cervical Disk Arthroplasty: A Case Report August 6, 2024 A Case Series of Selective Nerve Root Block – A Technique for Delaying Surgery in Patients with Lumbar Radiculopathy
August 6, 2024 A Case Series of Selective Nerve Root Block – A Technique for Delaying Surgery in Patients with Lumbar Radiculopathy November 10, 2019 Surgical Treatment of a Chronic Morel-Lavallée Lesion: A Case Report
November 10, 2019 Surgical Treatment of a Chronic Morel-Lavallée Lesion: A Case Report