
Schwannoma, a nerve sheath tumor, having inflammatory micro environment, can produce symptoms mimicking prolapsed intervertebral disc, on stopping anti-inflammatory medications. The coexistence of nerve sheath tumor and prolapsed disc at same level will make confusion in the management.
Dr. G M Shafeeq, Spine Surgery Unit, Max Hospital, Nagpur, Maharashtra, India. E-mail: drgmshafeeq@gmail.com
Introduction: Lumbar intervertebral disc herniation commonly causes back pain and radiculopathy, but its coexistence with paravertebral tumors is rare. Nerve sheath tumors are the most frequent, yet their simultaneous occurrence with disc herniation producing similar symptoms is uncommon. Such cases are diagnostically and therapeutically challenging, as overlapping features may obscure the pathology and delay treatment.
Case Report: This is a rare case of a 33-year-old male presenting with low back pain and bilateral radiculopathy, left greater than right, for 1 month with positive straight leg raising test. Magnetic resonance imaging revealed an L5–S1 central disc herniation with an additional left paravertebral soft-tissue mass. Due to persistence and worsening of symptoms, even after conservative trail, he underwent endoscopic discectomy, and he had good relief of radicular pain. Postoperatively, after discontinuation of non-steroidal anti-inflammatory drugs, he developed left loin pain radiating to the thigh with tenderness at left loin. Excision biopsy of the mass confirmed a schwannoma. Following surgery, his symptoms improved markedly.
Conclusion: Sciatica may arise from lumbar disc herniation or from nerve sheath tumors, including intramuscular schwannomas. Schwannomas comprise multiple cellular elements – such as Schwann cells, axons, and macrophages – that create a complex “tumor microenvironment.” The dynamic interactions within this microenvironment play a key role in the development of symptoms. Anti-inflammatory agents can transiently suppress these processes; however, symptom recurrence, including back pain and radiculopathy, is often observed after their discontinuation.
Keywords: Schwannoma, tumor microenvironment, anti-inflammatory medication.
Lumbar disc herniation is one of the most frequent causes of radiculopathy and low back pain in adults. In contrast, spinal schwannomas are benign peripheral nerve sheath tumors, accounting for approximately 25–30% of all spinal tumors [1]. The simultaneous occurrence of lumbar disc herniation and schwannoma is extremely rare but clinically important because both can present with overlapping symptoms such as back pain and radiculopathy [2]. The tumor microenvironment (TME) of schwannomas is now recognized to contain inflammatory and immune cells that can influence tumor behavior and symptomatology [3]. Inflammatory mediators within the TME can exacerbate nerve irritation and mimic symptoms of disc herniation [4]. This case illustrates a unique clinical interaction between an L5–S1 disc herniation and a paraspinal schwannoma, where inflammatory changes around the tumor contributed to recurrent radiculopathy after discontinuation of anti-inflammatory therapy.
A 33-year-old male presented with low back pain and bilateral radiculopathy, left more than right, for 1 month. There was numbness over the left lower limb for 15 days, with no history of trauma. On examination, there was paraspinal muscle tenderness at the lumbar region. Straight leg raising test (SLRT) was 30° on the left and 60°on the right. There were no sensory or motor deficits. X-ray of the lumbosacral spine was normal. Magnetic resonance imaging (MRI) revealed an L5–S1 central disc bulge with a left paraspinal soft-tissue mass (Fig. 1). The patient was treated conservatively for 10 days with physiotherapy and medications (including non-steroidal anti-inflammatory drugs [NSAIDs]), but pain persisted and radicular symptoms worsened.

Figure 1: Pre-operative magnetic resonance imaging (T2): Showing (a) central disc bulge compressing the canal and nerve roots. (b) Soft-tissue mass.
Endoscopic decompression of the prolapsed disc was performed, addressing only the disc bulge. The mass was not disturbed as it was non-tender and asymptomatic, lying away from the operative field. The patient had marked pain relief in the immediate post-operative period.
However, after discontinuation of NSAIDs, he developed progressive left loin pain radiating to the left thigh, with localized tenderness at the left paraspinal region. SLRT again became painful on the left side, though neurological examination remained normal. A repeat MRI showed no recurrent disc herniation but revealed inflammatory changes surrounding the previously noted paraspinal mass (Fig. 2).

Figure 2: Magnetic resonance imaging (T2) (post-discectomy): Showing (a) Area of discectomy with decompressed canal. (b) Soft-tissue tumor.
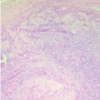
Surgical excision of the mass was done. Intraoperatively, inflammatory adhesions were noted around the lesion. Histopathological examination confirmed a benign schwannoma. Post-excision, the patient had complete and sustained pain relief. Biopsy revealed capsulated nodules of spindle cell neoplasm showing cellular and hypocellular areas with foci of Verocay bodies. The cells have spindle nuclei and mitosis is not seen (Fig. 3). The small nodule showed lymph node with reactive lymphoid hyperplasia.

Figure 3: Histopathology showing, ANTONY a area, containing spindle cells with elongated nuclei, in palisading pattern.
The coexistence of lumbar disc herniation and schwannoma is exceedingly rare, with only isolated case reports documented in literature [2,5]. Their clinical overlap may delay diagnosis since both can present with back pain, radiculopathy, and tenderness [6]. In this case, initial symptoms were primarily due to the L5–S1 central disc herniation, and the incidental paraspinal mass (later proven to be a schwannoma) was asymptomatic. The remarkable recurrence of pain after NSAID discontinuation, despite an intact discectomy site, suggested an inflammatory trigger related to the tumor. Emerging research indicates that schwannomas are not merely collections of Schwann cells, but contain a dynamic TME composed of fibroblasts, macrophages, mast cells, and inflammatory cytokines [3,7]. These immune elements can induce local inflammation and peritumoral edema, contributing to pain and neurological symptoms even in benign lesions [8]. Anti-inflammatory therapy, such as NSAIDs or corticosteroids, can transiently suppress cytokine-mediated inflammation within the TME, thereby alleviating symptoms [9]. In this patient, the post-operative pain-free interval corresponded to the period of NSAID use. Symptom recurrence after stopping NSAIDs likely reflected reactivation of inflammatory processes surrounding the schwannoma. Surgical excision remains the definitive treatment for symptomatic schwannomas [10]. The complete resolution of symptoms following tumor removal supports the hypothesis that inflammatory activity within or around the schwannoma, rather than mechanical compression alone, played a significant role in the clinical presentation.
This case underscores the importance of considering nerve sheath tumors in patients with recurrent or atypical radicular symptoms following lumbar disc surgery. The TME and associated inflammatory response may significantly influence symptom development. Early recognition and excision of the schwannoma led to complete pain relief. Anti-inflammatory therapy, while providing temporary benefit, may mask underlying tumor-related inflammation and delay diagnosis.
Schwannomas are benign tumors that arise from nerve sheath, and they can indeed mimic symptoms of a prolapsed intervertebral disc, such as radiculopathy. The tumor location and growth can compress the adjacent nerve roots, leading to similar symptoms. The presence of a TME in schwannoma can lead to inflammation, which may respond to anti-inflammatory medications, temporarily alleviating symptoms. However, this can also leads to delayed diagnosis, as the symptoms may be misattributed to a more common condition like a herniated disc.
References
- 1. Conti P, Pansini G, Mouchaty H, Capuano C, Conti R. Spinal neurinomas: Retrospective analysis and long-term outcome of 179 consecutively operated cases and review of the literature. Surg Neurol 2004;61:34-43; discussion 44. [Google Scholar] [PubMed]
- 2. Kim HS, Ju CI, Kim SW, Lee SM. Concomitant lumbar disc herniation and spinal schwannoma: A case report and review of literature. J Korean Neurosurg Soc 2007;42:344-6. [Google Scholar] [PubMed]
- 3. Torres-Mejía E. The tumor microenvironment in schwannomas: From bench to bedside. Front Oncol 2021;11:705592. [Google Scholar] [PubMed]
- 4. Chen Z, Pradhan S, Liu C, Le LQ. Mechanisms of schwannoma pain and behavior: A perspective from tumor microenvironment. Front Immunol 2020;11:1455. [Google Scholar] [PubMed]
- 5. Yoon KW, Park JH, Kim YJ. Coexistence of lumbar disc herniation and schwannoma causing radiculopathy: Case report. Spine (Phila Pa 1976) 2013;38:E195-8. [Google Scholar] [PubMed]
- 6. Ahn SH, Cho YW, Ahn MW, Jang SH, Sohn YK, Kim HS. Surgical treatment for spinal schwannoma: Efficacy and safety. J Korean Neurosurg Soc 2008;44:273-8. [Google Scholar] [PubMed]
- 7. Monterde B. Macrophage polarization and inflammation in schwannoma. Cancers (Basel) 2022;14:2894. [Google Scholar] [PubMed]
- 8. Kalamarides M. Inflammation and microenvironment in schwannomas. Neurooncol Adv 2020;2 Suppl 1:i37-45. [Google Scholar] [PubMed]
- 9. Okamoto Y. NSAIDs suppress peritumoral inflammation and improve neuropathic pain behavior in schwannoma models. J Neurooncol 2019;142:67-75. [Google Scholar] [PubMed]
- 10. Safaee M, Oh MC, Barbaro NM, Theodosopoulos PV, Lawton MT, Chou D, et al. Surgical outcomes in spinal schwannomas: Clinical article. J Neurosurg Spine 2014;21:701-8. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Anteromedial Knee Pain Unmasked: Schwannoma of the Infrapatellar Branch of the Saphenous Nerve – A Rare Case Report
January 1, 2026 Anteromedial Knee Pain Unmasked: Schwannoma of the Infrapatellar Branch of the Saphenous Nerve – A Rare Case Report August 1, 2025 Hidden in Plain Palm: A Rare Case of Incidental Thenar Schwannoma
August 1, 2025 Hidden in Plain Palm: A Rare Case of Incidental Thenar Schwannoma September 10, 2023 Schwannoma of the Sciatic Nerve as a Cause of Extra-articular Knee Pain: Case Report and Literature Review
September 10, 2023 Schwannoma of the Sciatic Nerve as a Cause of Extra-articular Knee Pain: Case Report and Literature Review- December 10, 2020 Tibial Nerve Schwannoma: An Unexplained Cause of Lateral Foot Pain – A Rare Case Report and Review