
Cemented THR is an appropriate approach for a pathological fracture neck of the femur with a unicameral bone cyst in an elderly patient.
Dr. Sarang Shete, Department of Orthopaedics, KAHER’S Jawaharlal Nehru Medical College, Belagavi - 590010, Karnataka, India. E-mail:drsarangshete@gmail.com
Introduction: Unicameral (simple) bone cysts (UBCs) are fluid-filled intramedullary cavities commonly seen in the metaphysis of long bones in young patients under the age of 20 years. Pathological hip fractures associated with UBCs in the proximal femur are rare, especially in non-osteoporotic elderly patients. The management of such tumors, such as benign lesions of bone causing pathological fractures at the biomechanically critical load-bearing zone of the neck of the femur, remains a clinical challenge due to limited literature on optimal treatment strategies.
Case Report: A 60-year-old non-osteoporotic male presented with right hip pain and inability to walk for 10 days, without any history of recent trauma. X-ray pictures revealed a pathological hip fracture of the right hip in the neck of the femur with an associated lytic lesion with benign radiological appearance. Computed tomography scan confirmed a bony cystic lesion, whereas a DEXA scan ruled out osteoporosis. Oncological workup excluded any metastatic pathology, and the patient was managed surgically with cemented total hip replacement (THR). Intraoperatively, a cystic lesion in the femoral neck was excised and sent for histopathological analysis, which confirmed it to be a unicameral (simple) bone cyst. The patient was mobilized on the first post-operative day and achieved excellent functional recovery, with a Harris Hip Score of 90 at 3-month follow-up.
Conclusion: Pathological fractures of the femoral neck due to UBCs are exceptionally rare in elderly patients. This case highlights the successful management of a unicameral bone cyst with cemented THR, demonstrating that THR can be a viable treatment option for pathological hip fractures due to benign bone lesions in older adults.
Keywords: Bone cysts, pathological fracture, femoral neck fracture, total hip replacement.
Unicameral bone cyst (UBC), also known as a simple bone cyst (SBC), is an intramedullary fluid-filled cavity containing serous or serosanguinous fluid in the metaphysis of long bones, commonly seen in patients under 20 years of age [1]. The proximal femur is the 2nd most common site of unicameral bone cyst following the proximal humerus [1,2,3]. It is usually an incidental finding, or they present with pain due to pathological fractures [3]. The management of pathological hip fractures due to metastatic carcinomatous lesions is well-studied. However, the approach to a benign lesion of the hip causing a pathological fracture is rarely seen, owing to its benign nature. Hence, we report a rare case of a pathological fracture neck of the femur caused by a SBC, which was successfully treated with cemented total hip replacement (THR) surgery.
A 60-year-old male patient presented with complaints of right hip pain and inability to bear weight on his right lower limb for 10 days, with no history of recent trauma. The patient also had a history of neck of femur fracture in his left hip due to a traumatic cause, which was treated with uncemented hemiarthroplasty (elsewhere) 4 years ago. Clinical examination revealed shortening of the right lower limb, groin tenderness, and absent active SLR with no distal neurovascular deficits. X-ray of the pelvis with both hips revealed a pathological fracture in the right neck of the femur with a lytic lesion at the basicervical region of the neck of the femur (Fig. 1).
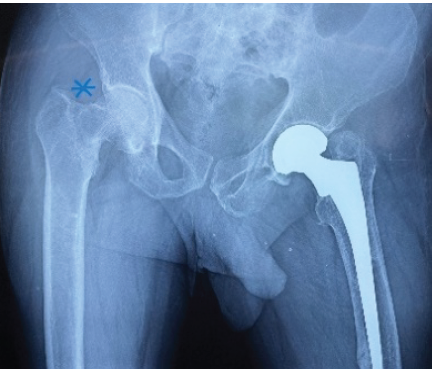
Figure 1: Pre-operative radiograph revealing an osteolytic lesion in the right neck of the femur (blue asterisk) and left hip bipolar implant in situ.
Computed tomography (CT) of the pelvis with both hips was performed, which confirmed the X-ray findings (Fig. 2).
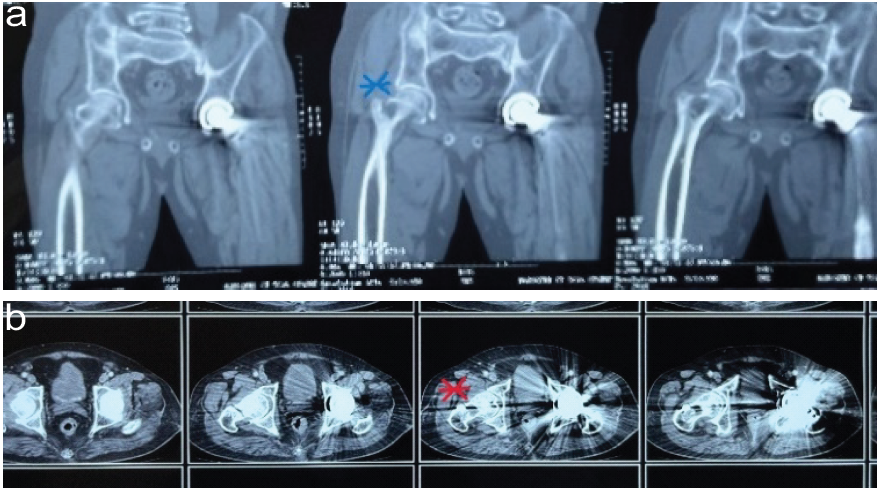
Figure 2: (a) Computed tomography (CT) scan coronal view (blue asterisk) confirms radiographic findings. (b) CT scan axial view with a red asterisk suggests the extent of the lytic bony lesion.
DEXA scan revealed no evidence of osteoporosis, and the patient underwent an oncological workup to rule out any metastatic cause for the pathological fracture. The patient subsequently underwent right cemented THR using the lateral approach. A cyst-like lesion was identified in the right femoral neck, which was excised and sent for histopathological examination. The patient’s post-operative radiograph was satisfactory (Fig. 3), and the patient was ambulated on the 1st post-operative day with support. The staples were removed after 2 weeks.
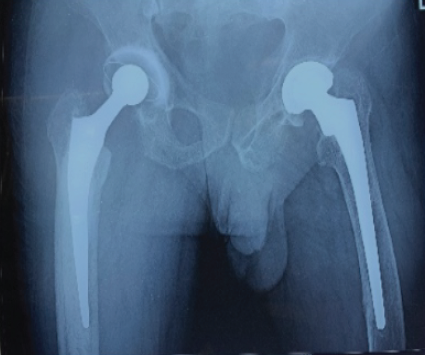
Figure 3: Post-operative radiograph showing cemented total hip replacement (right hip).
Histopathological examination revealed Gray-brown soft-tissue pieces with three blackish soft-tissue pieces from the neck of the femur containing brownish gelatinous fluid. On microscopic examination, the sections from the neck of the femur showed necrotic bone, granulation tissue, hemorrhage, and hemosiderin-laden macrophages. Sections from the cyst showed connective tissue, histiocytes, and hemosiderin pigment, suggestive of a unicameral bone cyst (Fig. 4).
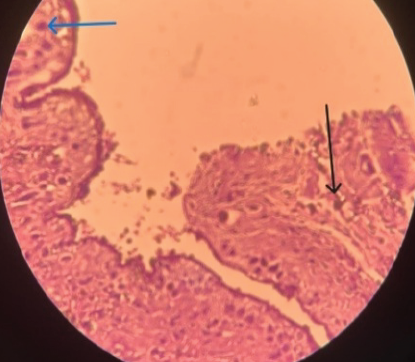
Figure 4: Histopathological image of a biopsy specimen’s Unicameral bone cyst confirms the diagnosis, with the black arrow suggesting hemosiderin-laden macrophages and fibroblasts, whereas the blue arrow suggests osteoblasts and osteoclasts.
A unicameral (simple) bone cyst is a uniloculated fluid-filled cavity usually seen in the metaphysis of long bones. More than 85% of bone cysts occur in patients under 20 years of age, with males being twice as commonly affected as females [1,2,3]. The proximal humerus and proximal femur are the most commonly involved bones, although it can occur in any bone. However, above the age of 20 years, SBCs are found to occur in the ilium and calcaneus [2]. These lesions are most active during skeletal growth, and most of them heal spontaneously. It is hypothesized that cysts are formed due to intramedullary venous occlusions [1]. SBCs are classified as active if the cyst is within 1 cm of the growth plate and latent if the lesion is beyond 1 cm from the growth plate, making it closer to the diaphysis [2]. These are mostly asymptomatic unless there is pain due to a pathological fracture. In the case of a pathological fracture, the cyst heals spontaneously in 2/3rd of such cases. However, this has not been reported for UBCs, causing pathological fractures of the hip in the current literature. Moreover, the biomechanical forces acting on the hip are too high to anticipate spontaneous healing at the fracture site of the femoral neck [1,4]. Radiologically, a unicameral bone cyst appears as a well-circumscribed osteolytic lesion located centrally. A periosteal reaction is observed in pathological fractures. The pathognomonic sign of a pathological fracture due to SBC is the “Fallen fragment sign,” which was not observed in our case [2]. Usually, magnetic resonance imaging (MRI) is essential to assess other extra-articular or non-bony cystic lesions of the hip [5]. We avoided an MRI owing to the pre-existing bipolar stainless steel implant in the contralateral hip and performed a CT scan. This patient had a contralateral hip fracture 4 years earlier owing to a trivial fall, which raised the possibility of a benign cystic lesion in the left hip. As a biopsy was not performed previously, it emphasizes the importance of biopsies if retrospectively analyzed for the possibility of bilateral UBCs in such cases of non-traumatic etiology. Unicameral bone cysts contain yellowish colored serous material, and a fibrous membrane lines the cavity wall. Deep to this lining, it contains fragments of immature bone, osteoclast giant cells, mesenchymal cells, and occasionally lymphocytes [2,6]. In case of a pathological fracture, the cystic fluid is discolored due to occult bleeding as seen in the histopathology and pathological examination report. Treatment for small lesions, if asymptomatic, is regular follow-ups and radiographs. Larger-sized lesions that are at risk of pathological fracture are treated surgically. These include curettage and bone graft or internal fixation, or less invasive options such as aspiration and injection of corticosteroid/bone marrow aspirate [2]. In young patients, non-arthroplasty surgeries can be considered [7]. However, in older patients with SBC in the neck of the femur leading to a pathological fracture, total hip arthroplasty is a better-suited treatment option. Cemented THR may have a better outcome as compared to uncemented THR [8]. As our patient was a 60-year-old with pre-existing contralateral uncemented bipolar hemiarthroplasty, Cemented THR was done successfully. A post-operative Harris Hip Score of 90 was achieved at 3 months follow-up. There is limited literature regarding the treatment of pathological fractures due to UBC. The current case report throws light on success in the management of a UBC causing a pathological fracture in the neck of the femur of an elderly male with curettage of the cyst and cemented THR. Interestingly, UBCs are among the uniquely placed benign bone tumors that can be reflected in all three stages of Enneking’s classification for benign tumor-like lesions [9,10]; hence, orthopedic surgeons must be familiar with the spectrum of benign bone tumors and the approach to their surgical management.
The choice of treatment of benign lesions of bone may present as a clinical challenge for many surgeons. Cemented THR should be considered a successful treatment option for pathological hip fractures due to UBC with pre-operative planning. Early outcome following this surgery is akin to the surgeries performed for pathological fractures of the neck of the femur due to osteoporosis encountered at this age.
Elderly patients with hip fractures of non-traumatic etiology require biopsy and have excellent clinical outcomes if treated with cemented THR in cases of unicameral bone cysts.
References
- 1. Turek SL. Unicameral bone cyst. In: Turek’s Orthopaedics: Principles and their Applications. 6th ed. New Delhi: Wolters Kluwer (India) Pvt. Ltd.; 2016. p. 646-7. [Google Scholar] [PubMed]
- 2. Dormans JP. Unicameral bone cyst. In: Azar FM, Beaty JH, Canale ST, editors. Campbell’s Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021. p. 969-71. [Google Scholar] [PubMed]
- 3. Jaffe HL. Solitary unicameral bone cyst. J Bone Joint Surg Am 1942;24:1004-14. [Google Scholar] [PubMed]
- 4. Callaghan JJ, Rosenberg AG, Rubash HE. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007. [Google Scholar] [PubMed]
- 5. Yukata K, Nakai S, Goto T, Ikeda Y, Shimaoka Y, Yamanaka I, et al. Cystic lesion around the hip joint. World J Orthop 2015;6:688-704. [Google Scholar] [PubMed]
- 6. Cohen J. Simple bone cysts. Studies of cyst fluid in six cases with a theory of pathogenesis. J Bone Joint Surg Am 1960;42-A:609-16. [Google Scholar] [PubMed]
- 7. Ruiz-Arellanos K, Larios F, Inchaustegui ML, Gonzalez MR, Pretell-Mazzini J. Treatment and outcomes of 4,973 unicameral bone cysts: A systematic review and meta-analysis. JBJS Rev 2024;12:e23.00159. [Google Scholar] [PubMed]
- 8. Raja BS, Gowda AK, Singh S, Ansari S, Kalia RB, Paul S. Comparison of functional outcomes and complications of cemented vs uncemented total hip arthroplasty in elderly neck of femur fracture patients: A systematic review and meta-analysis. J Clin Orthop Trauma 2022;29:101876. [Google Scholar] [PubMed]
- 9. Capanna R, Campanacci DA, Manfrini M. Unicameral and aneurysmal bone cysts. Orthop Clin North Am 1996;27:605-14. [Google Scholar] [PubMed]
- 10. Pala E, Trovarelli G, Angelini A, Cerchiaro MC, Ruggieri P. Modern treatment of unicameral and aneurysmatic bone cysts. EFORT Open Rev 2024;9:387-92. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Surgeon-Performed Intraoperative Pericapsular Nerve Group Block in Total Hip Replacement: A Cadaveric Feasibility Study
March 1, 2026 Surgeon-Performed Intraoperative Pericapsular Nerve Group Block in Total Hip Replacement: A Cadaveric Feasibility Study February 1, 2026 Fungal Infection of Native Hip Joint Presenting as Secondary Arthritis in 52-Year-Old Male – A Rare Case Report
February 1, 2026 Fungal Infection of Native Hip Joint Presenting as Secondary Arthritis in 52-Year-Old Male – A Rare Case Report February 1, 2026 Impaired Bone Healing and Fracture Complications during Limb Lengthening in a Neurofibromatosis Type 1 Patient Receiving Selumetinib: Case Report and Literature Review
February 1, 2026 Impaired Bone Healing and Fracture Complications during Limb Lengthening in a Neurofibromatosis Type 1 Patient Receiving Selumetinib: Case Report and Literature Review January 1, 2026 Harnessing 3D Printing Technology for Complex Acetabular Reconstruction in Revision Total Hip Arthroplasty: From Childhood Hip Trauma to Customized Modern Solutions
January 1, 2026 Harnessing 3D Printing Technology for Complex Acetabular Reconstruction in Revision Total Hip Arthroplasty: From Childhood Hip Trauma to Customized Modern Solutions