
Retrograde elastic nail fixation of humeral shaft fractures in children with two nails through a central entry point is a reliable technique, with a low risk of complications.
Dr. Sudhir Shankar Mane, Department of Orthopaedics, First Floor, SVS Medical College and Hospital, Yenugonda, Mahabubnagar - 509002, Telangana, India. E-mail: sdhrmane@gmail.com
Introduction: Almost all paediatric humerus fractures can be managed conservatively with a high rate of union. Surgical intervention may be indicated in a few scenarios. Retrograde nailing with titanium elastic nails through a central entry point proximal to the olecranon fossa offers several advantages when surgical fixation is indicated.
Case Report: Three male patients in the age group of 5–14 years with diaphyseal left humerus fractures were treated with retrograde elastic nailing after failed conservative management. The mean age of the patients was 10 years. All the surgeries were performed under general anaesthesia. The mean operative time was 100 minutes. The mean union time was 12 weeks. The mean follow-up duration was 26.3 months. One patient developed a superficial surgical site infection, and the nails had to be removed 9 weeks after the surgery. The QuickDASH score of all the patients 3 months after surgery was zero, indicating no disability. All patients had excellent outcomes.
Conclusion: When surgical stabilization of paediatric humeral shaft fractures is indicated, retrograde elastic nail fixation with two nails through a central entry point is a reliable technique, with a low risk of complications, offering stable fixation that eliminates the need for uncomfortable immobilization and enables early mobilization of the arm.
Keywords: Retrograde elastic nailing, pediatric humerus fractures, titanium elastic nails.
Humeral shaft fractures are uncommon in children, representing 0.4% to 3% of all paediatric fractures and 10% to 20% of humeral fractures. [1]. Almost all paediatric humerus fractures can be managed conservatively with a high rate of union. Authors suggest that before opting for non-operative treatment, the deformity should be reduced to within 30° for fractures of the proximal third, 20° for those in the middle third, and 15° for fractures of the distal third of the shaft [2]. Surgical intervention may be required in cases of polytrauma to enable early mobilization, in compound fractures for wound management, in patients with head injuries to facilitate nursing care, in pathologic fractures, and in certain instances with unacceptable angulation to preserve proper alignment [3,4]. Several techniques of retrograde nailing with titanium elastic nails for humerus fractures have been described. Antegrade nailing is not preferred due to violation of the rotator cuff, the possibility of injury to the growth plate, and impingement on the shoulder. Plate osteosynthesis is not recommended for humerus fractures in children. Retrograde Ender nails may be used [5]. Alternatively, titanium or stainless steel elastic nails may also be used. The most commonly used technique for retrograde nailing involves making a small skin incision and entry over the medial and lateral epicondyles [3]. Skaggs and Frick described another technique where two elastic nails are inserted in a retrograde manner through a central entry point on the posterior aspect of the humerus, slightly proximal to the olecranon fossa [4]. This technique was used to treat three children with humerus shaft fractures in whom conservative methods had failed. Very few studies in the literature have reported the long-term outcomes using this method. This case series includes three boys aged 7 years, 9 years, and 14 years (Table 1) with closed middle-third fractures of the left humerus who underwent retrograde titanium elastic nailing through a central entry point using the technique described by Skaggs and Frick. None of the patients had neurovascular injury or associated injuries. All the surgeries were done under general anaesthesia by the same surgeon.
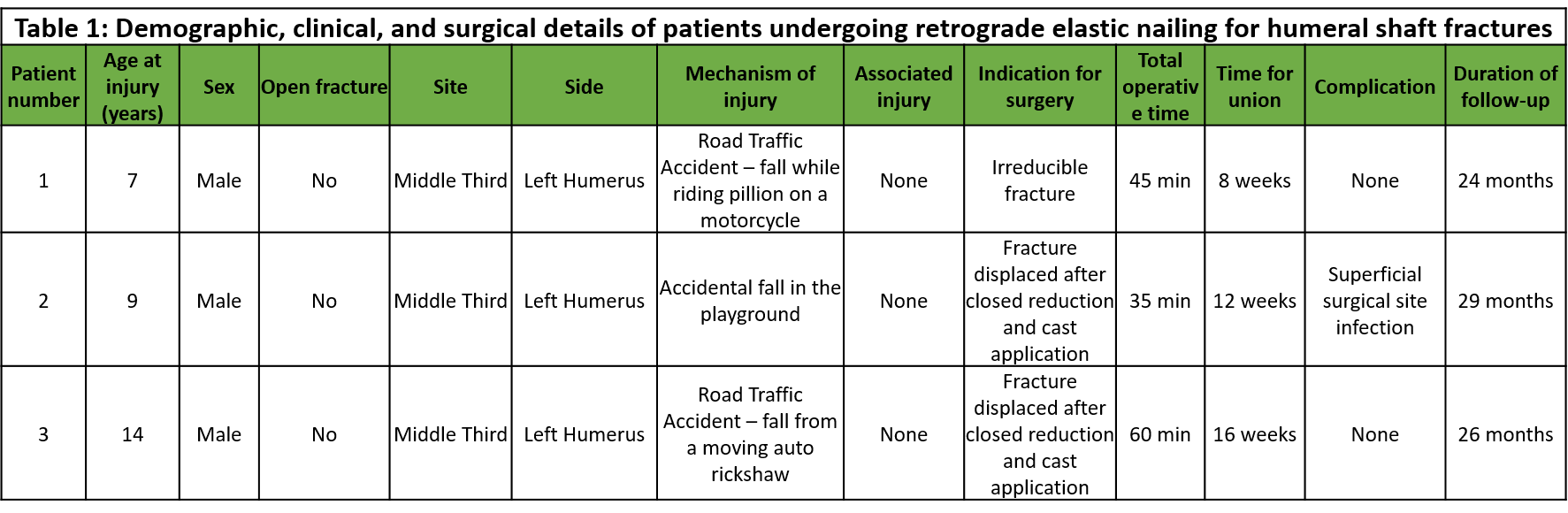
Table 1: Demographic, clinical, and surgical details of patients undergoing retrograde elastic nailing for humeral shaft fracture.
Surgical Technique and Post-operative Protocol
This technique has been described in detail in Lovell and Winter’s Pediatric Orthopaedics [4]. The patient was kept in a supine position with the arm on a radiolucent table. A posterior midline skin incision was made extending from the olecranon fossa proximally for about 4 to 6 cm, depending on the size of the patient. The incision was made sharply down through the triceps fascia, and the triceps muscle was split by blunt dissection to expose the posterior surface of the humerus (Fig. 1a). Care was taken to avoid the radial nerve. The radial
nerve is located about 10 cm proximal to the lateral epicondyle in adults, but this distance is comparatively lesser in children [4]. An entry point (Fig. 1b) was made with a drill or a straight bone awl above the olecranon fossa to access the medullary canal, with the distance adjusted according to the child’s size. Careful attention
must be given when creating the entry point to minimize the risk of an iatrogenic fracture with the drill/bone awl. The size of the elastic nail was determined by placing it next to the humerus and viewing both with an image intensifier. The elastic nail was bent slightly in the distal part. The nail was inserted, driven to the fracture site (Fig. 2a), and passed into the proximal fragment after reduction (Fig. 2b). A second rod was inserted for rotational stability, with one nail directed toward the greater tuberosity and the other toward the humeral head
(Fig. 2c). The nails were positioned correctly under fluoroscopic guidance using an image intensifier. The excess
length of the elastic nail was trimmed, leaving sufficient length for easy removal (Fig. 2d). Fluoroscopy ensures proper positioning and fracture reduction. A sling was provided after surgery for stabilization. Range-of motion exercises were started after 3–4 weeks, after sufficient healing had occurred. The elastic nails were removed electively after union of the fracture in two patients.
Patient 1
A 7-year-old boy presented with a closed fracture involving the middle third of the left humerus (Fig. 3a), sustained from a road traffic accident after falling while riding as a pillion on a motorcycle. The fracture was irreducible through conservative means, necessitating surgical intervention (Fig. 3b). The fracture united within 8 weeks (Fig. 3c), with no reported complications. Implant removal was done after 3 months. The patient was followed up for 24 months, demonstrating satisfactory recovery and healing with a full range of motion (ROM) at the shoulder and elbow (Fig. 3d and e).
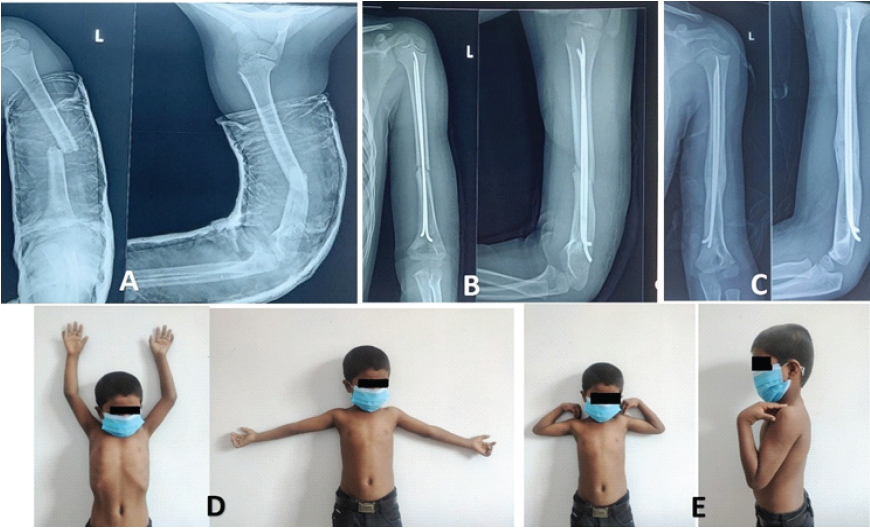
Figure 3: (a) Pre-operative X-ray of Patient 1, (b) Immediate post-operative X-ray of Patient 1, (c) Follow-up X-ray at 8 weeks, (d and e) Full range of motion at the shoulder and elbow after implant removal.
Patient 2
A 9-year-old boy sustained a closed fracture of the middle third of the left humerus due to an accidental fall in a playground. Initially managed with closed reduction and cast application, the fracture subsequently displaced (Fig. 4a), warranting surgical treatment (Fig. 4b). Callus formation was achieved at 6 weeks (Fig. 4c). However, the patient experienced a superficial surgical site infection necessitating implant removal. The fracture united in 12 weeks. The infection was controlled with IV antibiotics, and the patient had no further complications. Follow-up continued for 29 months, showing good long-term outcomes and full ROM of the elbow.
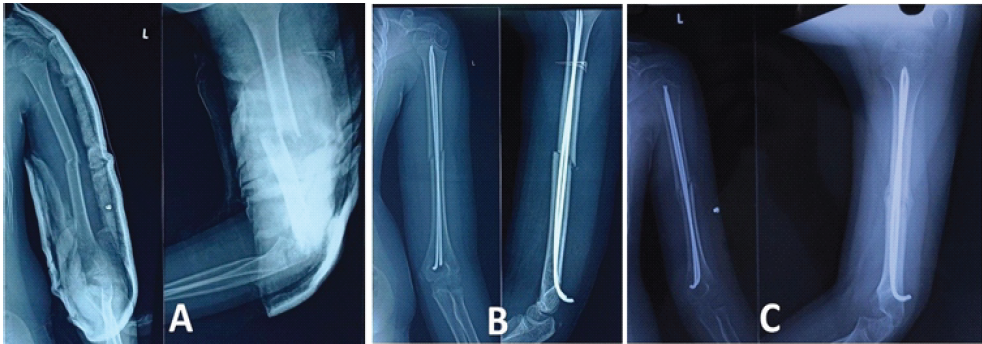
Figure 4: (a) Pre-operative X-ray of Patient 2, (b) Immediate post-operative X-ray of Patient 2, (c) Follow-up X-ray at 9 weeks when implant removal was planned.
Patient 3
A 14-year-old boy suffered a closed fracture of the middle third of the left humerus (Fig. 5a) following a road traffic accident, involving a fall from a moving auto rickshaw. Despite initial conservative management with cast application, the fracture was found to be displaced, necessitating surgical intervention (Fig. 5b). Fracture union occurred within 16 weeks, with no reported complications. Implant removal was done at 4 months. The patient was followed up for 60 months, indicating a favorable outcome with no residual issues and full ROM in the elbow.
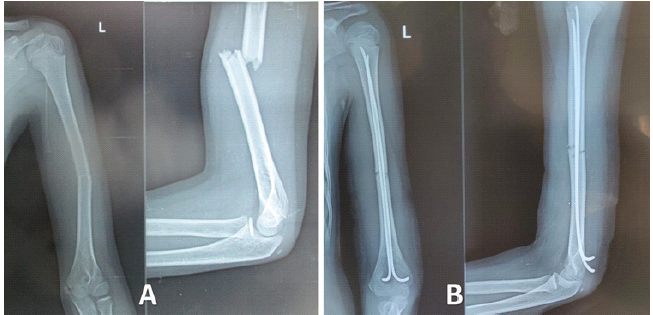
Figure 5: (a) Pre-operative X-ray of Patient 3, (b) Immediate post-operative X-ray of Patient 3.
We present a case series of three boys aged 7 years, 9 years, and 14 years with closed middle third fractures of the left humerus treated with retrograde titanium elastic nail fixation through a single entry point made proximal to the olecranon fossa. The outcomes in our case series were excellent. All the patients had a full range of motion in the elbow joint. Only one patient had to undergo implant removal earlier than indicated due to a superficial surgical site infection. In this study, the average age of the patients was 10 years, with a mean fracture union time of 12 weeks and an average follow-up duration of 26.3 months. The QuickDASH score [6] for all patients at 3-month follow-up was 0, indicating no disability. All fractures achieved healing in good alignment, with no intraoperative complications such as neurologic or vascular injuries. Closed reduction may occasionally fail due to the interposition of muscle or periosteum between the fracture ends. In patients where closed reduction fails, open reduction may be attempted by making a skin incision over the fracture site. A retrospective study of 13 patients (mean age 12.0 years) by Garg et al. from the USA reported that all fractures healed in good alignment with no intraoperative complications or infections [3]. The dual entry point technique with two nails was followed in 11 patients, whereas antegrade nailing was done for two patients. Two cases of nail migration occurred, including one with skin protrusion, and one patient required tendon transfer for pre-operative radial nerve injury. Notably, 12 of 13 patients returned to full activities without limitations, aligning with our study’s findings. Samara et al. reported a single nail technique of retrograde nailing for proximal humerus fractures in 19 children, where the entry point was made 10–20 mm proximal to the lateral epicondyle [7]. All fractures appeared united on the radiographs at a median of 6 weeks. A Nepali study that included 28 children reported excellent results in 85.71% of patients and good outcomes in 14.29% [8]. A single retrograde nail was used. The average patient age was 8.85 ± 1.84 years (range: 6–12), and the mean time to fracture union was 8.28 ± 2.43 weeks (range: 6–12). Complications included one case each of malunion (~10°), nail migration, superficial infection, transient radial nerve palsy, and nail protrusion. Wang et al. from China reported excellent outcomes in 37 children using the dual entry point technique for the proximal humerus [9]. They reported skin irritation due to protruding hardware at the distal humerus in two cases. This was resolved after implant removal. The mean union time was 8 weeks (range 7–10 weeks) after surgery. A Korean study evaluated the antegrade and retrograde two-nail technique in 12 patients [10]. No neurovascular injuries or infections occurred during surgery. However, four patients experienced nail site irritation, with two requiring early nail removal at 6 weeks due to skin lesions and pain. One boy had a fracture near the proximal nail insertion site. All patients regained a full range of motion and returned to daily life by the final follow-up.

Table 2: Comparative analysis of outcomes and techniques from various studies on retrograde elastic nailing for humeral shaft fractures in children.
The retrograde double nail technique through a central entry point offers more advantages compared to the single nail technique, though the single nail technique is quicker and more cost-effective. However, the insertion of two nails provides better rotational stability [5,9]. Compared to conservative management, surgical intervention allows quicker recovery, and inconvenient immobilization can be avoided. Surgical fixation allows polytrauma patients with lower limb injuries to be mobilized earlier with the aid of assistive devices such as walkers and crutches. The key findings of all the studies are compared in Table 2. There are a few limitations in this study. The case series included only three patients who were operated on by a single surgeon. Future multicentric studies with a large sample size and longer follow-up duration can provide more insights into how fractures treated by this method remodel over time.
In children where surgery is indicated, retrograde elastic nail fixation of humeral shaft fractures with two nails through a central entry point is a reliable technique, with a low risk of complications, offering stable fixation that eliminates the need for uncomfortable immobilization and enables early mobilization of the arm.
Fixation of humeral shaft fractures in children with retrograde elastic nails through a central entry point is a reliable technique with several advantages and should be considered when surgical fixation is indicated.
References
- 1. Wiktor Ł, Tomaszewski R. Humeral Shaft Fractures in Children Incidence, Management and Treatment Effects. Ortop Traumatol Rehabil. 2022 Aug 31;24(4):251-261. [Google Scholar] [PubMed]
- 2. Webb L, Mooney J. Fractures and dislocations about the shoulder. In: Green N, Swiontkowski M, editors. Skeletal Trauma in Children. Philadelphia, PA: WB Saunders; 2003. p. 322-43. [Google Scholar] [PubMed]
- 3. Garg S, Dobbs MB, Schoenecker PL, Luhmann SJ, Gordon JE. Surgical treatment of traumatic pediatric humeral diaphyseal fractures with titanium elastic nails. J Child Orthop 2009;3:121-7. [Google Scholar] [PubMed]
- 4. Skaggs DL, Frick S. Chapter 33: Upper extremity fractures in children. In: Lovell WW, Weinstein SL, Flynn JM, editors. Lovell and Winters’ Pediatric Orthopaedics. 7th ed. Vol. 2. Philadelphia (PA): Wolters Kluwer Health/Lippincott Williams & Wilkins; 2014. p. 17034–1706. [Google Scholar] [PubMed]
- 5. Shazar N, Brumback RJ, Vanco B. Treatment of humeral fractures by closed reduction and retrograde intramedullary ender nails. Orthopedics 1998;21:641-6. [Google Scholar] [PubMed]
- 6. Beaton DE, Wright JG, Katz JN, Upper Extremity Collaborative Group. Development of the QuickDASH: Comparison of three item-reduction approaches. J Bone Joint Surg Am 2005;87:1038-46. [Google Scholar] [PubMed]
- 7. Samara E, Tschopp B, Kwiatkowski B, Vardar E, Lutz N, Zambelli PY. A single retrograde intramedullary nail technique for treatment of displaced proximal humeral fractures in children: Case series and review of the literature. JBJS Open Access 2021;6:e20.00119. [Google Scholar] [PubMed]
- 8. Kapil Mani KC, Acharya P, Pangeni BR, Marahatta SB. Pediatric humeral fracture fixed by a single retrograde titanium elastic nail. Apollo Med 2017;14:212-7. [Google Scholar] [PubMed]
- 9. Wang X, Shao J, Yang X. Closed/open reduction and titanium elastic nails for severely displaced proximal humeral fractures in children. Int Orthop 2013;38:107-10. [Google Scholar] [PubMed]
- 10. Kwak YH, Min SK, Lee YB, Park KB. Operative treatment of pediatric humeral diaphyseal fractures with flexible intramedullary nails. J Korean Orthop Assoc 2012;47:250-6. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 Outcome of Clavicle Fractures Treated by Various Modalities
June 1, 2025 Outcome of Clavicle Fractures Treated by Various Modalities July 10, 2024 Bilateral Anterior Cruciate Ligament Reconstruction with All-Inside Technique for Adolescent: A Review of the Literature and Case Report
July 10, 2024 Bilateral Anterior Cruciate Ligament Reconstruction with All-Inside Technique for Adolescent: A Review of the Literature and Case Report March 10, 2021 Spontaneous Early Intraprosthetic Dislocation of 22 mm Skirted Femoral Head in Dual Mobility Hip Prosthesis: A Case Report
March 10, 2021 Spontaneous Early Intraprosthetic Dislocation of 22 mm Skirted Femoral Head in Dual Mobility Hip Prosthesis: A Case Report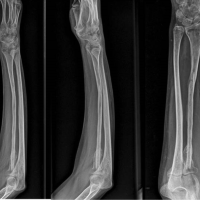 May 10, 2022 Fibrous Dysplasia of Radius Bone-excision and Fibula Graft: A Case Report
May 10, 2022 Fibrous Dysplasia of Radius Bone-excision and Fibula Graft: A Case Report