
Syndromic clubfoot associated with Nail-Patella Syndrome should not be presumed rigid or resistant. With early diagnosis and timely intervention, excellent outcomes can be achieved through conservative treatment using the Ponseti method.
Dr. Burhanuddin F Chhatriwala, Department of Orthopaedics, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India. E-mail: burhan110128@hotmail.com
Introduction: Nail-patella syndrome (NPS) is a rare autosomal dominant disorder characterized by nail dysplasia, hypoplastic or absent patellae, elbow anomalies, and iliac horns. Its association with congenital talipes equinovarus, or clubfoot, is extremely uncommon and rarely documented.
Case Report: We describe a 1.5-year-old male child, born of a 2° consanguineous marriage, who presented with bilateral clubfoot and complete absence of fingernails. Great toenails were absent bilaterally, whereas the remaining toenails were preserved. The patellae were non-palpable clinically, and ultrasound confirmed the absence of ossification centers bilaterally. Radiographs revealed bilateral iliac horns. Ponseti casting was initiated at 2 months of age, and full correction was achieved after five casts, followed by bilateral percutaneous Achilles tenotomy. At 6-month follow-up, the patient exhibited plantigrade, pain-free feet with good dorsiflexion and no recurrence.
Conclusion: NPS can occasionally be associated with flexible clubfoot, which may respond well to conservative management. The Ponseti method, when initiated early, remains an effective option in such rare syndromic presentations.
Keywords: Nail-patella syndrome, clubfoot, Ponseti method, congenital talipes equinovarus, syndromic clubfoot, LMX1B mutation.
Nail-patella syndrome (NPS), also known as hereditary onycho-osteodysplasia, is a rare autosomal dominant condition caused by mutations in the LMX1B gene on chromosome 9. This gene plays a crucial role in dorsal limb patterning, nephron development, and anterior segment formation in the eye [1]. NPS is characterized by classical musculoskeletal features, including nail dysplasia, hypoplastic or aplastic patellae, elbow anomalies, and pathognomonic iliac horns on pelvic radiographs [2]. Renal involvement and open-angle glaucoma may also be seen in some patients.
Congenital talipes equinovarus (CTEV), or clubfoot, is a congenital foot deformity characterized by hindfoot equinus and varus, forefoot adduction, and cavus. It occurs in approximately 1–7/1000 live births [3]. While most cases are idiopathic, about 20% are syndromic or associated with underlying neuromuscular conditions [4]. The association between NPS and CTEV is rare, with only a few cases described. The Ponseti method has become the gold standard in the management of CTEV, including many syndromic variants.
A 1.5-year-old male child was brought to our clinic with bilateral clubfoot noted since birth. He was the third child of healthy parents in a 2° consanguineous marriage. The elder siblings were developmentally normal. The antenatal and birth history were uneventful.
On examination, the child had bilateral clubfoot with equinus, hindfoot varus, forefoot adduction, and mild cavus deformity. The pre-casting Pirani Scoring was 5 in the right leg and 5.5 in the left leg. All fingernails were absent on both hands (Fig. 1 and 2).

Figure 1: Right hand dorsal aspect.

Figure 2: Left hand dorsal aspect.
Toenails were present on all toes except the great toes bilaterally, which were anonychic (Figs. 3 and 4). The patellae were not palpable clinically. The elbow range of motion was full, and the rest of the musculoskeletal and systemic examination was unremarkable.

Figure 3: Right foot dorsal aspect.
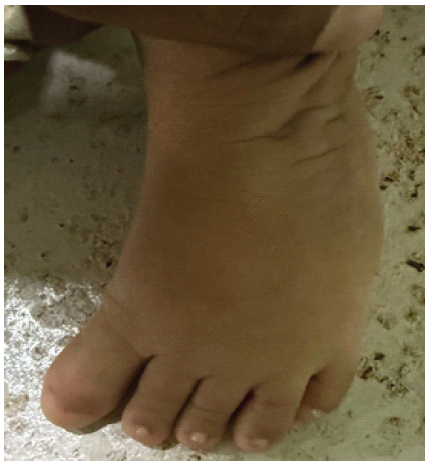
Figure 4: Left foot dorsal aspect.
Radiographs of the pelvis revealed bilateral iliac horns (Fig. 5). Ultrasound of the knees demonstrated absent ossification centers for both patellae (Fig. 6).

Figure 5: X-ray pelvis with both hips – anteroposterior with iliac horns. Marked with an arrow.
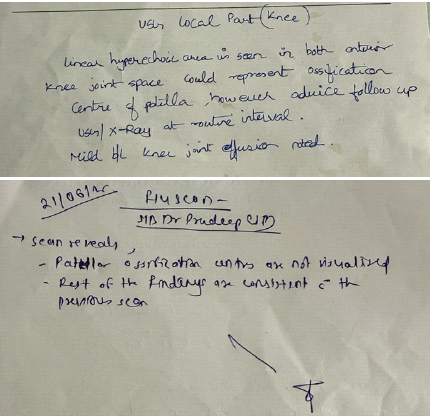
Figure 6: Ultrasound of the knee report.
There were no vertebral or renal anomalies on screening, and renal function tests were normal. Based on the combination of clinical and radiological findings – absent fingernails, great toenail dysplasia, iliac horns, and patellar aplasia – a diagnosis of NPS was made [1,2]. Genetic counseling was offered to the family.
Orthopedic management began at 2 months of age with serial weekly long leg casts according to the Ponseti protocol. Correction of the deformity was achieved in five casts. This was followed by bilateral percutaneous Achilles tenotomy and application of a final cast for 3 weeks. At the end of the tenotomy, the Pirani score was 0 for both legs. A foot abduction brace was prescribed, and bracing compliance was closely monitored.
At 6-month follow-up, the child had pain-free, plantigrade feet with 15° of dorsiflexion bilaterally. The Laaveg-Ponseti functional score was 95/100. No recurrence or brace intolerance was observed, and the child had begun to walk independently. The last follow-up images are given below (Fig. 1, 2, 3, 4).
NPS is a multisystem disorder with a highly variable presentation. Its hallmark skeletal findings include nail dysplasia, hypoplastic or absent patellae, and iliac horns [1,2]. These anomalies often go unrecognized unless specifically investigated, particularly in infants, where patellar ossification is delayed. [9] In our case, the complete absence of fingernails on both hands and great toenail aplasia prompted evaluation for syndromic causes. The identification of iliac horns on pelvic radiographs and absent patellar ossification confirmed the diagnosis of NPS.[10] These findings highlight the importance of a detailed musculoskeletal and radiological assessment in children with bilateral clubfoot and nail anomalies. Clubfoot in syndromic settings, particularly those involving neuromuscular conditions such as arthrogryposis or spina bifida, tends to be stiff, resistant to conservative methods, and associated with higher recurrence [4,5]. However, limited data suggest that NPS-associated clubfoot behaves more like idiopathic cases. Ey Batlle et al. reported a small series of four children with NPS and clubfoot, all successfully treated with the Ponseti method without recurrence [6]. Our patient responded well to early Ponseti casting started at 2 months of age. Complete correction was achieved in five casts, and results were maintained following tenotomy and bracing. This reinforces the notion that not all syndromic clubfeet should be presumed resistant to conservative treatment. Joint laxity, commonly described in NPS, may contribute to the favorable response and improved brace tolerance [7]. The presence of consanguinity in this case may explain the pronounced phenotypic features. While NPS is typically inherited in an autosomal dominant fashion, enhanced expression in consanguineous unions may reflect underlying homozygosity or more penetrant gene expression [8]. Overall, this case emphasizes the critical role of early recognition and comprehensive evaluation in syndromic clubfoot. When managed appropriately, children with NPS and associated CTEV can achieve excellent functional outcomes without the need for extensive surgical correction.
NPS should be considered in any child presenting with bilateral clubfoot and associated nail dysplasia, especially when patellae are not clinically palpable, and iliac horns are seen on radiographs. The Ponseti method remains a highly effective treatment, even in syndromic cases such as NPS, when initiated early and followed rigorously.
Clubfoot associated with Nail-patella syndrome, though rare, is responsive to conservative treatment. Complete absence of fingernails and great toenail aplasia should alert clinicians to this diagnosis. Iliac horns and patellar aplasia, detectable radiologically, support the diagnosis. Early initiation of the Ponseti method can result in excellent long-term outcomes.
References
- 1. Dreyer SD, Zhou G, Baldini A, Winterpacht A, Zabel B, Cole W, et al. Mutations in LMX1B cause abnormal skeletal patterning and renal dysplasia in nail patella syndrome. Nat Genet 1998;19:47-50. [Google Scholar] [PubMed]
- 2. Bongers EM, Huysmans FT, Levtchenko E, de Rooy JW, Blickman JG, Admiraal RJ, et al. Genotype-phenotype studies in nail-patella syndrome show that LMX1B mutation location is involved in the risk of developing nephropathy. Eur J Hum Genet 2005;13:935-46. [Google Scholar] [PubMed]
- 3. Dobbs MB, Gurnett CA. Update on clubfoot: Etiology and treatment. Clin Orthop Relat Res 2009;467:1146-53. [Google Scholar] [PubMed]
- 4. Janicki JA, Narayanan UG, Harvey B, Roy A, Wright JG. Treatment of neuromuscular and syndromic clubfeet using the Ponseti method. J Pediatr Orthop 2009;29:393-7. [Google Scholar] [PubMed]
- 5. van Bosse HJ. Challenging clubfeet: The arthrogrypotic clubfoot and the complex clubfoot. J Child Orthop 2019;13:271-81. [Google Scholar] [PubMed]
- 6. Ey Batlle AM, Vinyals RM, Míguez GP. Clubfoot associated with Nail-Patella Syndrome: Evolution and treatment with Ponseti method. Acta Sci Orthop 2022;5:30-3. [Google Scholar] [PubMed]
- 7. Moroney PJ, Noel J, Richards BS. A single-center prospective evaluation of the Ponseti method in non-idiopathic congenital talipes equinovarus. J Pediatr Orthop 2012;32:636-40. [Google Scholar] [PubMed]
- 8. Ghoumid J, Petit F, Holder-Espinasse M, Jourdain AS, Guerra J, Dieux-Coeslier A, et al. Nail-Patella Syndrome: Clinical and molecular data in 55 families raising the hypothesis of a genetic heterogeneity. Eur J Hum Genet 2016;24:44-50. [Google Scholar] [PubMed]
- 9. Bongers EM, Gubler MC, Knoers NV. Nail-patella syndrome. Overview on clinical and molecular findings. Pediatr Nephrol 2002;17:703-12. [Google Scholar] [PubMed]
- 10. Mankin HJ, Jupiter J, Trahan CA. Hand and foot abnormalities associated with genetic diseases. Hand (N Y) 2011;6:18-26. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Easy Cast Removal in Idiopathic Congenital Talipes Equinovarus: A Study on Modified Ponseti Technique using an Interposed Polythene Sheet
November 1, 2025 Easy Cast Removal in Idiopathic Congenital Talipes Equinovarus: A Study on Modified Ponseti Technique using an Interposed Polythene Sheet July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus
July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus January 1, 2026 Management of Relapsed, Residual, and Resistant Idiopathic Congenital Talipes Equinovarus
January 1, 2026 Management of Relapsed, Residual, and Resistant Idiopathic Congenital Talipes Equinovarus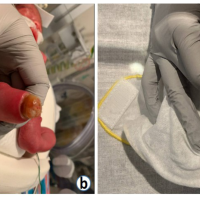 September 1, 2024 Club Foot with Contralateral Congenital Amniotic Band Syndrome Amputation Successfully Treated with Ponseti Method: Case Report
September 1, 2024 Club Foot with Contralateral Congenital Amniotic Band Syndrome Amputation Successfully Treated with Ponseti Method: Case Report