
This case underscores the importance of including rare musculoskeletal tumors in the differential diagnosis of atypical orthopaedic lesions and demonstrates that accurate imaging, histopathological confirmation, and appropriate surgical management are essential for achieving optimal oncologic and functional outcomes.
Dr. Behic Celik, Department of Orthopedics and Traumatology, Yeditepe University Hospital, Icerenkoy, 34752 Atasehir/Istanbul, Istanbul, Turkey. E-mail: behic13@gmail.com
Introduction: Malignant peripheral nerve sheath tumors (MPNST) are uncommon soft-tissue sarcomas that typically arise in proximal segments of the extremities or pelvis. Their management requires precise biopsy planning, careful surgical assessment, and coordinated multidisciplinary care. Tumors involving multiple longitudinal levels of the leg are rare and pose significant challenges for limb salvage.
Case Report: We report the case of a 79-year-old male presenting with a rapidly progressive mass extending along the posterior cruris, in the setting of a prior hip hemiarthroplasty and a revision total knee arthroplasty with long femoral and tibial stems. Magnetic resonance imaging demonstrated two heterogeneous solid masses in the posterolateral proximal right cruris and biopsy revealed a high-grade MPNST (Fédération Nationale des Centres de Lutte Contre le Cancer grade 3). The tumor board concluded that limb-sparing resection was unsafe due to tumor extent, limited soft-tissue envelope, and anticipated difficulty achieving durable wound closure. The presence of existing long-stem implants further complicated determination of a safe osteotomy level. Above-knee amputation was therefore selected as the most reliable method for achieving oncologic control while minimizing post-operative complications.
Discussion/Results: The amputation was performed with fluoroscopy-guided planning of the osteotomy level to avoid stem interference, followed by myoplasty and myodesis for stable stump reconstruction. Histopathology confirmed a high-grade MPNST with diffuse S100 and SOX10 positivity, extensive necrosis, high mitotic activity, and a Ki-67 index of 50%.
Conclusion: This case illustrates the critical importance of methodical biopsy planning and multidisciplinary coordination in managing sarcomas of the lower extremity. The unusual longitudinal distribution of the tumor, combined with the constraints imposed by pre-existing long-stem implants, made limb salvage infeasible. Individualized surgical planning, incorporating both oncologic and reconstructive considerations, is essential when managing complex MPNSTs in reconstructively compromised limbs.
Keywords: Malignant peripheral nerve sheath tumor, limb salvage, above-knee amputation, lower extremity sarcoma, revision arthroplasty implants.
Malignant peripheral nerve sheath tumor (MPNST) represents the sixth most common subtype of soft-tissue sarcomas, accounting for roughly 5–10% of all cases [1,2]. Although its precise histogenetic origin is still uncertain, most tumors arise in association with peripheral nerves and are believed to derive from neural crest–related cells [3]. Approximately half of all MPNSTs occur sporadically, while the remaining 50% develop in individuals with neurofibromatosis type 1 [4]. Clinically, MPNST typically occurs in a manner similar to other soft-tissue sarcomas, often presenting as a progressively enlarging mass over months or years. These tumors most frequently originate near major nerve bundles of the extremities and pelvis—such as the sciatic nerve, brachial plexus, and sacral plexus—resulting most commonly in the proximal upper and lower limbs [5]. Common symptoms include pain, paresthesia, and may include various neurologic deficits. For localized high-grade MPNST, the current standard of care involves surgical resection followed by adjuvant radiotherapy. Despite aggressive treatment, local recurrence occurs in approximately 40–65% of patients, and metastatic spread develops in 30–60%, most commonly to the lungs [6]. Overall, MPNST carries a poor prognosis, with reported 5-year survival rates ranging from 20% to 50% and mortality reaching up to 75% in high-grade cases [7].
A 79-year-old male with no known comorbidities presented with a 2-year history of a progressive soft-tissue mass located along the posterior aspect of the right leg, extending from the distal popliteal region to the mid-cruris. A previous incision scar was noted over the lesion, reportedly from an earlier biopsy, although neither the patient nor his relatives could provide reliable information regarding the prior procedure. The initial biopsy performed at an outside center had been reported as incomplete. The patient had undergone a revision total knee arthroplasty with long femoral and tibial stems at another institution approximately 2 years earlier. He reported that the mass had increased significantly in size over the past year. Initial radiographs demonstrated soft-tissue swelling without clearly identifiable calcifications. The patient was referred for anesthesia evaluation for a repeat biopsy. Pre-operative magnetic resonance imaging demonstrated two heterogenous solid masses in the posterolateral proximal right cruris: A larger lesion measuring approximately 90 × 77 × 105 mm with central cystic/necrotic, non-enhancing areas, and a smaller adjacent caudal lesion measuring approximately 40 × 38 × 42 mm (Fig. 1). Core biopsy results were consistent with a high-grade MPNST. Clinically, he reported progressive pain, decreased appetite, and weight loss. positron emission tomography-computed tomography (PET-CT) was recommended for staging.

Figure 1: Pre-operative evaluation of the right cruris showing lateral (a) and posterior (b) clinical photographs, coronal magnetic resonance imaging (MRI) demonstrating both lesions (c), and sagittal MRI showing their longitudinal extent (d).
The case was discussed in a multidisciplinary tumor board, where palliative radiotherapy was initially considered. Following PET-CT evaluation, the tumor board concluded that limb-sparing surgery would not be feasible due to the large tumor size, aggressive pathology, and expected soft-tissue deficiency in a limb previously reconstructed with long-stem implants. An above-knee amputation was recommended. The patient and his family were informed in detail about the planned procedure, including the possibility of a high-risk post-operative course and the need for intensive care monitoring. He was subsequently referred to anesthesia for pre-operative assessment.
Surgical procedure
An above-knee amputation was planned after multidisciplinary evaluation due to the size and extent of the high-grade MPNST and the anticipated inability to achieve durable soft-tissue coverage with limb-sparing options. Pre-operative imaging confirmed the presence of a hip hemiarthroplasty stem and a long revision femoral stem from the patient’s prior total knee arthroplasty. Pre-operative X-ray demonstrated that the tibial revision stem extended approximately 170 mm proximal to the knee joint line, while the tip of the femoral stem was located roughly 170 mm distal to the greater trochanter. These measurements confirmed that both implants occupied substantial portions of the femur and tibia. The planned transfemoral amputation level was positioned approximately 1 cm proximal to the proximal end of the tibial stem, thereby avoiding stem interference while preserving an adequate residual femoral length for prosthetic fitting (Fig. 2).

Figure 2: Pre-operative radiographs showing the hip anteroposterior (AP) view with the hemiarthroplasty stem (a) and the knee AP view with the revision type long femoral and tibial stems (b), including measured distances from the greater trochanter and knee joint line to the respective stem tips.
A fish-mouth configuration was selected to optimize stump contour and closure. Following standard preparation, an anterior incision was created and extended circumferentially to form anterior and posterior flaps. Dissection proceeded through the subcutaneous tissues to the medial aspect of the thigh, where the adductor canal was identified. The femoral artery and vein were isolated and ligated proximally and distally. The saphenous nerve was divided sharply at a proximal level. Dissection continued posteriorly to expose the sciatic nerve, which was transected in a single sharp cut at a proximal location. The deep femoral vessels were identified and ligated in a similar fashion. After completing circumferential mobilization, the femur was osteotomized at the pre-determined mid-femoral level using a Gigli saw, safely distal to both pre-existing femoral stems. The bone edges were smoothed. The stump was reconstructed using adductor myoplasty secured through drill holes in the femur. This was followed by myodesis of the anterior and posterior muscle compartments to provide stable muscular coverage. The anterior and posterior flaps were approximated with fascial sutures, and the wound was closed in a layered, tension-free manner. A single closed-suction drain was placed, and the stump was dressed and compressed with an elastic bandage. The amputated specimen was submitted for pathological examination.
Pathology and histology
Final pathology from multiple incisional and Tru-cut biopsies of the proximal and distal crural masses demonstrated a high-grade MPNST. All specimens showed a densely cellular spindle-cell neoplasm composed of intersecting fascicles of atypical, elongated, and occasionally serpentine cells with coarse chromatin and scant cytoplasm. The tumor exhibited a mixed diffuse and nodular growth pattern with alternating hypercellular and hypocellular areas. Geographic tumor necrosis was prominent, involving approximately 50% of the sampled tissue. Frequent mitotic figures (10–19 mitoses/10 high-power fields) were identified. Multinucleated tumor cell groups were also present. According to the Fédération Nationale des Centres de Lutte Contre le Cancer system, the tumor demonstrated a differentiation score of 3, mitotic score of 2, and necrosis score of 2, corresponding to an overall grade 3 sarcoma (a total score of 7). Immunohistochemically, the tumor showed strong diffuse positivity for S100 and SOX10, supporting neural crest–related differentiation. Additional positive markers included CD34, CD56, CD99, collagen IV, FXIIIa, and focal epithelial membrane antigen. The Ki-67 proliferation index was markedly elevated at approximately 50%, and p53 expression was detected in approximately 70% of tumor nuclei (Fig. 3). Markers for skeletal muscle differentiation (actin, caldesmon), mesothelial differentiation (calretinin), cytokeratin (pan-CK), and others were negative.

Figure 3: Macroscopic appearance of the tumor, measuring 19 × 11 × 7 cm (a), macroscopic view of the above-knee amputation specimen, measuring 66 × 17 × 13 cm (b), malignant mesenchymal tumor composed of spindle cells arranged in a fascicular pattern, with irregular bundles and short storiform areas (Hematoxylin and Eosin, ×15) (c), Ki-67 immunostaining demonstrating strong nuclear positivity in tumor cells, with a proliferation index of 50% (Ki-67, ×40) (d), diffuse nuclear and cytoplasmic positivity in tumor cells (S-100, ×10) (e), diffuse nuclear positivity in tumor cells with SOX10 staining (SOX10, ×10) (f).
Taken together, the morphologic features and immunohistochemical profile confirmed the diagnosis of high-grade MPNST according to the 2020 World Health Organization classification.
MPNSTs typically arise in the proximal segments of the extremities and pelvis, often in association with major nerve trunks, such as the sciatic or brachial plexus [8]. In contrast, the present case demonstrated an uncommon pattern of multifocal involvement along the cruris, with lesions identified both proximally and distally. This longitudinal distribution significantly complicated attempts at limb-sparing resection. Standard treatment for high-grade MPNST includes wide excision with negative margins followed by adjuvant radiotherapy, with chemotherapy considered in selected cases [9]. However, in this patient, radical resection posed substantial risks: The expected inability to achieve durable wound closure, the limited soft-tissue envelope, and the consensus opinion of the orthopedic, plastic surgery, and oncology teams led to above-knee amputation as the safer option. The presence of a hip hemiarthroplasty stem and a long-stem revision femoral component introduced additional challenges, as the osteotomy level had to be carefully selected to avoid violating existing implants while still achieving oncologic control. This constraint also influenced the planning of soft-tissue coverage and stump stability. Furthermore, even if limb-sparing excision had been attempted, the tibial revision stem and prior surgical field would have created a high-risk environment for post-operative infection, potentially compromising both oncologic and functional outcomes [10]. Taken together, these factors supported amputation as the most appropriate management strategy to ensure reliable disease control and minimize complications in this anatomically complex and surgically constrained limb [11].
This case highlights the importance of a methodical and multidisciplinary approach in the evaluation and management of MPNSTs and other sarcoma-like malignancies. Careful planning of biopsy location and technique is essential to avoid compromising future surgical options and to ensure accurate diagnosis. Similarly, early involvement of orthopedic oncology, plastic surgery, radiology, and medical oncology teams is critical for defining the safest and most effective treatment pathway. The unusual longitudinal distribution of the tumor throughout the cruris, combined with the presence of multiple long-stem implants, created unique challenges in determining both the level of resection and the feasibility of limb salvage. These factors ultimately justified above-knee amputation as the most reliable means of achieving disease control and secure wound closure. This case underscores the need to individualize treatment strategies for complex sarcomas, especially when anatomical, reconstructive, or implant-related limitations make standard excision approaches unsafe.
Complex MPNSTs in limbs containing long-stem implants require meticulous planning to determine safe biopsy routes, resection margins, and amputation levels. In select patients, amputation may offer a safer and more reliable outcome than limb salvage.
References
- 1. Eilber FC, Brennan MF, Eilber FR, Dry SM, Singer S, Kattan MW. Validation of the postoperative nomogram for 12-year sarcoma-specific mortality. Cancer 2004;101:2270-5. [Google Scholar] [PubMed]
- 2. Grobmyer SR, Reith JD, Shahlaee A, Bush CH, Hochwald SN. Malignant peripheral nerve sheath tumor: Molecular pathogenesis and current management considerations. J Surg Oncol 2008;97:340-9. [Google Scholar] [PubMed]
- 3. Lin CT, Huang TW, Nieh S, Lee SC. Treatment of a malignant peripheral nerve sheath tumor. Onkologie 2009;32:503-5. [Google Scholar] [PubMed]
- 4. Bradtmöller M, Hartmann C, Zietsch J, Jäschke S, Mautner VF, Kurtz A, et al. Impaired PTEN expression in human malignant peripheral nerve sheath tumours. PLoS One 2012;7:e47595. [Google Scholar] [PubMed]
- 5. Anghileri M, Miceli R, Fiore M, Mariani L, Ferrari A, Mussi C, et al. Malignant peripheral nerve sheath tumors: Prognostic factors and survival in a series of patients treated at a single institution. Cancer 2006;107:1065-74. [Google Scholar] [PubMed]
- 6. Goertz O, Langer S, Uthoff D, Ring A, Stricker I, Tannapfel A, et al. Diagnosis, treatment and survival of 65 patients with malignant peripheral nerve sheath tumors. Anticancer Res 2014;34:777-83. [Google Scholar] [PubMed]
- 7. Carli M, Ferrari A, Mattke A, Zanetti I, Casanova M, Bisogno G, et al. Pediatric malignant peripheral nerve sheath tumor: The Italian and German soft tissue sarcoma cooperative group. J Clin Oncol 2005;23:8422-30. [Google Scholar] [PubMed]
- 8. Knight SW, Knight TE, Santiago T, Murphy AJ, Abdelhafeez AH. Malignant peripheral nerve sheath tumors-a comprehensive review of pathophysiology, diagnosis, and multidisciplinary management. Children (Basel) 2022;9:38. [Google Scholar] [PubMed]
- 9. Yao C, Zhou H, Dong Y, Alhaskawi A, Hasan Abdullah Ezzi S, Wang Z, et al. Malignant peripheral nerve sheath tumors: Latest concepts in disease pathogenesis and clinical management. Cancers (Basel) 2023;15:1077. [Google Scholar] [PubMed]
- 10. Seres R, Hameed H, McCabe MG, Russell D, Lee AT. The multimodality management of malignant peripheral nerve sheath tumours. Cancers (Basel) 2024;16:3266. [Google Scholar] [PubMed]
- 11. Baysal Ö, Sağlam F, Sofulu Ö, Yiğit O, Şirin E, Erol B. Indications of amputation after limb-salvage surgery of patients with extremity-located bone and soft-tissue sarcomas: A retrospective clinical study. Acta Orthop Traumatol Turc 2021;55:154-8. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Managing Hip Arthritis in an Above-Knee Amputee: A Case Report of Total Hip Arthroplasty with Surgical Technique and Rehabilitation Considerations
March 1, 2026 Managing Hip Arthritis in an Above-Knee Amputee: A Case Report of Total Hip Arthroplasty with Surgical Technique and Rehabilitation Considerations March 1, 2026 Primary Intraosseous Malignant Nerve Sheath Tumor of Humerus Presenting With Pathological Fracture: A Rare Case Report With Review of Literature
March 1, 2026 Primary Intraosseous Malignant Nerve Sheath Tumor of Humerus Presenting With Pathological Fracture: A Rare Case Report With Review of Literature February 1, 2025 Limb Salvage and Reconstruction of a Complex Upper Extremity Injury: A Case Report
February 1, 2025 Limb Salvage and Reconstruction of a Complex Upper Extremity Injury: A Case Report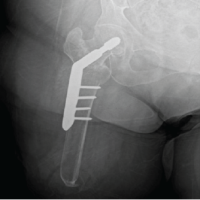 November 1, 2024 Intertrochanteric Fracture Fixation Using a Traction Table in a Patient with Ipsilateral Above-knee Amputation – A Case Report and Review of Reduction Techniques
November 1, 2024 Intertrochanteric Fracture Fixation Using a Traction Table in a Patient with Ipsilateral Above-knee Amputation – A Case Report and Review of Reduction Techniques