
Achieving early anatomical reduction and stable fixation is the most critical determinant of outcome in paediatric femoral neck fractures, as fracture characteristics and reduction quality have greater impact on prognosis than implant choice.
Dr. Anirudh Dwajan, Department of Orthopaedics, All India Institute of Medical Sciences, Bilaspur, Himachal Pradesh, India. E-mail: anirudhdwajan@gmail.com
Introduction: Femoral neck fractures in children are rare injuries associated with a high risk of complications, particularly avascular necrosis (AVN) of the femoral head. The purpose of this retrospective study was to evaluate the functional and radiological outcomes of pediatric femoral neck fractures treated surgically and to assess factors influencing clinical outcomes.
Materials and Methods: This retrospective, single-center study included 18 children (<16 years) with isolated unilateral femoral neck fractures who were treated surgically between January 2021 and September 2022. Fractures were classified according to the Delbet system. Internal fixation was performed using cannulated cancellous screws, Moore’s pins, or a combination of both. Operative time, blood loss, and fluoroscopy exposure were recorded from operative records. Patients had a minimum follow-up of 1 year. Functional outcomes were assessed using Ratliff’s criteria, and radiological evaluation included fracture union, loss of neck–shaft angle, and development of AVN. Given the rarity of the injury, the study was designed as a retrospective single-center observational case series.
Results: Union was achieved in all but three cases. AVN of the femoral head was observed in three patients, predominantly in Delbet type I and II fractures. Functional outcomes tended to be more favorable in less proximal fracture types. No statistically significant association was found between implant type and functional outcome.
Conclusion: Outcomes following internal fixation of pediatric femoral neck fractures appeared to be more closely related to fracture morphology and quality of reduction than to implant choice. These findings suggest that patient and fracture characteristics may play a greater role in determining outcomes than the fixation method used.
Keywords: Femoral neck fractures, pediatric orthopedics, internal fixation, avascular necrosis, hip fractures, treatment outcome.
Fractures of the femoral neck in the pediatric age group are uncommon injuries and are associated with a risk of various long-term complications. The reported incidence of these fractures in children ranges from 0.3% to 0.6% annually [1,2,3]. The most commonly affected age group is between 10 and 13 years [4]. Males are affected more commonly than females [4]. High-energy trauma, particularly road traffic accidents, represents the most frequent mechanism of injury; however, falls from height have also been implicated [5]. Approximately half of affected patients experience some form of long-term complication [2,6,7,8,9]. These adverse outcomes are largely attributable to the tenuous blood supply to the femoral head and the unique osseous anatomy in children. Recent comprehensive reviews have emphasized that pediatric femoral neck fracture management should be tailored to the distinctive anatomic and radiographic features of the immature proximal femur, with emphasis on fracture classification, reduction quality, and fixation strategy to minimize complications [10]. Consequently, a thorough understanding of fracture mechanics, appropriate management options, post-operative care, and potential complications is essential. Despite multiple fixation options being described, there remains limited high-quality evidence evaluating clinical and radiological outcomes in pediatric femoral neck fractures, particularly in resource-constrained settings.
This retrospective single-center study included 18 patients aged <16 years with isolated unilateral femoral neck fractures diagnosed on plain radiographs or computed tomography who underwent surgical intervention. The study period extended from January 2021 to September 2022, and all procedures were performed by the same surgical team. All patients underwent pre-anesthetic evaluation before surgery and had a minimum follow-up of 1 year. All cases were operated on between 12 and 36 h after injury, following referral from primary or secondary care centers. The choice of fixation method was based on fracture type, patient age, and surgeon discretion, taking implant availability into account. Cannulated cancellous screw (CCS) fixation was preferentially used in patients older than 13 years and generally avoided in more proximal fractures. In patients younger than 13 years, either smooth pins or a combination of CCS and smooth pins was used. Due to the rarity of pediatric femoral neck fractures, no formal sample size calculation was performed. Of the 18 patients, 11 were male, and 7 were female. Ten injuries resulted from road traffic accidents, seven from falls from height, and one from direct impact due to a heavy object. Fractures were classified according to the Delbet system. Three cases were Delbet type I, eleven were type II, and four were type III.
Closed reduction under fluoroscopy was successfully attempted in all cases using either the Whitman or Leadbetter technique. Anatomical reduction with neutral or positive medial cortical alignment was aimed for. The neck–shaft angle of the contralateral side was used as a guide, along with Lowell’s “S” curves in both anteroposterior and lateral views. Cortical translation was maintained at <2 mm, and malrotation was avoided. When anatomical reduction could not be achieved, the quality of reduction was ensured to be at least “fair” as defined by Shrader et al. [8,11]. Internal fixation was performed in all cases using CCS, Austin-Moore’s pins, or a combination of both. Needle aspiration of the intracapsular hematoma was not performed in any case. Functional outcomes were assessed using Ratliff’s criteria based on clinical records and follow-up documentation [12,13]. Patients were divided into three groups, namely Groups A, B, and C. Group A consisted of patients treated with CCS alone, Group B included patients treated with Moore’s pins, and Group C included patients in whom both of these implants were used in combination. Group A comprised seven patients, Group B comprised six patients, and Group C comprised five patients. Patients with associated injuries hampering the usual post-operative rehabilitation protocol were excluded from analysis. Patients with pre-existing major systemic disorders or those having contraindications to surgical intervention were also excluded. The post-operative rehabilitation regime was adjusted based on the fixation technique used and the quality of fixation. All fixations were performed more than 12 h after injury, as most cases were referred from primary or secondary health care services. Operative time was calculated from the time of incision to the time of final closure. Blood loss was estimated by adding the blood collected by suction and that soaked by gauze pieces. One fully soaked gauze piece was taken as 50 mL of blood loss. Fluoroscopy exposure was assessed by counting the number of C-Arm shots.
Statistical Analysis
Categorical variables were summarized using frequencies and percentages, and continuous variables were expressed as mean values with ranges. Statistical analysis was performed using IBM SPSS Statistics software (IBM Corp., Armonk, NY, USA). Associations between categorical variables, including implant type, fracture type, age group, and functional outcomes according to Ratliff’s criteria, were analyzed using the Chi-square test. A P-value of <0.05 was considered statistically significant.
Techniques used
Compliant patients aged 10 years or more were mobilized to non-weight bearing for 2 weeks, followed by toe-touch weight bearing for the 3rd week and partial weight-bearing for weeks 4–6. Only compliant patients were included in the analysis. Children aged <10 years and non-compliant patients were immobilized in a hip spica cast for 8 weeks, followed by gradual range-of-motion exercises and progressive weight bearing. Our rehabilitation protocol was identical in all three study groups and was in accordance with contemporary protocols described in the literature. After attempting closed reduction under general anesthesia using the previously described techniques, patients were positioned supine, standard aseptic precautions were followed, and an incision was made from the base of the greater trochanter extending approximately 6 cm distally. The tensor fascia lata was incised, and the vastus lateralis was split using blunt dissection. The periosteum was preserved, and either 4-mm CCS, Moore’s pins, or a combination of both were inserted along the femoral neck axis in either parallel or divergent configuration under C-arm guidance. The screws were introduced using guidewires and drill bits of appropriate size. Care was taken to keep each screw at least 5 mm short of the articular surface in both anteroposterior and lateral views. On the lateral view, screws were positioned centrally within the femoral neck, whereas on the anteroposterior view, one screw was placed superiorly and the other inferiorly within the femoral neck (Fig. 1).
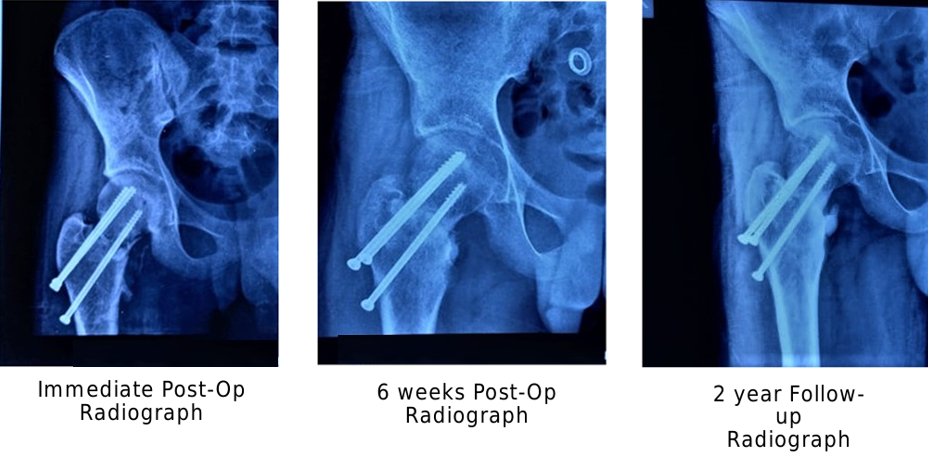
Figure 1: Anteroposterior radiographs of a pediatric femoral neck fracture treated with cannulated cancellous screw fixation showing the immediate post-operative appearance, progression of fracture healing at 6 weeks, and maintained alignment with union.
In cases where Moore’s pins were used, an incision was made similarly to that in the CCS group, and the periosteum was not elevated from the bone. Three Austin–Moore pins with a diameter of 3 mm were inserted in an inverted triangle configuration under C-arm guidance (Fig. 2). All pins were kept at least 5 mm short of the articular cartilage.
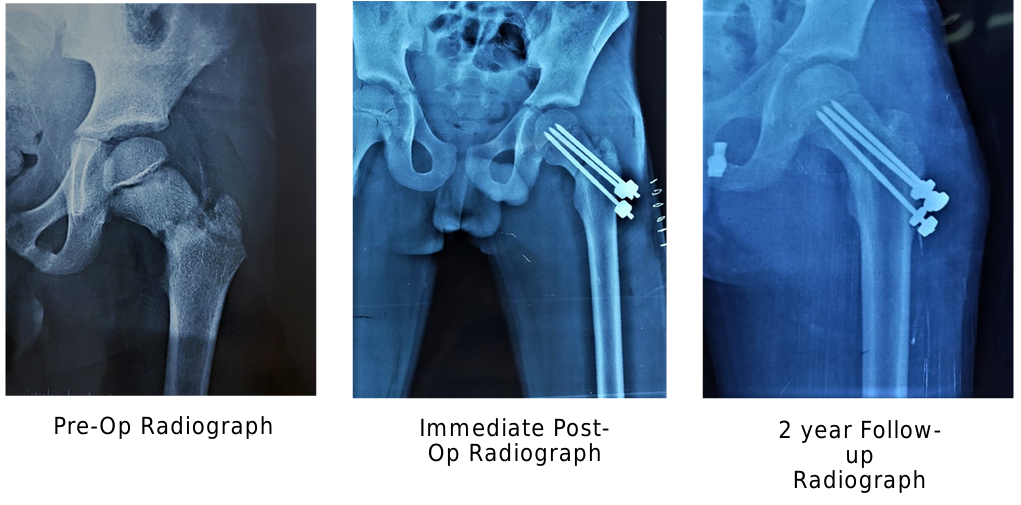
Figure 2: Anteroposterior radiographs of a pediatric femoral neck fracture demonstrating the pre-operative appearance, immediate post-operative fixation with smooth (Moore’s) pins, and maintained alignment with fracture union at 2-year follow-up.
In cases where a combination of two implants was used, a 3-mm Moore’s pin was first inserted into the inferior part of the femoral neck, with the tip positioned in the inferomedial compartment of the femoral head and maintained at least 5 mm from the articular surface in both views. On the lateral view, the pin was positioned centrally within both the femoral neck and head. This was followed by insertion of a 4-mm CCS superior to the Moore’s pin in a parallel direction using a guidewire (Fig. 3). The screw functioned as an anti-rotation device. The advantage of using a CCS instead of an additional Moore’s pin was its ability to achieve intraoperative compression at the fracture site while minimizing post-operative soft-tissue irritation.
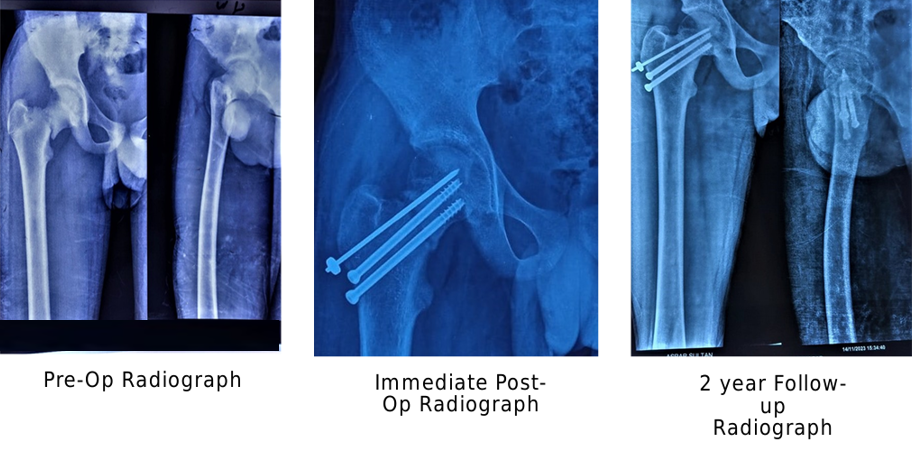
Figure 3: Anteroposterior radiographs of a pediatric femoral neck fracture showing the pre-operative fracture pattern, immediate post-operative fixation using a combination of cannulated cancellous screws and smooth pins, and maintained alignment with union at 2-year follow-up.
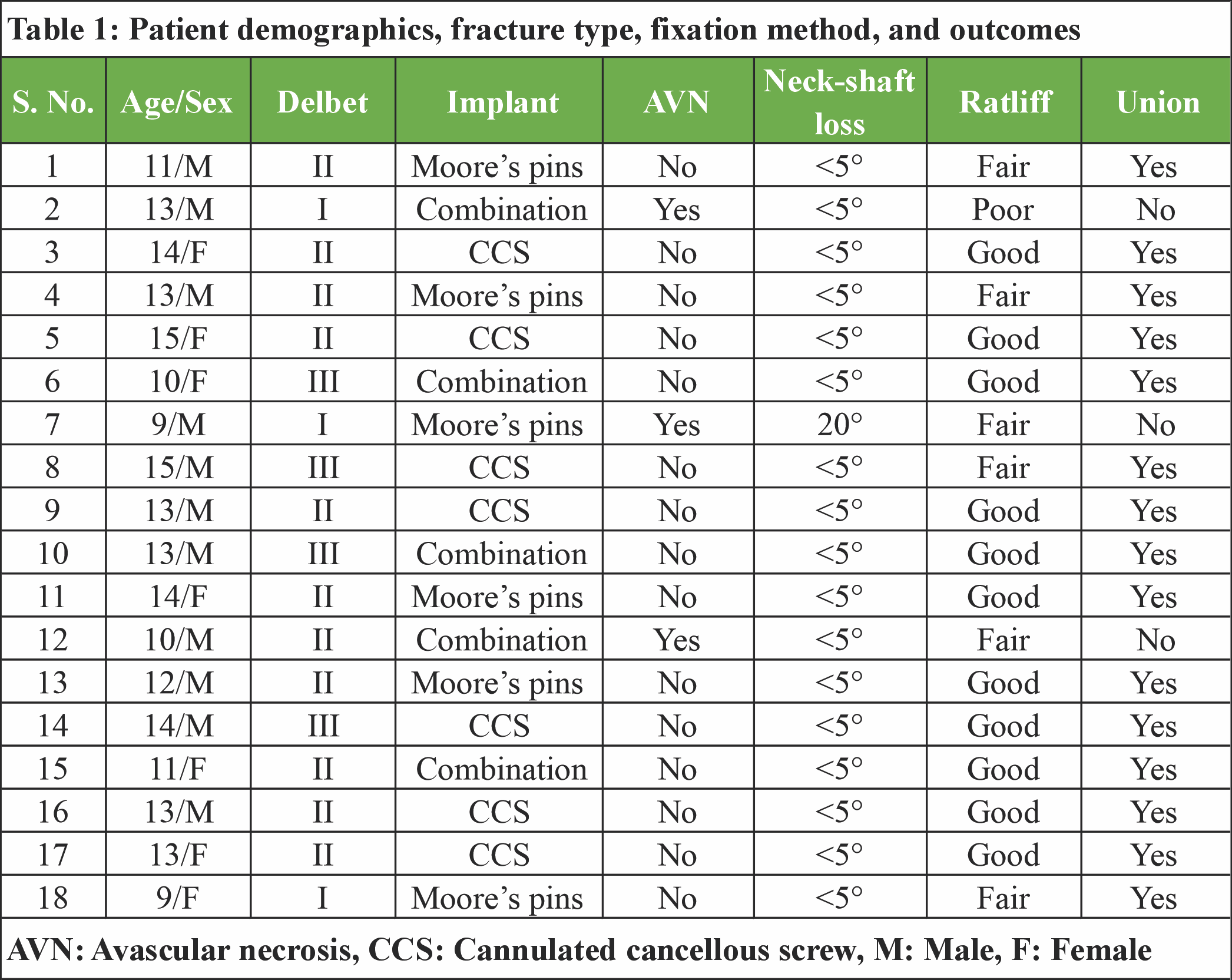
Patient demographics, fracture characteristics, fixation methods, and outcomes for all 18 cases are summarized in Table 1. Three patients developed avascular necrosis (AVN), all of whom had Delbet type I or II fractures. Non-union was observed in three cases. The majority of patients achieved good functional outcomes according to Ratliff’s criteria, with fair or poor results occurring predominantly in patients with AVN or non-union.
Overall, 11 patients achieved good functional outcomes, 6 had fair outcomes, and 1 had a poor outcome according to Ratliff’s criteria. Fair and poor outcomes were predominantly observed in patients who developed AVN or non-union.
Patients were categorized into three groups: The CCS group (Group A), the Moore’s pins group (Group B), and the combined fixation group (Group C). The number of patients in Groups A, B, and C was seven, six, and five, respectively. The mean age was 13.85 years in Group A, 11.33 years in Group B, and 11.40 years in Group C. Group A comprised four males and three females, Group B four males and two females, and Group C three males and two females. Of the 18 patients, 10 had right-sided, and 8 had left-sided fractures.
The mean operative time was 37.86 min in Group A, 51.66 min in Group B, and 40.00 min in Group C. The mean blood loss was 101.43 mL in Group A, 157.50 mL in Group B, and 132.00 mL in Group C. The mean fluoroscopy exposure was 15.28 C-arm shots in Group A, 24.83 shots in Group B, and 21.40 shots in Group C. AVN occurred in one patient in Group B and two patients in Group C, whereas no cases were observed in Group A. Intra-operative parameters, including operative time, blood loss, and fluoroscopy exposure, differed across the three fixation groups (Fig. 4). No statistically significant association was observed between implant type and functional outcome.

Figure 4: Bar chart showing comparison of intra-operative parameters – operative time, estimated blood loss, and number of C-arm fluoroscopy shots – among the three fixation groups (Group A: Cannulated cancellous screws, Group B: Moore’s pins, and Group C: Combination fixation).
Functional outcomes according to Ratliff’s grading system at final follow-up were good in six cases and fair in one case in Group A. In Group B, four patients had fair outcomes, and two had good outcomes, whereas in Group C, three patients had good outcomes, one had a fair outcome, and one had a poor outcome. A higher proportion of good outcomes was observed in Group A, whereas fair and poor outcomes were more frequent in Groups B and C. When functional outcomes were analyzed according to age, one patient aged ≤10 years had a good outcome, and three had fair outcomes, with no poor results observed in this age group. Among patients aged >10 years, 10 had good outcomes, three had fair outcomes, and one had a poor outcome. Statistical analysis demonstrated no significant association between age and Ratliff functional grade (χ2 = 4.062, P = 0.131). Analysis according to fracture type showed that among Delbet type I fractures, no patient achieved a good outcome, two had fair outcomes, and one had a poor outcome. In Delbet type II fractures, eight patients had good outcomes, and three had fair outcomes, whereas in Delbet type III fractures, three patients had good outcomes, and one had a fair outcome. There was no statistically significant association between fracture type and functional outcome (χ2 = 8.407, P = 0.078).
With respect to implant type, six patients in the CCS group had good outcomes, and one had a fair outcome. In the Moore’s pins group, two patients had good outcomes, and four had fair outcomes, whereas in the combination group, three patients had good outcomes, one had a fair outcome, and one had a poor outcome. No statistically significant association was observed between implant type and functional outcome (χ2 = 7.081, P = 0.132). The mean post-operative limb-length discrepancy (LLD) at final follow-up was <1 cm. Shortening was greatest in Group A (mean 0.8 cm) and lowest in Group B (mean 0.5 cm). Three patients developed post-operative surgical site infections. Two patients presented with erythema and mild serous discharge that resolved within 1 week with oral antibiotics. One patient developed a purulent discharge requiring culture-directed intravenous antibiotics, which resolved within 2 weeks. No patient developed early implant failure, varus collapse, femoral head cut-through, or gross malunion. Post-operative pain was the most common complaint but was successfully managed with oral analgesics, and all patients returned to activities of daily living by final follow-up. Three cases of AVN were observed – two in Delbet type I fractures and one in a Delbet type II fracture. One case occurred in Group B and two in Group C. All cases were confirmed by magnetic resonance imaging. Coxa vara developed in one patient in Group B, with a 20° reduction in neck–shaft angle over 1 year. In all other patients, loss of neck–shaft angle at final follow-up was <5°.
Fractures of the femoral neck in children are rare injuries and occur more than 100 times more frequently in adults than in the pediatric population [13]. Several important differences exist between adult and pediatric femoral neck fractures. The first relates to the mechanism of injury. In children, the proximal femur, except for the physis, is particularly strong and requires high-energy trauma to fracture, whereas in elderly patients, osteoporotic bone may fracture even after trivial trauma. This observation was reflected in the present study, as most pediatric fractures resulted from high-energy mechanisms. The second major difference concerns the blood supply. In adults, intra-osseous vessels freely supply the femoral head, whereas in children, the physis acts as a barrier to vascular channels, increasing the risk of vascular disruption and subsequent AVN. There is substantial evidence indicating a strong correlation between clinical and radiological outcomes and the risk of late-onset AVN [13,14]. Several factors have been implicated in the development of AVN, including fracture type, timing of fixation, intracapsular decompression, quality of reduction, and post-operative immobilization [15,16,17,18,19]. More proximal fracture patterns are associated with a higher risk of AVN [20,21], with reported incidences ranging from 0% to 92%. The risk also increases with age and is highest in adolescents [21]. Contemporary clinical studies have also found that factors such as the degree of initial fracture displacement and prolonged time from injury to surgery are associated with higher rates of AVN of the femoral head, supporting the emphasis on early and accurate reduction [22]. These observations are consistent with the present study, in which AVN occurred predominantly in patients with more proximal fracture patterns. Surgery-related infection rates have been reported between 1% and 2% in contemporary literature [23]. The proximal femoral physis contributes approximately 15% of total limb growth at a rate of about 3 mm/year [24]; therefore, concerns regarding physeal arrest and subsequent LLD are justified. Smooth pins are thought to reduce the risk of physeal damage compared with cancellous screws [19,25], whereas CCS provide greater mechanical stability. The risks of crossing the physis must be balanced against the consequences of unstable fixation, such as non-union, coxa vara, and AVN. Delbet type I and high type II fractures often require transphyseal fixation due to limited metaphyseal bone stock. The objective of this study was to evaluate functional and radiological outcomes of surgically treated pediatric femoral neck fractures and to assess factors associated with complications such as AVN, non-union, and coxa vara. Operative time, fluoroscopy exposure, blood loss, and post-operative complications were also analyzed across fixation groups.
Clinical decision-making considerations
The findings of the present study suggest that successful outcomes in pediatric femoral neck fractures are more closely associated with fracture morphology, patient age, and the quality of reduction than with implant choice alone. In younger children with proximal fractures and substantial remaining growth potential, smooth pins have been advocated in the literature to minimize physeal injury, whereas in older children and adolescents with more distal fracture patterns, CCS have been reported to provide reliable stability. In selected cases, a combination of fixation methods has been described as a potential option to balance stability and physeal preservation. The limitations of the present study include a small sample size, a single-center design, and a relatively short mean follow-up period. However, as radiological evidence of AVN of the femoral head can typically be detected within 1 year following injury [13], the duration of follow-up was sufficient to identify this complication. Regardless of the fixation method used, achieving anatomical reduction and stable fixation was prioritized in all cases. At final follow-up, all patients and their guardians reported satisfaction with the outcomes of surgical treatment.
Ethical Approval
This retrospective study used anonymized clinical data collected during routine patient care. Formal institutional ethics approval was not required according to institutional policy for retrospective observational studies. The study was conducted in accordance with accepted ethical standards, and informed consent was obtained from patients’ guardians.
Pediatric femoral neck fractures remain challenging injuries because of their rarity and the risk of serious complications such as AVN and non-union. In this retrospective single-center case series, functional and radiological outcomes were more closely associated with fracture morphology, patient age, and the quality of reduction than with the type of implant used for fixation. No statistically significant association was identified between implant choice and functional outcome. CCS, smooth pins, and combination constructs all resulted in acceptable outcomes when stable fixation and satisfactory reduction were achieved. These findings suggest that implant selection should be individualized based on fracture characteristics and patient factors rather than a fixed implant protocol. Larger multicenter prospective studies are required to further clarify the influence of fixation strategy on long-term outcomes in pediatric femoral neck fractures.
Early anatomical reduction and stable internal fixation are the most important determinants of outcome in pediatric femoral neck fractures. Fracture morphology, patient age, and quality of reduction have a greater influence on functional outcome and risk of avascular necrosis than the choice of implant, emphasizing the importance of achieving and maintaining optimal reduction regardless of fixation method.
References
- 1. Davison BL, Weinstein SL. Hip fractures in children: A long-term follow-up study. J Pediatr Orthop 1992;12:355-8. [Google Scholar] [PubMed]
- 2. Mirdad T. Fractures of the neck of femur in children: An experience at the Aseer central hospital, Abha, Saudi Arabia. Injury 2002;33:823-7. [Google Scholar] [PubMed]
- 3. Bimmel R, Bakker A, Bosma B, Michielsen J. Paediatric hip fractures: A systematic review of incidence, treatment options and complications. Acta Orthop Belg 2010;76:7-13. [Google Scholar] [PubMed]
- 4. Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC. Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-20. [Google Scholar] [PubMed]
- 5. Varshney MK, Kumar A, Khan SA, Rastogi S. Functional and radiological outcome after delayed fixation of femoral neck fractures in pediatric patients. J Orthop Traumatol 2009;10:211-6. [Google Scholar] [PubMed]
- 6. Yeranosian M, Horneff JG, Baldwin K, Hosalkar HS. Factors affecting the outcome of fractures of the femoral neck in children and adolescents: A systematic review. Bone Joint J 2013;95-B:135-42. [Google Scholar] [PubMed]
- 7. Pape HC, Krettek C, Friedrich A, Pohlemann T, Simon R, Tscherne H. Long-term outcome in children with fractures of the proximal femur after high-energy trauma. J Trauma 1999;46:58-64. [Google Scholar] [PubMed]
- 8. Shrader MW, Jacofsky DJ, Stans AA, Shaughnessy WJ, Haidukewych GJ. Femoral neck fractures in pediatric patients: 30 years experience at a level 1 trauma center. Clin Orthop Relat Res 2007;454:169-73. [Google Scholar] [PubMed]
- 9. Patterson JT, Tangtiphaiboontana J, Pandya NK. Management of pediatric femoral neck fracture. J Am Acad Orthop Surg 2018;26:411-9. [Google Scholar] [PubMed]
- 10. Wang W, Canavese F, Xiong Z, Tang S, Chen S, He S. Management of pediatric femoral neck fractures from classification to surgery: A review of indications based on anatomic and radiographic features of the proximal femur. EFORT Open Rev 2025;10:e20240129. [Google Scholar] [PubMed]
- 11. Haidukewych GJ, Rothwell WS, Jacofsky DJ, Torchia ME, Berry DJ. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am 2004;86:1711-6. [Google Scholar] [PubMed]
- 12. Li Y, Sun D, Wang K, Liu J, Wang Z, Liu Y. Postoperative avascular necrosis of the femoral head in pediatric femoral neck fractures. PloS One 2022;17:e0268058. [Google Scholar] [PubMed]
- 13. Ratliff AH. Fractures of the neck of the femur in children. J Bone Joint Surg Br 1962;44-B:528-42. [Google Scholar] [PubMed]
- 14. Dong B, Li F, Li C. Risk factors for avascular necrosis in pediatric femoral neck fractures: A systematic review and meta-analysis. J Orthop Surg 2025;20:989. [Google Scholar] [PubMed]
- 15. Leung PC, Lam SF. Long-term follow-up of children with femoral neck fractures. J Bone Joint Surg Br 1986;68:537-40. [Google Scholar] [PubMed]
- 16. Bagatur AE, Zorer G. Complications associated with surgically treated hip fractures in children. J Pediatr Orthop B 2002;11:219-28. [Google Scholar] [PubMed]
- 17. Bombaci H, Centel T, Babay A, Türkmen IM. Evaluation of complications of femoral neck fractures in children operated on at least 24 hours after initial trauma. Acta Orthop Traumatol Turc 2006;40:6-14. [Google Scholar] [PubMed]
- 18. Flynn JM, Wong KL, Yeh GL, Meyer JS, Davidson RS. Displaced fractures of the hip in children. Management by early operation and immobilisation in a hip spica cast. J Bone Joint Surg Br 2002;84:108-12. [Google Scholar] [PubMed]
- 19. Togrul E, Bayram H, Gulsen M, Kalaci A, Ozbarlas S. Fractures of the femoral neck in children: Long-term follow-up in 62 hip fractures. Injury 2005;36:123-30. [Google Scholar] [PubMed]
- 20. Inan U, Köse N, Omeroğlu H. Pediatric femur neck fractures: A retrospective analysis of 39 hips. J Child Orthop 2009;3:259-64. [Google Scholar] [PubMed]
- 21. Moon ES, Mehlman CT. Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta-analysis of 360 cases. J Orthop Trauma 2006;20:323-9. [Google Scholar] [PubMed]
- 22. Feng W, Zhang H, Zhu D, Song B, Wang Q. Clinical features of pediatric femoral neck fractures and analysis of risk factors for avascular necrosis of the femoral head: A retrospective case-control study of 45 patients. Injury 2024;55:111829. [Google Scholar] [PubMed]
- 23. Herring JA. Tachdjian’s Pediatric Orthopaedics. 4th ed. Philadelphia, PA: Saunders; 2008. [Google Scholar] [PubMed]
- 24. Chandankere V, Shah H. Controversies in the management of pediatric neck femur fractures- a systematic review. J Orthop 2021;27:92-102. [Google Scholar] [PubMed]
- 25. Morsy HA. Complications of fracture of the neck of the femur in children. A long-term follow-up study. Injury 2001;32:45-51. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System March 1, 2026 Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review
March 1, 2026 Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting
March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes
March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes