
In elderly patients undergoing primary total hip arthroplasty, cemented femoral fixation provides superior mid- to late-term functional outcomes without increasing short-term complication rates compared with cementless fixation.
Dr. Santosh Kumar Mishra, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India. E-mail: doctorskmishra@gmail.com
Introduction: Total hip arthroplasty (THA) is an effective intervention for advanced hip disorders in elderly patients; however, the optimal method of femoral fixation remains debated. This study compared clinical, intraoperative, and radiographic outcomes of cemented versus cementless THA in an elderly population.
Material and Methods: This prospective cohort study included 120 patients aged 65 years or older who underwent primary unilateral THA. Patients were allocated to either a cemented (n = 60) or cementless (n = 60) femoral fixation group based on intraoperative assessment. Baseline characteristics were comparable between groups. Operative time, blood loss, complications, radiographic outcomes, and functional recovery using the Harris Hip score (HHS) were evaluated over a 12-month follow-up. Statistical analysis was performed with a significance threshold of P < 0.05.
Results: Mean operative time and intraoperative blood loss were significantly higher in the cemented THA group compared with the cementless group (P < 0.01 and P = 0.002, respectively). Functional outcomes improved progressively in both cohorts. While early post-operative HHS did not differ significantly, cemented THA demonstrated superior functional scores at 6 months (P = 0.03) and 12 months (P = 0.002). The incidence of post-operative complications, including infection, dislocation, aseptic loosening, and mortality, was low and comparable between groups. Radiographic assessment revealed no significant differences in stem subsidence, radiolucent lines, or implant alignment at final follow-up.
Conclusion: Both cemented and cementless THA provide favorable outcomes in elderly patients. Cemented fixation is associated with improved mid- and late-term functional outcomes without an increase in short-term complications, supporting its continued use in this population.
Keywords: Total hip arthroplasty, cemented fixation, cementless fixation, elderly patients, Harris Hip score.
Total hip arthroplasty (THA) is one of the most effective reconstructive procedures for restoring mobility and relieving pain in degenerative and fracture-related hip pathology. As life expectancy increases, a growing proportion of THAs is performed in older adults who commonly present with reduced bone quality, multiple comorbidities, and higher perioperative vulnerability. In this population, the method of implant fixation – cemented versus cementless – remains a clinically important decision because it may influence early stability, complication patterns, and functional recovery [1]. Cemented femoral fixation provides immediate mechanical stability and may be advantageous in osteoporotic bone, where press-fit fixation can be unpredictable. Conversely, cementless stems aim for biological osseointegration and have become widely used, partly due to perceived advantages in operative efficiency and long-term fixation. However, in elderly patients, the balance between early mechanical stability and the risks associated with each technique (including perioperative and implant-related complications) is not fully resolved, and age-based thresholds for fixation choice remain debated [2]. Evidence differs depending on the clinical indication. In displaced femoral neck fractures – where rapid mobilization and early stability are critical – randomized data have suggested higher early hip-related complications with uncemented stems compared with cemented stems, including periprosthetic fractures and dislocations, while mortality and functional outcomes were similar in the short term [3]. Importantly, extended follow-up of the same trial cohort has shown that the complication profile can evolve over time; despite early excess complications with uncemented stems, longer-term outcomes did not demonstrate a progressive accumulation of late failures in the uncemented group, underscoring the value of studying both early and mid- to long-term endpoints when comparing fixation strategies in older adults [4]. Complementing trial evidence, contemporary observational data in patients aged 65 years and older undergoing THA after femoral neck fracture have continued to evaluate whether cemented fixation reduces post-operative complications compared with cementless fixation in real-world practice [5]. For elective THA in older patients (predominantly for degenerative disease), recent large cohort evidence has reported comparable medium- and long-term survivorship and similar improvements in patient-reported outcomes between cemented and cementless stems among individuals aged ≥70 years, suggesting that both fixation methods can be effective in appropriately selected elderly patients [6]. Nevertheless, registry analyses in fracture-related arthroplasty highlight that fixation choices beyond the femoral stem (including acetabular fixation) may influence revision patterns and mortality signals, emphasizing that “cemented versus cementless” is not a single uniform exposure and may vary by implant construct and clinical context [7]. Given these mixed findings across indications and study designs, there remains a need for prospective, systematically collected clinical data comparing cemented and cementless THA in elderly patients using standardized outcome measures, including functional scores, radiographic assessment, and complication surveillance. The present prospective cohort study was designed to compare clinical outcomes and complication profiles of cemented versus cementless THA in an elderly population treated at our institution, with the aim of generating clinically applicable evidence to inform fixation strategy selection in routine practice.
Study design and setting
This prospective cohort study was conducted at a tertiary care teaching hospital. Elderly patients undergoing primary THA were followed longitudinally and grouped according to the method of femoral fixation – cemented or cementless – based on the operating surgeon’s standard practice and intraoperative assessment of bone quality.
Ethical considerations
The study protocol was approved by the Institutional Ethics Committee (Ref. No. 175/IEC/GMC/2024; October 11, 2024). Written informed consent was obtained from all participants prior to enrollment, and the study was conducted in accordance with the principles of the Declaration of Helsinki.
Study population
Patients aged ≥65 years with end-stage hip pathology requiring primary unilateral THA were screened for eligibility. Indications for surgery included primary osteoarthritis, avascular necrosis of the femoral head, and displaced intracapsular fracture of the neck of the femur.
Inclusion criteria were:
- Age 65 years or older
- Ability to ambulate independently or with support prior to surgery
- Willingness to participate and provide written informed consent.
Exclusion criteria were:
- Revision hip arthroplasty
- Inflammatory arthropathies (e.g., rheumatoid arthritis)
- Active local or systemic infection
- Severe neuromuscular disorders affecting gait
- Pathological fractures or malignancy involving the hip.
Sample size estimation
Sample size was calculated assuming a clinically meaningful difference of 7 points in the Harris Hip score (HHS) between the two groups at 1 year, with a standard deviation of 12, a two-sided alpha of 0.05, and a power of 80%. The minimum required sample was 52 patients per group. Anticipating a 10–15% loss to follow-up, a total of 120 patients were enrolled, with 60 patients allocated to each cohort.
Group allocation
Patients were assigned to either
- Cemented THA group, in which polymethyl methacrylate bone cement was used for femoral stem fixation, or
- Cementless THA group, in which press-fit, porous-coated femoral stems were implanted without cement.
Acetabular components were cementless in both groups to maintain uniformity.
Surgical technique
All procedures were performed by experienced orthopedic surgeons using a standardized posterolateral approach under spinal or combined spinal–epidural anesthesia. Prophylactic antibiotics were administered preoperatively and continued for 24 h postoperatively. Implant selection was based on pre-operative templating and intraoperative stability. Post-operative rehabilitation protocols, including early mobilization and weight-bearing status, were identical for both groups.
Outcome measures
The primary outcome was functional outcome assessed using the HHS at 3 months, 6 months, and 12 months postoperatively.
Secondary outcomes included:
- Operative time
- Intraoperative blood loss
- Early post-operative complications (periprosthetic fracture, infection, dislocation)
- Radiographic evidence of loosening or subsidence
- Mortality within 12 months.
Standardized anteroposterior pelvic radiographs were obtained immediately after surgery and at each follow-up visit.
Follow-up
Patients were reviewed clinically and radiographically at 6 weeks, 3 months, 6 months, and 12 months. Any adverse events or reoperations were recorded prospectively.
Statistical analysis
Data were analyzed using Epi Info (v7.0). Continuous variables were expressed as mean ± standard deviation and compared using the independent samples t-test. Categorical variables were analyzed using the Chi-square test. P < 0.05 was considered statistically significant.
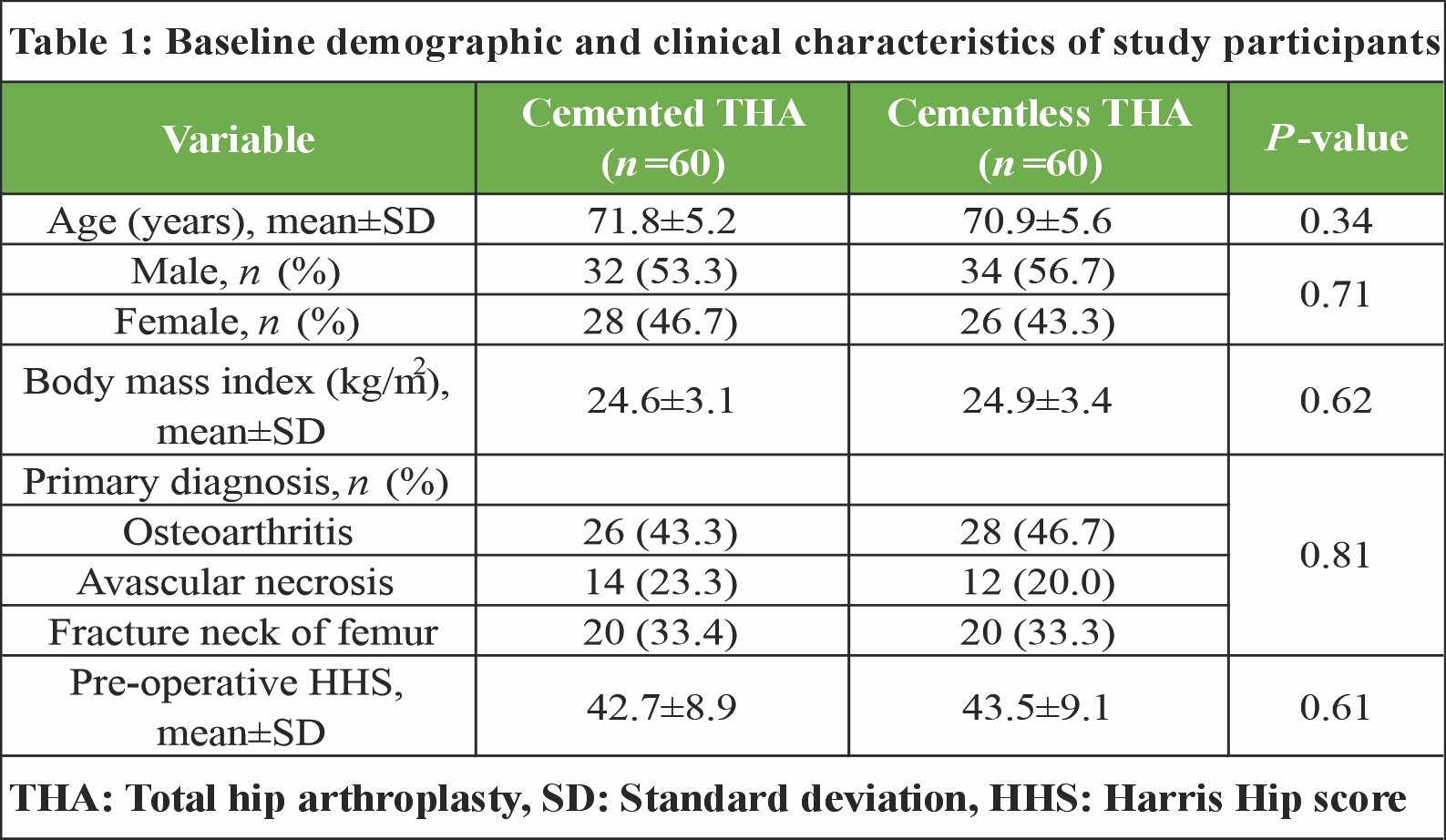
The two groups were comparable with respect to baseline demographic and clinical variables. Mean age was 71.8 ± 5.2 years in the cemented group and 70.9 ± 5.6 years in the cementless group (P = 0.34). Sex distribution, body mass index, primary indication for surgery, and pre-operative HHS did not differ significantly between groups (Table 1).
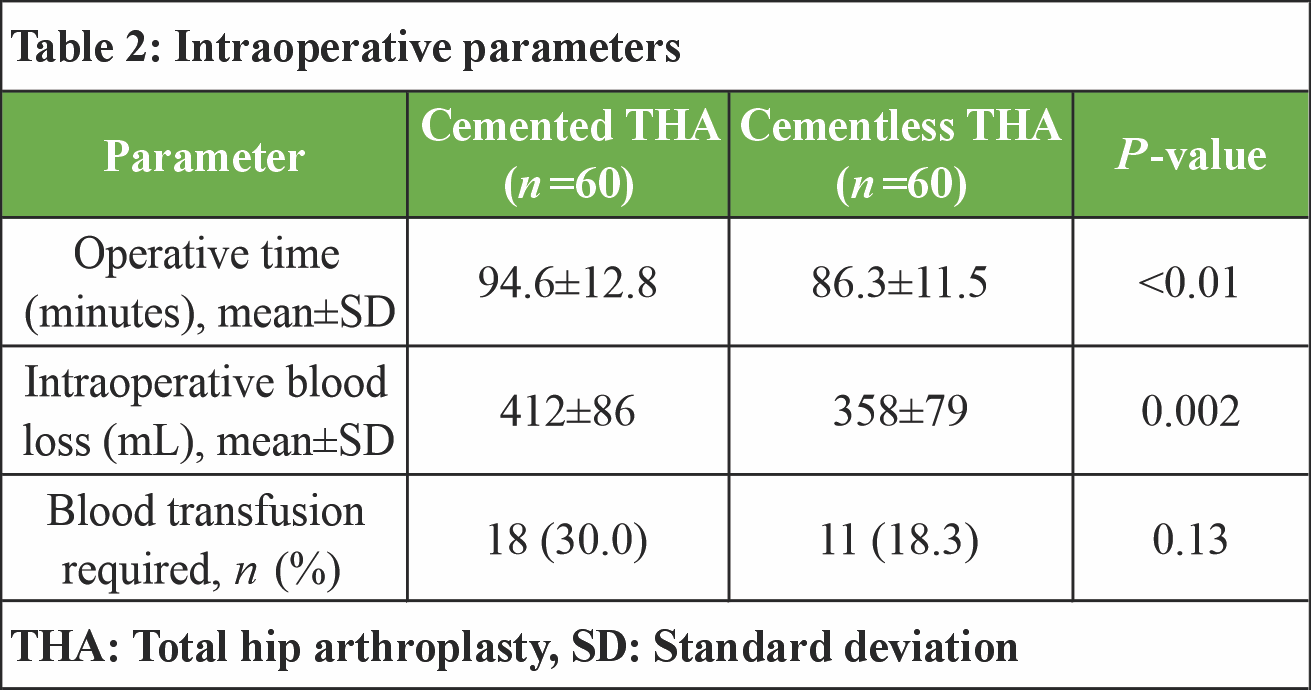
Mean operative duration was significantly longer in the cemented THA group compared with the cementless group (94.6 ± 12.8 minutes vs. 86.3 ± 11.5 min, P < 0.01). Intraoperative blood loss was also higher in patients receiving cemented fixation (412 ± 86 mL vs. 358 ± 79 mL, P = 0.002). Although a greater proportion of patients in the cemented group required perioperative blood transfusion, this difference did not reach statistical significance (Table 2).
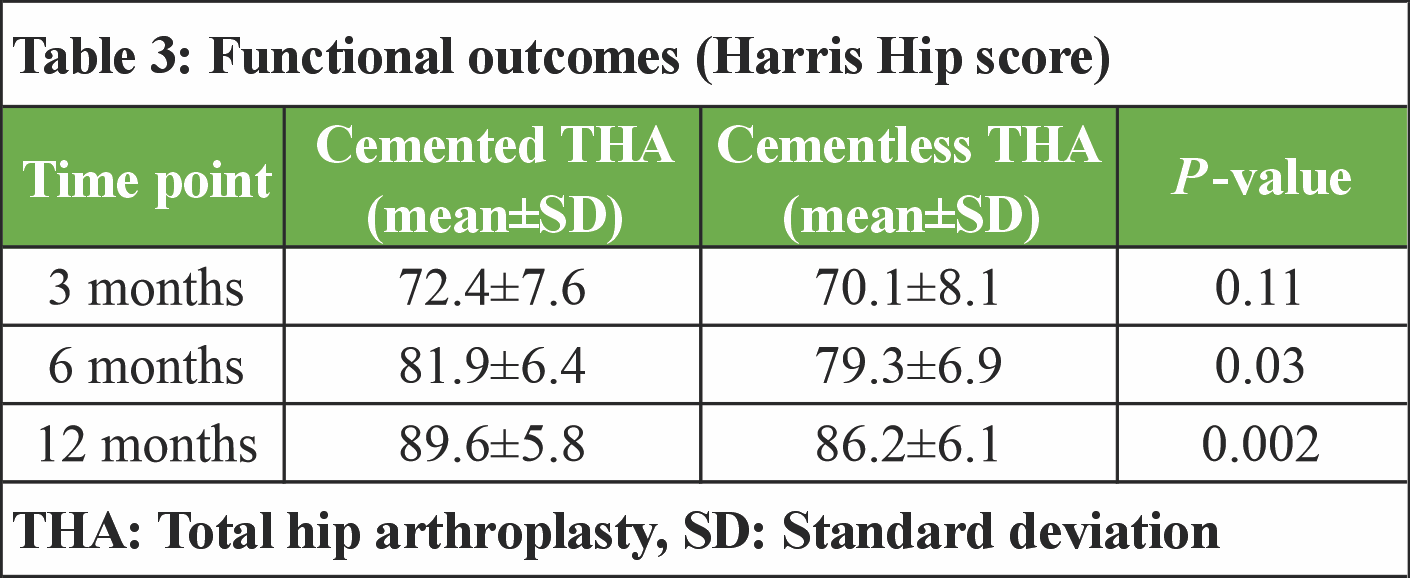
Both groups demonstrated progressive improvement in functional outcomes over time. At 3 months postoperatively, the mean HHS was comparable between the cemented and cementless THA groups (72.4 ± 7.6 vs. 70.1 ± 8.1, P = 0.11). At 6 months, patients in the cemented group showed significantly higher scores (81.9 ± 6.4 vs. 79.3 ± 6.9, P = 0.03). This difference persisted at 12 months, with the cemented THA group achieving a superior mean HHS (89.6 ± 5.8 vs. 86.2 ± 6.1, P = 0.002) (Table 3).
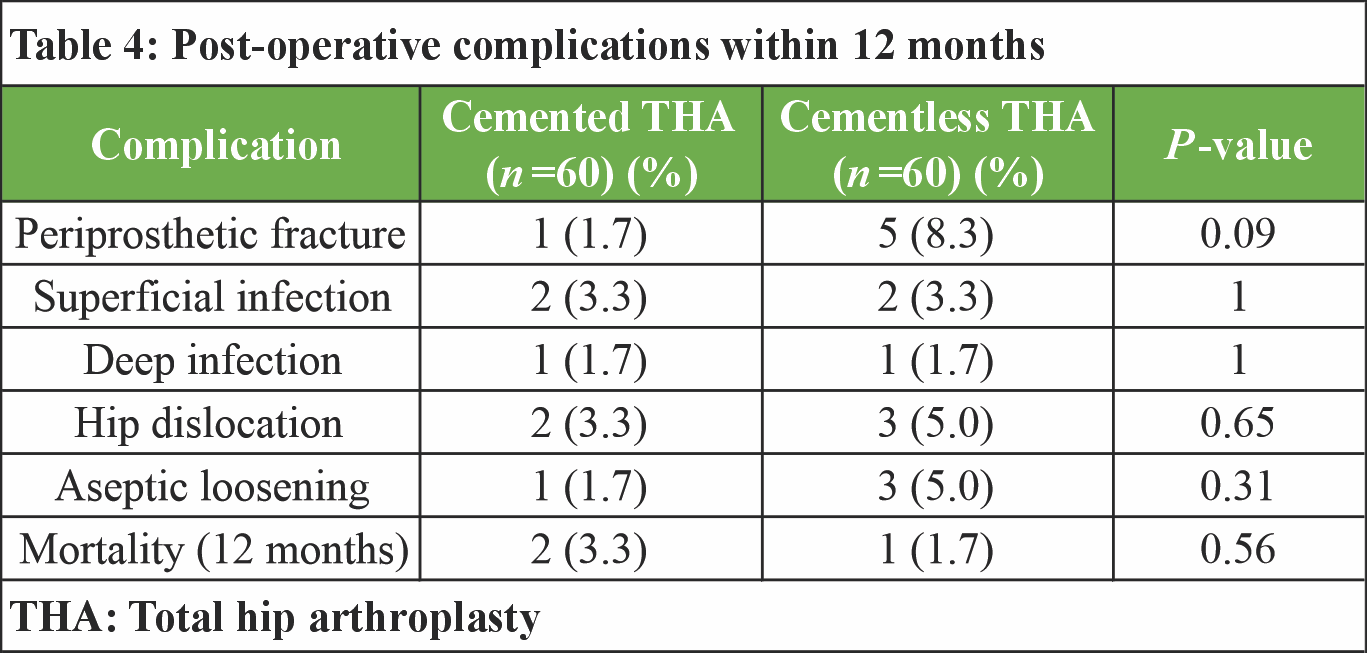
The overall incidence of post-operative complications within 12 months was low in both groups. Periprosthetic fractures occurred more frequently in the cementless THA group; however, this difference was not statistically significant. Rates of superficial and deep infection, hip dislocation, aseptic loosening, and 12-month mortality were comparable between the two cohorts, with no statistically significant differences observed (Table 4).
At final follow-up, radiographic evaluation revealed a low incidence of femoral stem subsidence and radiolucent lines in both groups. Stem subsidence >2 mm was more commonly observed in the cementless THA group, though the difference was not statistically significant. The majority of implants in both groups demonstrated satisfactory alignment on radiographs, with no significant intergroup difference (Table 5 and Fig. 1).
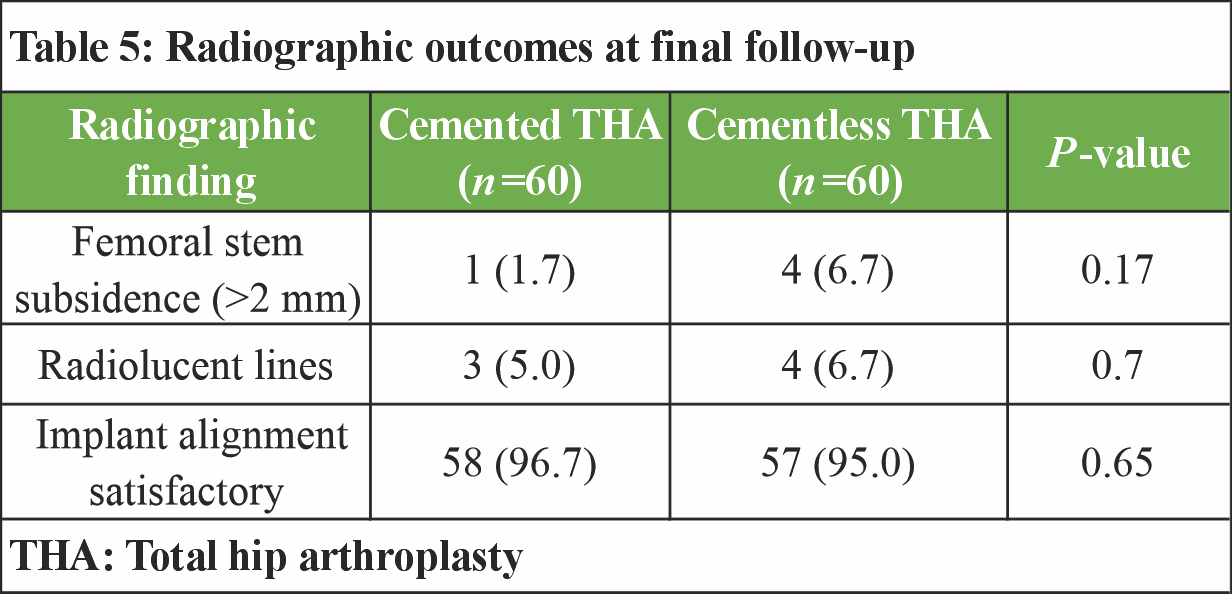
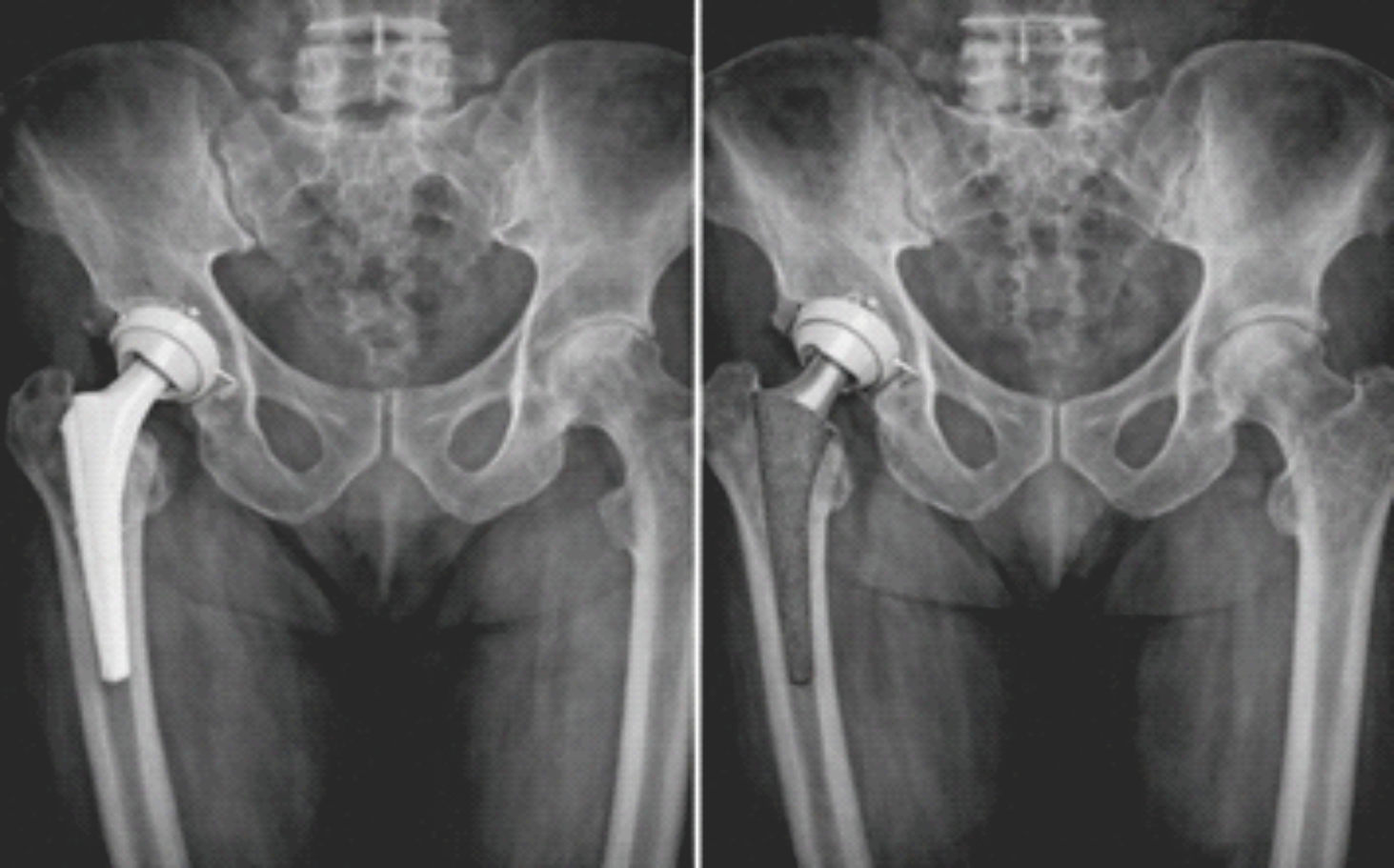
Figure 1: Anteroposterior pelvic radiograph comparing a cemented femoral stem (left) to a cementless femoral stem in direct bone contact (right).
In this prospective cohort of elderly patients who underwent primary THA, both fixation strategies produced substantial functional improvement with low complication rates at 12 months. The key findings were (i) cemented THA required longer operative time and was associated with higher intraoperative blood loss, (ii) functional recovery favored cemented fixation at 6 and 12 months, and (iii) early complications and radiographic adverse findings were uncommon and broadly comparable, although numerically more periprosthetic fractures and stem subsidence were observed in the cementless group.
The longer operative time and higher blood loss observed with cemented fixation are clinically plausible because cementing adds procedural steps (canal preparation, cement pressurization, stem insertion, and curing). Contemporary clinical comparisons have similarly reported shorter operative times with cementless femoral fixation in routine THA settings, supporting the direction of our intraoperative findings [8]. From a practical standpoint, these differences may be relevant in frail elderly patients where surgical duration and blood loss can influence early recovery trajectories and resource utilization, even when transfusion rates are not significantly different.
A notable finding in the present study was the higher HHS in the cemented group at 6 and 12 months. This may reflect more predictable early mechanical stability of cemented stems in osteoporotic bone, potentially facilitating confident rehabilitation and gait restoration. Evidence across populations remains mixed; however, registry-based and cohort data indicate that fixation-related outcomes can vary by age and sex, with older individuals – particularly elderly women – showing higher vulnerability to stem-related failure patterns when cementless fixation is used [9,10]. These observations support the concept that elderly patients represent a biologically distinct group in whom immediate fixation reliability may translate into measurable functional differences over the 1st post-operative year.
Although overall complication rates were low and statistically comparable, our data showed a numerical excess of periprosthetic fractures in the cementless group. This direction is consistent with broader evidence: database and registry analyses frequently identify periprosthetic femoral fracture as a more common early failure mode with cementless stems in older patients, which is one reason some health systems have promoted cemented fixation in targeted elderly cohorts [11]. In addition, systematic review evidence focused on arthroplasty for elderly femoral neck fracture populations has reported higher implant-related complication burdens with uncemented fixation, particularly related to fracture risk and early mechanical events [12]. While our cohort was not powered to detect small differences in uncommon events, the observed trend aligns with the wider literature and reinforces the importance of fixation choice in patients with compromised femoral bone stock.
Radiographic differences between groups were modest. The slightly higher frequency of clinically relevant subsidence (>2 mm) and radiolucent findings in the cementless group, without statistically significant separation, is compatible with early settling behavior described for press-fit stems – especially in elderly bone – while remaining within a low absolute event rate. Large cohort studies have highlighted that implant design and fixation philosophy (e.g., collared versus collarless; metaphyseal versus metadiaphyseal filling) can modify revision and complication risks, implying that “cementless” is not a single uniform exposure [13]. This nuance is clinically important when interpreting our results, as outcomes may differ with alternative stem geometries or surface technologies.
A key concern with cemented femoral stems is bone cement implantation syndrome (BCIS), characterized by intraoperative hypoxia, hypotension, and, in severe cases, cardiovascular collapse. Contemporary syntheses report that BCIS can occur during cemented arthroplasty, with risk influenced by patient frailty and comorbidity burden [14,15]. Although our study did not quantify intraoperative physiological events as a formal endpoint, the broader evidence emphasizes that cemented fixation in elderly patients should be accompanied by systematic anesthetic and surgical precautions (e.g., optimized volume status, high inspired oxygen during cementing, and vigilant hemodynamic monitoring), particularly in high-risk individuals.
Internationally, fixation practice continues to vary, with some systems showing increasing cementless utilization even in older age groups, whereas others have implemented targeted strategies to increase cemented fixation in elderly patients to mitigate fracture-related failures [16]. Our findings contribute prospective clinical data supporting the view that cemented fixation can provide functional advantages during the 1st post-operative year in an elderly cohort, without a detectable increase in early adverse outcomes – while recognizing that longer operative time and blood loss are trade-offs to consider.
The prospective design, standardized follow-up intervals, and parallel assessment of function, complications, and radiographs strengthen interpretability. However, several limitations should be acknowledged. First, allocation was not randomized, so unmeasured confounding (e.g., subtle differences in bone quality, surgeon preference, or implant selection) may have influenced outcomes. Second, the follow-up period of 12 months captures early and mid-term recovery but cannot address longer-term revision risk or late loosening patterns. Third, uncommon complications (including severe BCIS, deep infection, or aseptic loosening) require larger samples to compare reliably. Finally, subgroup analyses by indication (osteoarthritis vs. avascular necrosis vs. fracture neck of femur) were not performed and may yield additional clinically relevant insights.
This study has certain limitations. The non-randomized design and allocation based on intraoperative judgment and surgeon preference may introduce selection bias and residual confounding despite comparable baseline characteristics. Being a single-center study, the findings may not be fully generalizable to other institutions with different patient profiles or surgical practices. The 12-month follow-up captures early and mid-term outcomes but does not permit assessment of long-term implant survivorship or revision rates. The sample size was powered for functional outcomes rather than rare complications, limiting reliable comparison of infrequent adverse events. Inclusion of heterogeneous indications (osteoarthritis, avascular necrosis, and fracture neck of femur) may have introduced variability that was not explored through subgroup analysis. Bone quality assessment was based on intraoperative evaluation rather than standardized objective measures such as dual-energy X-ray absorptiometry. Functional assessment relied solely on the HHS without additional patient-reported outcome measures. Implant-specific design variables were not analyzed separately, and outcome assessment was not blinded, which may introduce observer bias. Economic considerations and cost-effectiveness were not evaluated.
In elderly patients undergoing primary THA, both cemented and cementless fixation techniques resulted in satisfactory clinical and radiographic outcomes at 1-year follow-up. Cemented THA was associated with longer operative time and greater intraoperative blood loss but demonstrated superior functional recovery at mid- and late-term follow-up compared with cementless fixation. The incidence of post-operative complications and radiographic abnormalities was low and comparable between the two techniques. These findings suggest that cemented femoral fixation may offer functional advantages in the elderly population without increasing short-term complication rates, whereas cementless fixation remains a viable alternative when appropriately selected.
The selection of femoral fixation in elderly patients should account for bone quality and the need for reliable early implant stability. Cemented THA, despite slightly longer operative time and greater blood loss, offers more consistent functional recovery over the 1st post-operative year. Cementless fixation remains an acceptable option in carefully selected elderly patients with good femoral bone stock. An individualized fixation strategy, rather than age alone, is essential to optimize outcomes and minimize complications in this population.
References
- 1. Axenhus M, Chammout G, Kelly-Pettersson P, Mukka S, Magnéli M, Sköldenberg O. Long-term outcomes of cemented compared to uncemented femoral stems in total hip arthroplasty for displaced femoral neck fractures in elderly patients. Eur J Trauma Emerg Surg 2025;51:73. [Google Scholar] [PubMed]
- 2. Konan S, Abdel MP, Haddad FS. Cemented versus uncemented hip implant fixation: Should there be age thresholds? Bone Joint Res 2020;8:604-7. [Google Scholar] [PubMed]
- 3. Chammout G, Muren O, Laurencikas E, Bodén H, Kelly-Pettersson P, Sjöö H, et al. More complications with uncemented than cemented femoral stems in total hip replacement for displaced femoral neck fractures in the elderly. Acta Orthop 2017;88:145-51. [Google Scholar] [PubMed]
- 4. Gounot A, Charlot A, Guillon P, Schaefer A, Moslemi A, Boutroux P, et al. The use of uncemented stems in femoral neck fractures in elderly patients: A comparative study of 671 cases. Orthop Traumatol Surg Res 2024;110:103878. [Google Scholar] [PubMed]
- 5. Hameed D, McCormick BP, Sequeira SB, Dubin JA, Bains SS, Mont MA, et al. Cemented versus cementless femoral fixation for total hip arthroplasty following femoral neck fracture in patients aged 65 and older. J Arthroplasty 2024;39:1747-51. [Google Scholar] [PubMed]
- 6. Rocha AC, Somerville LE, Moody PW, Lanting BA, Howard JL, Naudie DD, et al. Cementless versus cemented stems in patients aged 70 years or older undergoing total hip arthroplasty. J Arthroplasty 2025;40:S250-4. [Google Scholar] [PubMed]
- 7. Roitzsch C, Rogmark C, Wu Y, Grimberg A, Lützner J, Postler A. Cemented versus cementless cup fixation in total hip arthroplasty for proximal femoral fractures: Analysis of revision and mortality rates from the German arthroplasty registry (EPRD). J Orthop Surg Res 2025;20:873. [Google Scholar] [PubMed]
- 8. Crockatt WK, El Othmani MM, Dupont MM, Okonkwo JT, Sarpong NO, Herndon CL. A comparative study on the outcome of cemented and cementless stems during total hip arthroplasty conversion in patients with failed osteosynthesis of proximal femur fracture. Hip Pelvis 2025;37:137-44. [Google Scholar] [PubMed]
- 9. Kelly MP, Chan PH, Prentice HA, Paxton EW, Hinman AD, Khatod M. Cause-specific stem revision risk in primary total hip arthroplasty using cemented vs cementless femoral stem fixation in a us cohort. J Arthroplasty 2022;37:89-96.e1. [Google Scholar] [PubMed]
- 10. Dale H, Børsheim S, Kristensen TB, Fenstad AM, Gjertsen JE, Hallan G, et al. Fixation, sex, and age: Highest risk of revision for uncemented stems in elderly women – data from 66,995 primary total hip arthroplasties in the Norwegian arthroplasty register. Acta Orthop 2020;91:33-41. [Google Scholar] [PubMed]
- 11. Gjertsen JE, Nilsen D, Furnes O, Hallan G, Kroken G, Dybvik E, et al. Promoting cemented fixation of the femoral stem in elderly female hip arthroplasty patients and elderly hip fracture patients: A retrospective cohort study from the Norwegian arthroplasty register and the Norwegian hip fracture register. Acta Orthop 2024;95:130-7. [Google Scholar] [PubMed]
- 12. Raja BS, Gowda AK, Singh S, Ansari S, Kalia RB, Paul S. Comparison of functional outcomes and complications of cemented vs uncemented total hip arthroplasty in the elderly neck of femur fracture patients: A systematic review and meta-analysis. J Clin Orthop Trauma 2022;29:101876. [Google Scholar] [PubMed]
- 13. Moore MC, Dubin JA, Monárrez R, Bains SS, Hameed D, Nace J, et al. Cemented versus cementless femoral fixation for total hip arthroplasty following osteoarthritis. J Arthroplasty 2024;39:1545-9. [Google Scholar] [PubMed]
- 14. Brokke KE, Graman M, Servaas S, Sierevelt IN, Steegers MA, Nolte PA. Bone cement implantation syndrome: A scoping review. Br J Anaesth 2025;135:1038-50. [Google Scholar] [PubMed]
- 15. Bonfait H, Delaunay C, De Thomasson E, Tracol P, Werther JR, Orthorisq. Bone cement implantation syndrome in hip arthroplasty: Frequency, severity and prevention. Orthop Traumatol Surg Res 2022;108:103139. [Google Scholar] [PubMed]
- 16. Gaidici T, Deckey DG, Seyler TM, Bolognesi MP, Spangehl MJ, Bingham JS. Femoral fixation for primary total hip arthroplasty-an international registry perspective. Arthroplast Today 2025;34:101755. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Managing Hip Arthritis in an Above-Knee Amputee: A Case Report of Total Hip Arthroplasty with Surgical Technique and Rehabilitation Considerations
March 1, 2026 Managing Hip Arthritis in an Above-Knee Amputee: A Case Report of Total Hip Arthroplasty with Surgical Technique and Rehabilitation Considerations March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting
March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting March 1, 2026 Evaluation of Spine Hip Relation and its Correlation as a Guide to Total Hip Arthroplasty
March 1, 2026 Evaluation of Spine Hip Relation and its Correlation as a Guide to Total Hip Arthroplasty March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes
March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes