
Ipsilateral in-tandem impalement injuries are rare and should be managed with avoidance of pre-hospital removal, careful preoperative assessment, and controlled removal in the operating room to prevent complications.
Dr. Chirag Sharma, Department of Orthopaedics, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India. E-mail: chiragammu@gmail.com
Introduction: Impalement injuries are rare injuries and require immediate limb and life-saving measures. Time is of the essence in such cases, and such situations can be challenging for the emergency care providers.
Case Report: We report an unusual case of 47-year-old male farmer who was brought to the emergency department with a rare combination of impalement injuries with metallic rotavator blades of a power-tiller lodged in his ipsilateral knee and ankle joints.
Conclusion: Impalement injuries are difficult and being rare often call for quick hospital mobilization and a multidisciplinary team management. The safe retrieval of a foreign body depends critically on the quality of pre-hospital care received and on a thorough clinical examination, relevant history, and careful pre-operative preparation.
Keywords: Impalement injury, Knee joint, Ankle joint, Agricultural trauma, Surgical management.
Concomitant penetrating injuries to the knee and ankle with sharp objects in a single patient are rarely seen. Penetrating trauma creates an open wound. There are three possible sequelae of penetrating injuries- the impaling object may act as a retained foreign body in the tissues; exits after it enters; or travels the entire length of tissue/organ to appear on opposite/another area [1]. When retained, it can act as a foreign body, resulting in complications such as soft-tissue damage, infection, and foreign body granuloma [2]. Impalement injuries are defined as “penetration of a body cavity or region by an elongated object which remains in situ following the injury’’ [3]. There is no fixed protocol for the management of such injuries. Time is of the essence in such cases, but a quick or lackadaisical attempt at retrieval can result in iatrogenic injuries to nearby critical structures or even retention of a part of the foreign body. This case report discusses a rare impalement injury in a rural farmer and the management undertaken thereof.
A 47-year-old male farmer was brought to the emergency department in the evening after 8 h of injury with an impalement injury. Metal rods (rotavator blades) were lodged in his right knee and right ankle joint. The injury occurred when the patient was working in his farm; he fell from his power tiller into the metallic rotavator blades of the power tiller. It took nearly 6 h for the bystanders to free him from the machine by disconnecting the shaft of the rotavator blades from the rotor. The cloth he was wearing (trouser) was also cut along with the blade as these were intertwined. On examination, two metallic rods (rotavator blades of the power tiller) were seen projecting out through the knee and ankle joints. One blade was seen traversing the knee joint entering through the popliteal fossa and exiting through the anterior aspect of the knee. The second blade was seen traversing the ankle through the posteromedial to anterolateral directions. The patient was, however, fully conscious and physiologically stable. There was no active bleeding, and fortunately, there was no neurovascular deficit. Dorsalis pedis artery pulsation was felt, and SpO2 of the affected limb in pulse oximetry was 100%. The knee was fixed at 70° flexion. Knee and ankle movements were not attempted as we expected these to be painfully restricted with risk of further damage to underlying structures (Figs. 1, 2, 3).

Figure 1: Clinical photo at presentation showing the exiting end of the rotavator blade in the right knee (anterior aspect) in 70° flexion.
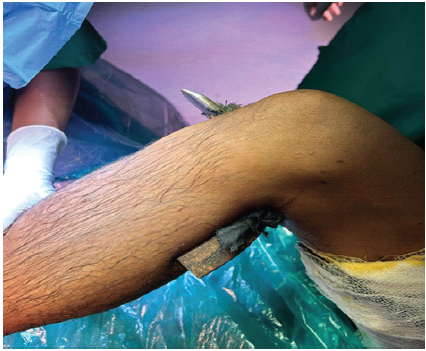
Figure 2: Lateral profile of right knee showing the metallic blade in situ with an impaled piece of clothing.

Figure 3: Clinical photo showing the metallic blade across the ankle joint.
After ensuring intravenous access and adequate analgesia, the patient party was counseled and prognosticated. He was administered tetanus prophylaxis and intravenous antibiotics. Now, attention was given to the wounds. All wounds were first washed with copious amount of normal saline. The visible ends of the two large metallic objects passing through the knee and ankle joints were also gently cleaned of all visible darts with saline and antiseptic solutions. Any fracture of the adjoining bones is quickly ruled out by doing X-ray examinations. Vascular Doppler study of the affected limb showed good biphasic flow in the dorsalis pedis and posterior tibial arteries. Angiogram was not advised by the vascular surgeon. Routine blood investigations, including blood grouping and cross-matching were sent as emergent, and the patient was planned for emergency surgery (Figs. 4 and 5).

Figure 4: X-ray of the knee joint with the metal rotavator blade in situ.

Figure 5: X-ray of the ankle joint showing the rotavator blade in situ.
After taking due informed consent, the patient was taken to the operation theatre after 3 h of his arrival. He was placed in a supine position on the operating table. General anesthesia was administered and airway secured. A tourniquet was used at an appropriate pressure to aid in the procedure. The vascular surgery team was informed to be in standby mode. Removal of blade from the ankle was attempted first. Incisions were given at the entry and exit wounds, and a thorough wash was given. The metallic blade was removed with a single pull. Twists and turns were avoided to prevent any iatrogenic damage to the surrounding structures [4]. The area was thoroughly washed once more with normal saline and diluted betadine. Incisions were then carefully made without deep dissection at the entry and exit wounds in the knee. A light mallet was used to gently strike at the anterior aspect of the metallic blade in a controlled manner. The rod was then removed with a single pull. Along with the blade, the entire portion of the torn clothing was removed. Careful debridement was then done at both sites (knee and ankle) along with copious irrigation. Complete removal of the objects was confirmed clinically and through fluoroscopy. Gentle examination under anesthesia (Joint stability tests) was then performed, which suggested ligament injuries in both sites. The tourniquet was then deflated to check for any inadvertent arterial injury. SpO2 of the limb was >94%. Once the absence of arterial injury was confirmed, the wound was closed in layers. An above-knee anterior slab was put for adding stability of the joints and injured soft tissues. The post-operative radiograph documented the absence of any foreign bodies. Post-operatively an magnetic resonance imaging (MRI) was also done, which confirmed lateral meniscus and lateral collateral ligament injuries, anterior talofibular, calcaneofibular and tibiotalar ligaments in both the knee and the ankle, respectively. Absence of any retained clothing was also confirmed in the MRI. His post-operative hospital stay was mostly uneventful except for a superficial wound infection at the popliteal entry wound that eventually healed with IV antibiotics, single debridement, and regular dressings. The sutures were removed at the end of the 2nd week. The patient was then discharged in satisfactory clinical condition with the explanation that he may eventually require knee and ankle arthroscopy and reconstruction of some of the critically torn ligaments of the knee and ankle joint if these fail to heal satisfactorily (Fig. 6, 7, 8, 9, 10).

Figure 6: Intra-operative photograph showing the removal of the foreign object from the ankle.

Figure 7: The J-type rotavator blades (used in deep tilling) retrieved at surgery (Top- from the knee; Bottom- from the ankle).

Figure 8: The fragment of the patient’s clothing that was driven into the popliteal entry wound with the blade.
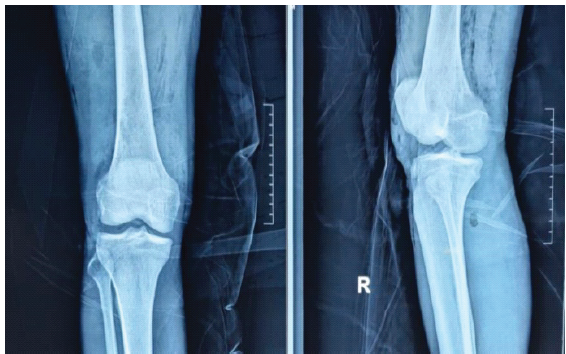
Figure 9: Post-operative anterior – posterior and lateral check radiograph of the right knee.
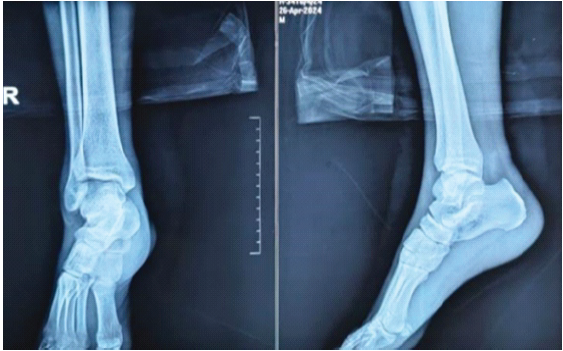
Figure 10: Post-operative (Anteroposterior and Lateral) radiograph of the right ankle.
Eachempati et al. [5] describe two types of impalement injuries. In Type 1 injuries, the human body or body parts strike an immobile object; often seen in industrial and vehicular accidents when the victim is ejected out. In Type 2 injuries, a moving object penetrates an immobile human body. The region of the body involved, nature of the impaling object, and the quantum of energy dissipated to the tissue dictates the severity of injury [1]. To the best of our knowledge, penetrating injuries involving two consecutive, ipsilateral joints in a single patient have not been previously described in the literature [6]. It is vital to fathom that an impaled object must not be removed in the pre-hospital setting in impalement injuries. This is because more often than not, vascular lesions remain sealed (albeit temporarily) by the impaling object itself, avoiding catastrophic hemorrhage [4]. Oftentimes, the penetrating object provides a tamponade effect, and hence removal of such object (metallic, organic, inorganic) may potentially cause torrential bleed [7,8]. X-ray examination is the investigation of choice for the assessment of an impaled object. Understanding the loco-regional anatomy is crucial for safe exploration. Nerve and blood vessels are at risk in terms of their damage either at the very time of injury or during removal or exploration [8]. Nearby structures and tissues, if damaged, may need primary repair mandating a multi-disciplinary surgical team, and this should be anticipated without fail while planning its removal [8]. Optimum anesthesia, precaution, teamwork, lighting, and time are necessary for safe and successful retrieval of the impaling object [2]. It may also be necessary to use a tourniquet subject to the nature of the injury. The best way to retrieve an impaling object is to follow the path of its insertion [8]. In our case, we had carefully enlarged the entry and exit points of the wound with skin incisions and it had made removal effective and easier. A thorough debridement and antibiotic prophylaxis are paramount. The choice of antibiotics (broad-spectrum cephalosporins) is preferred depending on the situations (mode of exposure/event) [9]. Various complications mentioned in literature are retained/missed foreign bodies, migration into joint cavities, injuries to nerves and vessels, delayed inflammatory reactions, granuloma formation, and infection [2,10]. Missed foreign bodies are common and can be a cause for litigation [11]. Hence, to avoid potential litigation of such known complications, it is imperative to explain well while taking informed consent before, during and after the attempted removal of impaled objects. This also entails proper record keeping before, during and after surgery to corroborate ( clinical images, radiological images and other investigations and reports) [4,12]. A penetrating trauma rarely results in a localized damage alone. We were fortunate that the neurovascular integrity was preserved despite the metallic blades being close to the named arteries (popliteal, anterior, and posterior tibial arteries).
Impalement injuries are difficult and being rare, call for quick hospital mobilization and a multidisciplinary team management. The safe retrieval of a foreign body depends critically on a thorough clinical examination, careful preparation, and a detailed history. No attempt should be made to remove impaling objects in the emergency room. Surgical exploration should always be performed in the operating room only, since retrievals may require extraordinary support from other surgical specialties and anesthesia. Removal done using a single pull technique facilitates safe retrieval and helps in avoiding neurovascular injuries.
Impalement injuries should never be managed by premature removal of the foreign body outside the operating room. Thorough assessment, multidisciplinary preparedness, and controlled extraction along the path of entry, followed by meticulous debridement, are essential to prevent neurovascular injury, infection, retained foreign bodies, and medicolegal complications.
References
- 1. Stewart MG. Principles of ballistics and penetrating trauma. In: Head, Face and Neck Trauma: Comprehensive Management. New York: Thieme; 2005. p. 188-94. [Google Scholar] [PubMed]
- 2. Lammers RL. Soft tissue foreign bodies. Ann Emerg Med 1988;17:1336-44. [Google Scholar] [PubMed]
- 3. Hyde MR, Schmidt CA, Jacobson JG, Vyhmeister EE, Laughlin LL. Impalement injuries to the thorax as a result of motor vehicle accidents. Ann Thorac Surg 1987;43:189-90. [Google Scholar] [PubMed]
- 4. Shaji G, Franco AC. A case report of penetrating extremity trauma: A near miss encounter. J Orthop Case Rep 2021;11:106-9. [Google Scholar] [PubMed]
- 5. Eachempati SR, Barie PS, Reed RL 2nd. Survival after transabdominal impalement from a construction injury: A review of the management of impalement injuries. J Trauma 1999;47:864-6. [Google Scholar] [PubMed]
- 6. Kerketta AH, Kumar R, Sahu S, Laik JK, Rajak MK. Wooden foreign body impalement through the right shoulder region – an unusual penetrating injury: A case report. World J Orthop 2022;13:1064-8. [Google Scholar] [PubMed]
- 7. Bravman JT, Ipaktchi K, Biffl WL, Stahel PF. Vascular injuries after minor blunt upper extremity trauma: Pitfalls in the recognition and diagnosis of potential “near miss”injuries. Scand J Trauma Resusc Emerg Med 2008;16:16. [Google Scholar] [PubMed]
- 8. Skinner EJ, Morrison CA. Wound Foreign body removal. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar] [PubMed]
- 9. Mirzayan R, Schnall SB, Chon JH, Holtom PD, Patzakis MJ, Stevanovic MV. Culture results and amputation rates in high-pressure paint gun injuries of the hand. Orthopedics 2001;24:587-9. [Google Scholar] [PubMed]
- 10. Singh A, Kaur A, Singh M. Missed foreign body in the arm-a case report. Glob J Res Anal 2017;6:337-8. [Google Scholar] [PubMed]
- 11. Govindaraju RC, Munavalli J. Difficulties in the management of impalement injuries sustained in rural India. J Emerg Trauma Shock 2020;13:227-30. [Google Scholar] [PubMed]
- 12. Vukmir RB. Medical malpractice: Managing the risk. Med Law 2004;23:495-513. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 The Clean Pass: Upper Limb Impalement with Complete Neurovascular Preservation
February 1, 2026 The Clean Pass: Upper Limb Impalement with Complete Neurovascular Preservation February 1, 2026 Knee Joint Dislocation in a Difficult, Low-Resource Himalayan Setting: A Longitudinal Functional Outcome Study
February 1, 2026 Knee Joint Dislocation in a Difficult, Low-Resource Himalayan Setting: A Longitudinal Functional Outcome Study January 1, 2026 A Case Report of an Intra-Articular Lipoma in the Inferomedial Recess of the Anterior Knee Joint: Clinical Implications and Diagnostic Challenges: Case Report and Review of Literature
January 1, 2026 A Case Report of an Intra-Articular Lipoma in the Inferomedial Recess of the Anterior Knee Joint: Clinical Implications and Diagnostic Challenges: Case Report and Review of Literature January 1, 2026 Single Stage Autologous Minced Cartilage Implantation for Chondral Defects of the Knee: A Case Series
January 1, 2026 Single Stage Autologous Minced Cartilage Implantation for Chondral Defects of the Knee: A Case Series