
Awareness of normal post-operative biomarker trajectories helps prevent misdiagnosis of periprosthetic joint infection or venous thromboembolism in the early post-operative period.
Dr. Yogesh Singh Parihar, Department of Orthopaedics, Gajra Raja Medical College, Gwalior, Madhya Pradesh, India. E-mail: yogeshsinghparihar123@gmail.com
Introduction: Total joint arthroplasty, including total hip and knee replacement, is among the most successful orthopedic interventions for end-stage arthritis. However, complications, such as periprosthetic joint infection and venous thromboembolism remain significant causes of morbidity. Serum biomarkers, such as D-dimer, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP), are commonly used to assess post-operative inflammation and potential complications. Despite extensive literature worldwide, normative post-operative biomarker trends in Indian patients remain poorly defined.
Materials and Methods: A prospective observational study was conducted in the Department of Orthopaedics, G.R. Medical College and J.A. Group of Hospitals, Gwalior, from October 2022 to June 2024. Fifty patients (25 total hip arthroplasty and 25 total knee arthroplasty) aged ≥50 years were enrolled. Serial serum D dimer, CRP, ESR, total leukocyte count, sodium, and calcium levels were measured pre-operatively and on post-operative days 1, 3, 5, 7, 14, and 28. Results: D-dimer exhibited a biphasic response – a rapid increase within 24 h (mean ≈ ×8.6 baseline), a fall by day 3, a secondary peak around day 10–14, and normalization by week 4. CRP peaked on day 3 and ESR on day 5, both showing a gradual decline thereafter. Mild transient post-operative hyponatremia was observed in 12% of cases. No infection or thromboembolic events occurred.
Conclusion: Transient elevations of D-dimer, ESR, and CRP represent the expected physiological ostoperative response after uncomplicated arthroplasty. Recognizing these normal patterns helps differentiate benign post-operative inflammation from infection or thrombosis, preventing unnecessary interventions.
Keywords: Arthroplasty, biomarkers, C-reactive protein, d-dimer, erythrocyte sedimentation rate.
Total joint arthroplasty (TJA) is a cornerstone of modern orthopedic surgery, providing reliable pain relief and functional recovery in advanced osteoarthritis and post-traumatic arthritis [1]. With rising life expectancy and better access to surgical care, the demand for TJA is increasing worldwide, including in developing nations [2]. Despite its success, post-operative complications, such as periprosthetic joint infection (PJI), venous thromboembolism (VTE), and aseptic loosening continue to pose diagnostic and management challenges [3,4]. Distinguishing normal post-operative inflammation from early infection or thrombosis remains a critical yet difficult task, particularly in the first few weeks after surgery when routine laboratory parameters are physiologically elevated [5].
Role of serum biomarkers
Serum D-dimer, C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR) are valuable yet non-specific indicators of post-operative response. D-dimer reflects fibrin degradation and activation of the coagulation-fibrinolytic cascade. Elevated levels occur after major surgery, trauma, infection, or thrombosis [5]. CRP is an acute-phase reactant synthesized by hepatocytes under interleukin-6 stimulation; it rises within 6–8 h after tissue injury, peaks around 48–72 h, and typically normalizes within 3–4 weeks [6]. ESR increases more gradually, peaking between post-operative days 5–7, and may remain elevated for several weeks due to its dependence on plasma fibrinogen and erythrocyte aggregation [7]. Together, these biomarkers provide insight into the magnitude and course of post-operative inflammatory and coagulative responses. However, interpreting these values requires caution. Overreacting to physiologic post-operative elevations may result in unnecessary antibiotic or anticoagulant therapy, prolonged hospitalization, and increased healthcare costs [8].
Rationale and knowledge gap
Existing studies from Western populations have established general patterns for post-operative D-dimer, ESR, and CRP fluctuations. Yet baseline inflammatory profiles differ across populations due to genetic, dietary, and environmental factors [9,10]. In India, limited literature defines the normal post-operative kinetics of these biomarkers following uncomplicated arthroplasty. Establishing reference trends can improve diagnostic precision and avoid misinterpretation of laboratory findings in the early recovery period.
Aim
To evaluate serial post-operative changes in serum D-dimer, ESR, and CRP after total hip and knee arthroplasty, define their normal physiological trajectories, and determine their diagnostic and prognostic relevance in uncomplicated cases.
Study design and setting
This was a prospective observational study conducted in the Department of Orthopaedics and Trauma Centre, J.A. Group of Hospitals, G.R. Medical College, Gwalior (M.P.), from October 2022 to June 2024. The study aimed to evaluate post-operative variations in serum biomarkers – D-dimer, ESR, and CRP – among patients undergoing primary total hip and knee arthroplasty [11].
Ethical approval
The protocol was approved by the Institutional Ethics Committee of Gajara Raja Medical College, Gwalior (IEC Approval No. 65/IEC-GRMC/2022, dated 01 September 2022). All procedures followed the Declaration of Helsinki (2013 revision), and written informed consent was obtained from all participants before inclusion [12].
Sample size and population
A total of 50 patients aged ≥50 years were enrolled: 25 total hip arthroplasty (THA) cases and 25 total knee arthroplasty (TKA) cases. Inclusion criteria: Age ≥50 years, elective primary arthroplasty for degenerative or post-traumatic arthritis, patients fit for surgery, and consenting to serial post-operative sampling. Exclusion criteria: Active infection, VTE, or metabolic bone disease, chronic inflammatory or autoimmune disorders, abnormal baseline ESR, CRP, or D-dimer values, revision arthroplasty, or major systemic illness.
Parameters assessed
Venous blood samples were obtained pre-operatively and on post-operative days 1, 3, 5, 7, 14, and 28 for serial biochemical analysis. Serum D-dimer was quantified using an enzyme-linked immunosorbent assay-based immunoturbidimetric method [13] on the Cobas 6000 Analyzer. CRP levels were determined through a quantitative turbidimetric immunoassay using the Beckman Coulter AU480 Analyzer. The ESR [14] was measured manually by Wintrobe’s method, following standard laboratory procedures. Total leukocyte count (TLC) was assessed with an automated hematology analyzer. Serum sodium and calcium concentrations were evaluated via the ion-selective electrode technique on the Siemens Dimension EXL 200 Analyzer [15]. All biochemical analyses were performed in the Central Biochemistry Laboratory of G.R. Medical College and J.A. Group of Hospitals, Gwalior, under standardized protocols to ensure consistency and accuracy.
Data analysis
Data were entered into Microsoft Excel and analyzed using Statistical Package for Social Sciences v25 (IBM Corp., USA). Continuous variables were expressed as mean ± standard deviation. Temporal patterns were analyzed descriptively, focusing on serial variation trends rather than hypothesis testing [16].
Demographic profile
Among 50 patients, 25 underwent THA and 25 TKA. The mean age was 58.6 ± 7.2 years (range 50–72 years), with 28 males (56%) and 22 females (44%).
Age and gender distribution
Most participants were between 51 and 60 years (44%), followed by 61–70 years (36%) (Table 1). Males (n = 28) were slightly more than females (n = 22). Age- and gender-wise distribution of patients undergoing arthroplasty is depicted in a bar diagram in Fig. 1 [17].
D-dimer levels
Serum D-dimer demonstrated a biphasic post-operative trend – an initial sharp rise within 24 h (≈ 8.6- fold), a trough by day 3, and a smaller secondary rise by day 10–14 before normalization around week 4 (Table 2). No patient developed thromboembolic complications [18,19,20].
CRP and ESR
CRP showed a sharp increase after surgery, peaking on Day 3 (~205 mg/L) (Table 3), while ESR peaked later on Day 5 (~68 mm/h) (Table 4). Both markers declined gradually thereafter, with CRP approaching baseline by the 4th post-operative week [21,22,23] and ESR slightly above pre-operative values. Comparative post-operative trends of CRP and ESR following arthroplasty can be seen as shown in Fig. 2 [24].
TLC
A transient physiological rise in TLC was noted on post-operative Day 1 (≈ 11.8 × 109/L), followed by normalization by Day 5, consistent with acute inflammatory response [25] (Table 5).
Serum electrolytes
Mild transient hyponatremia (Na⁺ 130–134 mmol/L) occurred in 6 (12%) patients (Table 6), resolving spontaneously without neurological symptoms [26]. Serum calcium levels remained stable and within normal limits throughout follow-up (Table 7).
Post-operative inflammatory and coagulative responses are complex physiological reactions influenced by surgical trauma, blood loss, and tissue remodeling. Biomarkers, such as D-dimer, ESR, and CRP serve as essential tools for differentiating normal post-operative recovery from pathological processes, such as infection and thrombosis [27]. In the present study, all 50 patients demonstrated predictable, self-limiting alterations in these biomarkers following uncomplicated total hip and knee arthroplasty. No patient developed deep vein thrombosis (DVT), pulmonary embolism, or PJI, confirming that observed changes represented physiological variations rather than complications [28].
D-dimer as a key post-operative biomarker
D-dimer is a degradation product of cross-linked fibrin and a sensitive indicator of fibrinolytic activity. In this study, serum D-dimer exhibited a biphasic pattern: An initial sharp rise within 24 h, a partial decline by Day 3, and a secondary mild elevation around Days 10–14. This pattern aligns with findings from multiple studies that identified two post-operative peaks corresponding to intraoperative coagulation and subsequent tissue healing. Shahi et al. reported that D-dimer typically peaks on Day 1 and again on Days 10–14 after TKA, even in the absence of thrombosis [18]. Similarly, older studies observed biphasic kinetics with early coagulation activation and a second wave due to fibrinolysis during wound healing [19]. The normalization of D-dimer by Day 28 in the present study supports its transient nature and physiological relevance. A recent meta-analysis confirmed that post-operative D-dimer levels may remain elevated for up to 14 days without indicating thrombosis [20]. These findings emphasize that a high D-dimer in the first 2–3 weeks after arthroplasty should not be considered diagnostic of VTE unless accompanied by symptoms or imaging evidence [21]. Misinterpretation can lead to unnecessary anticoagulation and bleeding risk. Our study, therefore, supports the concept of context-based interpretation rather than fixed cutoff values. Diagnostic Relevance of D-dimer in infection: Beyond thrombosis, D-dimer has gained attention as a potential marker for prosthetic joint infection. Saleh et al. reported significantly higher D-dimer levels in infected versus aseptic revision arthroplasties [10]. In studies, it was confirmed that combining D-dimer with CRP improved the diagnostic sensitivity for PJI to 89% compared with CRP alone [22]. Because our cohort comprised only uncomplicated cases, the data provide a baseline reference curve that can guide future comparative infection-focused studies.
CRP and ESR: Markers of post-operative inflammation
Both CRP and ESR are well-established inflammatory markers; however, their kinetics differ substantially. CRP peaked on post-operative day 3 and normalized by week 4, whereas ESR peaked later (day 5) and declined more slowly. This staggered pattern aligns with contemporary reports by older studies [7,16]. CRP’s short half-life (~19 h) explains its rapid rise and fall, making it more reliable for early detection of post-operative infection, whereas ESR is useful for long-term monitoring of resolution [23]. A persistently rising or secondarily elevated CRP after day 5, or an ESR that continues to increase beyond the 2nd week, should prompt evaluation for PJI. Our results, showing uniform decline after expected peaks, confirm normal inflammatory recovery.
Integration of biomarker patterns
When considered together, these biomarkers provide complementary insights into the patient’s post-operative trajectory. D-dimer reflects coagulation-fibrinolytic activity. CRP signifies hepatic acute-phase response. ESR correlates with plasma fibrinogen and chronic inflammatory state. Their combined interpretation allows differentiation between normal post-operative response and potential complications [25]. In studies, it was emphasized on the importance of a “biomarker profile approach” rather than relying on isolated parameters [24]. Similarly, it was demonstrated that D-dimer combined with CRP improved sensitivity and specificity for early infection detection compared with either marker alone [25]. The present study contributes to this growing body of evidence by defining baseline post-operative trajectories for these biomarkers in Indian patients-information that was previously lacking in regional literature.
Electrolyte and hematological trends
Post-operative leukocytosis peaking on day 1 is a well-documented physiological stress response mediated by catecholamine surge [26]. The quick return to baseline by day 5 distinguishes it from infectious leukocytosis. Mild, transient hyponatremia observed in 12% of cases was clinically insignificant, consistent with perioperative fluid shifts and stress-related antidiuretic hormone release [26]. Similar trends have been noted in the analysis of early post-operative biochemical changes [28].
Clinical implications
Understanding the normal pattern of these biomarkers offers several advantages [29,30]: Improved diagnostic accuracy for early detection of PJI and thromboembolism, avoidance of unnecessary antibiotic or anticoagulant use, reducing cost and iatrogenic risks, and establishment of reference trajectories for future comparative studies, especially in the Indian subcontinent. Guidance for post-operative follow-up scheduling, as normalization times are predictable and reproducible.
Limitations
The study was observational and limited by a moderate sample size (n = 50) and a single-center design. Advanced diagnostic imaging, such as venography or Doppler, was not routinely used to confirm subclinical thromboembolism. In addition, the study did not include cases with post-operative infection or DVT, so biomarker differentiation in such scenarios could not be directly assessed. Larger multicentric trials, including complicated cases are needed for threshold validation.
Future scope
Future multicentric studies should include both uncomplicated and complicated cases to establish thresholds distinguishing physiological versus pathological elevations. In addition, inclusion of other markers, such as fibrinogen, interleukin-6, and procalcitonin could provide a more comprehensive post-operative biomarker panel [30].
Learning points
D-dimer rises sharply within 24 h, shows a mild secondary elevation around 10–14 days, and normalizes by 4 weeks after uncomplicated arthroplasty, CRP peaks at day 3 and ESR at day 5, reflecting sequential inflammatory responses, awareness of these normal trajectories prevents misdiagnosis of infection or thrombosis in the early post-operative period, serial combined interpretation of D-dimer + CRP + ESR improves specificity over any single marker and establishing population- specific reference curves is essential for accurate post-operative assessment in Indian patients.
Serum biomarkers demonstrate predictable and self-limiting post-operative trends following uncomplicated total hip and knee arthroplasty. D-dimer exhibits an early and secondary post-operative rise reflecting activation of coagulation and fibrinolysis, while CRP peaks around day 3 and ESR around day 5, both declining progressively thereafter. The absence of thromboembolic or infectious events confirms that these variations represent normal physiological recovery rather than pathological processes. Understanding these reference trajectories enables clinicians to differentiate expected post-operative inflammation from early PJI or VTE, thereby avoiding unnecessary antibiotic or anticoagulant use. This study establishes population-specific baseline data for Indian patients and highlights D-dimer as the most dynamic early indicator, complemented by CRP and ESR for subsequent monitoring and clinical decision-making.
Post-operative elevations of D-dimer, CRP, and ESR following uncomplicated total hip and knee arthroplasty represent predictable physiological responses rather than pathology. Awareness of their normal temporal patterns – particularly the early and secondary rise of D-dimer and the staggered peaks of CRP and ESR – enables clinicians to distinguish routine post-operative inflammation from early infection or thromboembolism. Serial, combined interpretation of these biomarkers can prevent unnecessary investigations and treatment while supporting safe, evidence-based post-operative decision-making.
References
- 1. Singh JA, Yu S, Chen L, Cleveland JD. Rates of total joint replacement in the United States: Futureprojections to 2040. J Rheumatol 2020;47:341-8. [Google Scholar] [PubMed]
- 2. Pivec R, Johnson AJ, Mears SC, Mont MA. Hip arthroplasty. Lancet 2012;380:1768-77. [Google Scholar] [PubMed]
- 3. Parvizi J, Gehrke T. Definition of periprosthetic joint infection. J Arthroplasty 2018;33:1331-4. [Google Scholar] [PubMed]
- 4. Love C, Tomas MB, Marwin SE, Pugliese PV, Palestro CJ. Role of nuclear medicine in diagnosis of the infected joint replacement. Radiographics 2001;21:1229-38. [Google Scholar] [PubMed]
- 5. Bytniewski P, Machała W, Romanowski L, Wiśniewski W, Kosowski K. The dynamics of D-dimer level fluctuation in patients after the cemented and cementless total hip and total knee replacement. J Orthop Surg Res 2014;10:89. [Google Scholar] [PubMed]
- 6. Sereda AP, Rukina AN, Trusova YV, Dzhavadov AA, Cherny AA, Bozhkova SA, et al. Dynamics of C-reactive protein level after orthopedic surgeries. J Orthop 2023;47:1-7. [Google Scholar] [PubMed]
- 7. Bilgen Ö, Atici T, Durak K, Karaeminoğullari O, Bilgen M. C-reactive protein values and ESR in total knee arthroplasty. Acta Orthop Belg 2020;86:645-52. [Google Scholar] [PubMed]
- 8. Ali KA, He L, Deng X, Pan J, Huang H, Li W. Assessing the predictive value of pre- and post-operative inflammatory markers in patients undergoing total knee arthroplasty. J Orthop Surg Res 2024;30:614. [Google Scholar] [PubMed]
- 9. Incesoy MA, Demirkiran CB, Kaya HB, Geckalan MA, Tak AY, Elmali N, et al. Natural course of postoperative C-reactive protein and erythrocyte sedimentation rate in unilateral and simultaneous bilateral total knee arthroplasty. BMC Musculoskelet Disord 2025;26:260. [Google Scholar] [PubMed]
- 10. Saleh A, George J, Faour M, Klika AK, Higuera CA. Serum biomarkers in periprosthetic joint infections . Bone Joint Res 2018;7:85-93. [Google Scholar] [PubMed]
- 11. Lee YS, Lee YK, Han SB, Nam CH, Parvizi J, Koo KH. Natural progress of D-dimer following total joint arthroplasty: A baseline for the diagnosis of the early postoperative infection. J Orthop Surg Res 2018;13:36. [Google Scholar] [PubMed]
- 12. Cutter B, Lum ZC, Giordani M, Meehan JP. Utility of D-dimer in total joint arthroplasty. World J Orthop 2023;14:90-102. [Google Scholar] [PubMed]
- 13. Ramadanov N, Marinova-Kichikova P, Hable R, Dimitrov D, Becker R. Comparison of postoperative serum biomarkers after total hip arthroplasty through minimally invasive versus conventional approaches: A systematic review and meta-analysis of randomized controlled trials. Prosthesis 2023;5:694-710. [Google Scholar] [PubMed]
- 14. Sadiq KI, Abdulzahra MA, Jaffar RM. Variations of inflammatory markers levels (ESR and CRP) in the perioperative period of total knee arthroplasty. Iraqi Nat J Med 2024;6:73-7. [Google Scholar] [PubMed]
- 15. Deirmengian GK, Zmistowski B, Jacovides C, O’Neil J, Parvizi J. Leukocytosis is common after total hip and knee arthroplasty. Clin Orthop Relat Res 2011;469:3031-6. [Google Scholar] [PubMed]
- 16. Mertens MT, Singh JA. Biomarkers in arthroplasty: A systematic review. Open Orthop J 2011;16:92-105. [Google Scholar] [PubMed]
- 17. Shih LY, Wu JJ, Yang DJ. Erythrocyte sedimentation rate and C-reactive protein values in patients with total hip arthroplasty. Clin Orthop Relat Res 1987;225;238-46. [Google Scholar] [PubMed]
- 18. Shahi A, Kheir MM, Tarabichi M, Hosseinzadeh HR, Tan TL, Parvizi J. Serum D-dimer test is promising for the diagnosis of periprosthetic joint infection and timing of reimplantation. J Bone Joint Surg 2017;99:1419-27. [Google Scholar] [PubMed]
- 19. Chen CJ, Wang CJ, Huang CC. The value of D-dimer in the detection of early deep-vein thrombosis after total knee arthroplasty in Asian patients: A cohort study. Thromb J 2008;6:5. [Google Scholar] [PubMed]
- 20. Kim YH, Kim JS. Incidence and natural history of deep-vein thrombosis after total knee arthroplasty. A prospective, randomised study. J Bone Joint Surg Br 2002;84:566-70. [Google Scholar] [PubMed]
- 21. Mercurio M, Galasso O, Familiari F, Iannò B, Bruno CF, Castioni D, et al. Trend of perioperative CRP (C-reactive protein) levels in non-infected total knee arthroplasty. Orthop Rev (Pavia) 2022;14:36589. [Google Scholar] [PubMed]
- 22. Qin L, Li F, Gong X, Wang J, Huang W, Hu N. Combined measurement of D-dimer and C-reactive protein levels: Highly accurate for diagnosing chronic periprosthetic joint infection. J Arthroplasty 2020;35:229-34. [Google Scholar] [PubMed]
- 23. Parvizi J, Della Valle CJ. AAOS clinical practice guideline: Diagnosis and treatment of periprosthetic joint infections of the hip and knee. J Am Acad Orthop Surg 2010;18:771-2. [Google Scholar] [PubMed]
- 24. He T, Wu W, Huang Y, Zhang X, Tang T, Dai K. Multiple biomarkers analysis for the early detection of prosthetic aseptic loosening of hip arthroplasty. Int Orthop 2013;37:1025-31. [Google Scholar] [PubMed]
- 25. Arabmotlagh M, Sabljic R, Rittmeister M. Changes of the biochemical markers of bone turnover and periprosthetic bone remodeling after cemented hip arthroplasty. J Arthroplasty 2006;21:129-34. [Google Scholar] [PubMed]
- 26. Hughes SF, Hendricks BD, Edwards DR, Maclean KM, Bastawrous SS, Middleton JF. Total hip and knee replacement surgery results in changes in leukocyte and endothelial markers. J Inflamm (Lond) 2010;7:2. [Google Scholar] [PubMed]
- 27. Hennrikus E, Georgeson A, Leymeister K, Mucha S, McGillen B, Miller R. Defining the cause of post-operative hyponatremia in the orthopedic patient. Int J Clin Med 2016;7:668-74. [Google Scholar] [PubMed]
- 28. Wu XD, Zhu ZL, Xiao PC, Liu JC, Wang JW, Huang W. Are routine postoperative laboratory tests necessary after primary total hip arthroplasty? J Arthroplasty 2020;35:2892-8. [Google Scholar] [PubMed]
- 29. Wu XD, Xiao PC, Zhu ZL, Liu JC, Li YJ, Huang W. The necessity of routine postoperative laboratory tests in enhanced recovery after surgery for primary hip and knee arthroplasty: A retrospective cohort study protocol. Medicine 2019;98:e15513. [Google Scholar] [PubMed]
- 30. Fernandez-Sampedro M, Sanlés-González I, García-Ibarbia C, Fañanás-Rodríquez N, Fakkas-Fernández M, Fariñas MC. The poor accuracy of D-dimer for the diagnosis of prosthetic joint infection but its potential usefulness in early postoperative infections following revision arthroplasty for aseptic loosening. BMC Infect Dis 2022;22:91. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Clinico-Laboratory Correlates of Inflammatory Markers in Elderly Knee Osteoarthritis
February 1, 2026 Clinico-Laboratory Correlates of Inflammatory Markers in Elderly Knee Osteoarthritis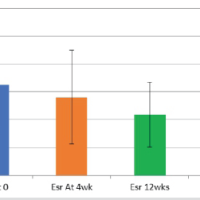 April 1, 2025 Effect of DMARD Therapy on Inflammatory Biomarkers and Disease Activity in Rheumatoid Arthritis Patients
April 1, 2025 Effect of DMARD Therapy on Inflammatory Biomarkers and Disease Activity in Rheumatoid Arthritis Patients January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty
January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty December 1, 2025 Superior Gluteal Artery Perforation Following Girdlestone Resection Arthroplasty: A Case Report
December 1, 2025 Superior Gluteal Artery Perforation Following Girdlestone Resection Arthroplasty: A Case Report