
Early closed reduction under adequate anesthesia remains the cornerstone of management for peritalar dislocation. A systematic approach, including immediate imaging, atraumatic reduction, temporary stabilization, and structured physiotherapy, is essential to achieve full recovery and minimize sequelae.
Dr. Touré Layes, Orthopaedic and Trauma Surgery, Bocar Sidi Sall Teaching Hospital, Kati, Mali. E-mail: layestoure854@gmail.com
Introduction: Peritalar dislocation is a rare injury involving simultaneous disruption of the talocalcaneal and talonavicular joints, usually following high-energy trauma. Early recognition and management are crucial to prevent chronic instability, stiffness, or post-traumatic osteoarthritis. We report a case of peritalar dislocation in a 48-year-old patient.
Case Report: A 48-year-old male sustained an isolated medial peritalar dislocation of the right foot after a road traffic accident. Clinical examination revealed medial displacement with a prominent talar head palpable through a submalleolar laceration. Radiographs confirmed the diagnosis. Under general anesthesia, closed reduction using the boot-puller maneuver was performed, followed by temporary transarticular K-wire fixation and below-knee cast immobilization for 6 weeks. Rehabilitation began after cast removal. At 6-month follow-up, the patient achieved full ankle and foot mobility, pain-free walking, and no signs of instability or complications.
Conclusion: Medial peritalar dislocations are uncommon but potentially disabling. Prompt diagnosis, gentle closed reduction, temporary stabilization, and supervised rehabilitation are essential for excellent functional outcomes.
Keywords: Peritalar dislocation, medial dislocation, subtalar dislocation, foot trauma.
Peritalar dislocation is defined as the simultaneous loss of normal contact between the talocalcaneal and talonavicular joints [1,2]. Peritalar dislocations are rare injuries, representing approximately 1% of all traumatic foot injuries and 1–2% of all joint dislocations. The medial form is the most common. They usually occur following high-energy trauma such as road traffic accidents or falls from height [3]. The diagnosis is established clinically and confirmed by standard radiographs. Stiffness and post-traumatic osteoarthritis are the most serious long-term complications. We report a case of peritalar dislocation in a 48-year-old patient.
A 48-year-old man was the victim of a road traffic accident involving a head-on collision between his motorcycle and a parked truck. During the impact, forced plantar flexion of the right foot occurred while braking, resulting in acute pain and complete functional impairment of the right foot and ankle. He was admitted to the emergency department within 4 h of the trauma. On arrival, he was hemodynamically stable and fully conscious. Initial clinical examination revealed a deformity of the right ankle in varus, associated with an anterolateral, arc-shaped submalleolar skin laceration measuring 8 cm in length, partially exposing the talar head (Fig. 1).

Figure 1: Clinical presentation of the right foot at admission. (a) Medial displacement of the right foot with varus deformity and (b) prominent talar head visible through a submalleolar laceration measuring approximately 8 cm.
Distal vascular examination showed palpable posterior and anterior tibial pulses. Sensory and motor function of the toes were preserved. Standard anteroposterior and lateral radiographs of the ankle demonstrated a medial peritalar dislocation (Fig. 2).

Figure 2: Preoperative radiographs of the right foot. (a) Standard anteroposterior and (b) lateral radiographs demonstrating isolated medial peritalar dislocation without associated fractures.
Under general anesthesia, thorough irrigation and debridement of the wound were performed, followed by closed reduction of the dislocation using the boot-puller maneuver (Fig. 3).

Figure 3: Clinical presentation after reduction. (a and b) Intraoperative photographs showing the boot-puller maneuver used to achieve closed reduction of the medial peritalar dislocation and close the wound.
The reduction was stabilized with transarticular Kirschner wires across the talocalcaneal and talonavicular joints (Fig. 4).

Figure 4: Post-operative radiographs. (a) Lateral views of ankle showed perfect reduction stabilized with k-wire and (b) Anteroposterior view of the right ankle.
The ankle was immobilized in a below-knee plaster cast for 6 weeks without weight-bearing. Wound healing was achieved by day 12, and post-operative recovery was uneventful. The K-wires were removed at 6 weeks, followed by a structured rehabilitation program. At 6-month follow-up, the patient had regained a full range of motion in flexion and extension (Fig. 5), and control radiographs showed a congruent reduction with no signs of necrosis or degenerative changes (Fig. 6).

Figure 5: Functional outcomes at 6 months. Functional outcomes at 6 months showed (a) plantar flexion of right ankle and (b) extension of ankle.
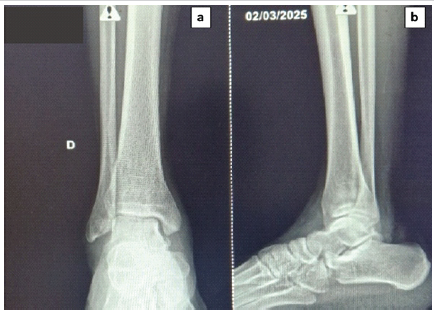
Figure 6: Follow-up radiographs at 6 months. (a) Standard anteroposterior and (b) lateral radiographs confirming maintained reduction and absence of secondary dislocation or post-traumatic osteoarthritis.
As in our clinical case, most peritalar dislocations occur in young or middle-aged adults following high-energy trauma, most commonly road traffic accidents [4]. In our patient, the mechanism involved a sudden braking maneuver that induced forced plantar flexion and inversion of the foot. Medial peritalar dislocation results from excessive inversion in which the strong calcaneonavicular (spring) ligament resists rupture, while the transmitted force disrupts the weaker interosseous talocalcaneal and calcaneocuboid ligaments. This mechanism leads to an en bloc medial displacement of the calcaneus, navicular, and the entire distal segment of the foot relative to the talus [4,5]. Several clinical forms of peritalar dislocation have been described: the medial type accounts for approximately 80% of cases, the lateral type for 17%, and the anterior and posterior variants for the remaining 3% [5]. Clinically, the deformity is often pathognomonic. In our case, the right foot was displaced medially, with a prominent talar head palpable on the dorsolateral aspect through the wound – findings consistent with the description of the medial form in the literature [2]. Early diagnosis is critical, and standard radiographs (anteroposterior and lateral) generally suffice. However, computed tomography scans may be necessary in complex or open injuries to identify associated fractures or intra-articular fragments [3]. In our case, the diagnosis was promptly made by plain radiography, which allowed early management. Emergency reduction is the cornerstone of treatment. It should be performed under general or regional anesthesia to facilitate muscle relaxation and avoid iatrogenic damage to articular cartilage. The boot-puller maneuver used in our patient is a simple and effective technique that restores alignment through gentle traction and reversal of the deforming forces. Once reduction is achieved, transarticular K-wire fixation provides temporary stabilization, preventing redislocation while soft-tissue healing occurs. Immobilization in a below-knee cast for 6 weeks remains standard to ensure adequate capsuloligamentous healing and to prevent chronic instability or recurrent subluxation. Early physiotherapy after cast removal is essential for functional recovery and to limit stiffness. The presence of a skin laceration in this case reflects the high-energy nature of the trauma. Associated injuries – particularly fractures of the malleoli, talus, or navicular – are reported in 20–30% of cases
As described in the literature, peritalar/subtalar dislocations often occur after high-energy trauma and are frequently associated with fractures of the foot and ankle, including those of the talus, malleoli, or navicular bone. [5 In open injuries, meticulous debridement is imperative to prevent infection, one of the most feared complications alongside post-traumatic osteoarthritis [3]. Osteoarthritis typically manifests as intermittent pain, especially when walking on uneven ground or during weather changes. Post-traumatic osteoarthritis following subtalar dislocation is a well-documented risk, often associated with intermittent pain and clinical symptoms during walking or daily activities [7,9,10]. At 6-month follow-up, our patient demonstrated a satisfactory functional outcome, characterized by pain-free walking and complete recovery of ankle and foot mobility. These favorable results emphasize the importance of early reduction, stable fixation, adequate immobilization, and supervised rehabilitation in optimizing outcomes for this rare but severe injury.
Peritalar dislocations are uncommon injuries that typically follow high-energy trauma. Early diagnosis, urgent reduction, and stable fixation are essential to restore anatomical alignment and prevent long-term complications such as instability or post-traumatic osteoarthritis. A prompt, well-executed orthopedic management protocol can lead to excellent functional recovery, even in open injuries.
Peritalar dislocation is a rare but serious injury that requires prompt recognition and urgent reduction to restore joint congruency and prevent long-term complications such as stiffness, avascular necrosis, and post-traumatic osteoarthritis. Early diagnosis based on careful clinical examination and plain radiographs, followed by stable immobilization and supervised rehabilitation, can yield excellent functional outcomes even in high-energy trauma.
References
- 1. Veltman ES, Steller EJ, Wittich P, Keizer J. Lateral subtalar dislocation: Case report and review of the literature. World J Orthop 2016;7:623-7. [Google Scholar] [PubMed]
- 2. Wang HY, Wang BB, Huang M, Wu XT. Treatment of closed subtalar joint dislocation: A case report and literature review. Chin J Traumatol 2020;23:367-71. [Google Scholar] [PubMed]
- 3. Prada-Cañizares A, Auñón-Martín I, Rico JV, Pretell-Mazzini J. Subtalar dislocation: Management and prognosis for an uncommon orthopaedic condition. Int Orthop 2016;40:999-1007. [Google Scholar] [PubMed]
- 4. Camarda L, Abruzzese A, La Gattuta A, Lentini R, D’Arienzo M. Results of closed subtalar dislocations. Musculoskelet Surg 2016;100:63-9. [Google Scholar] [PubMed]
- 5. Melenevsky Y, Mackey RA, Abrahams RB, Thomson NB 3rd. Talar fractures and dislocations: A radiologist’s guide to timely diagnosis and classification. Radiographics 2015;35:765-79. [Google Scholar] [PubMed]
- 6. Ruhlmann F, Poujardieu C, Vernois J, Gayet LE. Isolated acute traumatic subtalar dislocations: Review of 13 cases at a mean follow-up of 6 years and literature review. J Foot Ankle Surg 2017;56:201-7. [Google Scholar] [PubMed]
- 7. Yung KS, Kwok HM, Pan NY, Lo BA. Acute traumatic subtalar dislocation: a rare but important clinical entity with 15-year retrospective radiological analysis of 23 cases. J Clin Imaging Sci. 2024;14:30. [Google Scholar] [PubMed]
- 8. Jlidi M, Bouaicha W, Gharbi MH, Mallek K, Jaziri S, Sbaihi S, Daas S. Unusual case of lateral subtalar joint dislocation associated with calcaneal fracture and lateral malleolus fracture. Trauma Case Rep. 2023;47:100897. [Google Scholar] [PubMed]
- 9. McKeag P, Lyske J, Reaney J, Thompson N. Subtalar dislocation secondary to a low energy injury. BMJ Case Rep 2015;2015:bcr2014-208828. [Google Scholar] [PubMed]
- 10. Ruhlmann F, Poujardieu C, Vernois J, Gayet LE. Isolated acute traumatic subtalar dislocations: review of 13 cases at a mean follow-up of 6 years and literature review. J Foot Ankle Surg. 2017 Jan-Feb;56(1):201-207. doi:10.1053/j.jfas.2016.01.044. PMID:26947001. [Google Scholar] [PubMed] [CrossRef]





Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2024 A Rare Case of a Medial Peritalar Dislocation on a Rock Climber
September 1, 2024 A Rare Case of a Medial Peritalar Dislocation on a Rock Climber June 29, 2021 Filling Bone Defects after Hip Arthroplasty Revision Using Hydroxyapatite/β-tricalcium Phosphate: A Case Report with Long-term Result
June 29, 2021 Filling Bone Defects after Hip Arthroplasty Revision Using Hydroxyapatite/β-tricalcium Phosphate: A Case Report with Long-term Result September 1, 2025 A Race against Time: Managing Acute Unstable Slipped Capital Femoral Epiphysis in a 15-year old with Normal Body Mass Index using the Modified Dunn’s Procedure – A Case Report
September 1, 2025 A Race against Time: Managing Acute Unstable Slipped Capital Femoral Epiphysis in a 15-year old with Normal Body Mass Index using the Modified Dunn’s Procedure – A Case Report June 10, 2023 Well-Leg Compartment Syndrome Due to Hemilithotomy Positioning after Arthroscopic Reconstruction of the PCL
June 10, 2023 Well-Leg Compartment Syndrome Due to Hemilithotomy Positioning after Arthroscopic Reconstruction of the PCL