
Total hip arthroplasty in above-knee amputees demands customized, meticulously planned pre-operative assessment, intraoperative stump control, and fixation strategies, rehabilitation protocol to address unique anatomical and biomechanical challenges for optimal functional recovery.
Dr. Mantu Jain, Department of Orthopaedics, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India. E-mail: montu_jn@yahoo.com
Introduction: With improved survival rates and functional outcomes, amputees are increasingly presenting with degenerative hip pathology requiring total hip arthroplasty (THA). However, THA in patients with ipsilateral lower limb amputation poses unique anatomical, biomechanical and technical challenges, and current surgical training often lacks specific technical insights for these complex cases. The literature remains limited, with few reports detailing technical strategies and rehabilitative measures in this patient population. This report aims to contribute to the existing knowledge by highlighting key pre-operative, operative and rehabilitative considerations in THA following transfemoral amputation.
Case Report: A male in his early 30s, with left above-knee amputation following trauma 3 years prior, developed progressive left hip pain impairing prosthetic ambulation. Radiographs revealed advanced osteoarthritis with femoral head collapse and retained internal fixation hardware. Pre-operative assessment included full-length femur imaging and bone density evaluation, confirming adequate bone stock. An uncemented total hip replacement was performed via a modified lateral approach. Intraoperative control of the femoral stump was achieved with a Steinmann pin inserted in the distal femur, facilitating dislocation and stem positioning without compromising fixation. Post-operatively, rehabilitation emphasized strengthening hip flexors, extensors, abductors, and adductors, with weight-bearing deferred until soft tissue healing permitted prosthetic fitting. By 3 months, the patient resumed independent ambulation with the prosthesis. Follow-up imaging at 6 months showed stable implant integration. The Harris Hip Score improved from 30 pre-operatively to 70 post-operatively.
Conclusion: THA in above-knee amputees requires meticulous preoperative planning, including detailed imaging and bone quality evaluation, alongside tailored intraoperative techniques, such as traction pin use for stump control. Implant fixation strategy must consider residual femur morphology, and rehabilitation should be customized to overcome specific muscular deficits. With comprehensive management, favorable functional outcomes and prosthetic gait restoration can be achieved in this challenging patient population.
Keywords: Total hip arthroplasty, above-knee amputation, rehabilitation.
Above-knee amputation (AKA) has been linked to a greater risk of advanced osteoarthritis and osteopenia in the residual limb compared to below-knee amputation [1,2,3,4]. These patients are also predisposed to complications in the thigh region, including hip flexion and abduction contractures, heterotopic ossification, muscular atrophy of the residual limb, and skin breakdown at the stump [5,6]. These factors collectively pose significant challenges during total hip arthroplasty (THA), such as difficulty in achieving hip dislocation, controlling the residual limb, and accurately positioning the femoral component due to the absence of the knee and tibia. A short osteoporotic stump with a wide medullary canal further complicates implant fixation and increases the risk of intraoperative fracture. In addition, the surgical site’s proximity to the distal stump heightens the potential for post-operative infection. Functional recovery, including gait restoration and prosthesis use, is often hindered by altered biomechanics and muscle atrophy [7,8]. Addressing these challenges necessitates comprehensive preoperative assessment, meticulous surgical planning – including the approach, implant selection, techniques to control stump, draping strategy, and infection prevention – and a structured rehabilitation program targeting atrophied muscles.
A male patient in his early 30s presented with progressively worsening left hip pain over the past 6 months, significantly limiting his mobility and ability to bear weight through his prosthetic limb. Three years earlier, he had sustained multiple injuries in a high-impact road traffic accident, necessitating a low AKA on the left side. At that time, he also sustained a fracture of the ipsilateral femoral neck, for which he underwent safe surgical dislocation and internal fixation using headless screws. Post-operatively, he achieved initial recovery and was ambulatory with a prosthesis. However, over time, he developed a persistent, dull ache in the left hip, which intensified and became disabling. On examination, the stump was well-healed with no signs of infection or contracture, but notable gluteal muscle wasting and severe, painful restriction in hip range of motion were present. Pelvic radiographs demonstrated advanced arthritis of the left hip (Tönnis Grade 3), with femoral head collapse and retained headless screws in situ (Fig. 1). Pre-operative functional assessment using the Harris hip score (HHS) was 30, indicating severe disability [9].

Figure 1: Pre-operative radiograph.
A full-length radiograph of the residual stump was obtained for templating. The residual stump was long with minimal thinning of the cortices and widening of the medullary cavity. Non-contrast computed tomography of the pelvis was done to rule out any heterotopic ossification. A DEXA scan of the proximal femur region ruled out osteoporosis. Other basic pre-operative and infective workup revealed no significant abnormality.
The procedure was performed via a lateral (modified Hardinge) approach to the hip, with the patient positioned in the lateral decubitus position (Fig. 2).

Figure 2: Lateral decubitus position.
Intraoperative manipulation of the femur and hip dislocation was facilitated using a 6 mm Steinmann pin inserted into the lateral distal femur, providing leverage while minimizing interference with femoral stem placement in the medullary canal (Fig. 3 and 4). An uncemented 48 mm acetabular cup, a size 4 hydroxyapatite-coated uncemented femoral stem, and a 32 mm femoral head were implanted.

Figure 3: Steinman pin at the distal lateral femur.

Figure 4: Intra-operative manipulation by the Steinman pin.
Intraoperative stability was satisfactory. Post-operative radiographs confirmed appropriate alignment and positioning of the prosthetic components (Fig. 5).
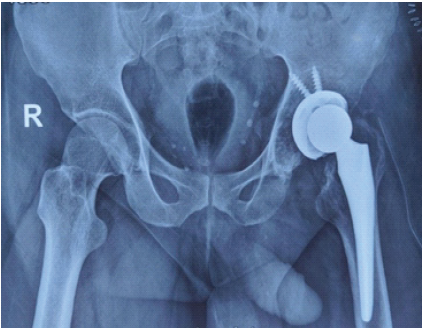
Figure 5: Immediate post-operative radiograph.
On post-operative day 2, post-dressing of the surgical site, rehabilitation commenced with a focus on strengthening exercises targeting the hip flexors, extensors, external rotators, abductors, and adductors. Weight-bearing was deferred until the surgical wound had adequately healed and residual limb swelling had subsided to permit prosthesis fitting. By post-operative day 6, the patient reported significant relief from preoperative pain and was discharged in stable condition, with advice to continue physiotherapy at home.
At the 12-week post-operative review, the patient was permitted to resume full weight-bearing with the aid of crutches and the above-knee prosthetic limb. Follow-up radiographs at 6 months demonstrated satisfactory osseointegration of the implants, with no evidence of component subsidence or osteolysis (Fig. 6). Clinically, the patient remained pain-free on the operated side and was mobilizing independently with crutches and the prosthesis. Functional outcome, as measured by the HHS, improved markedly from a pre-operative score of 30–70 at the latest follow-up.

Figure 6: Follow-up radiograph at 12 weeks.
Patients with AKAs present unique challenges that necessitate careful consideration during preoperative planning, surgical execution, and post-operative rehabilitation. Pre-operative imaging should include the entire residual femur to assess both the remaining bone stock and medullary canal dimensions, as prolonged prosthetic use may alter bone mineral density and distal femoral morphology [10,11]. Patients with reduced bone density are at a higher risk of sustaining intraoperative fractures, which can delay post-operative rehabilitation [1,12]. In such cases, cemented implants may offer advantages. In amputees, a diminished cortical area is frequently observed at the stump end, often accompanied by widening of the medullary canal. Consequently, several authors recommend the routine use of cemented components in this population to minimize fracture risk and facilitate early weight-bearing [11,13]. In our case, the patient had a long residual stump with no evident osteoporosis, widening of the canal; hence, an uncemented prosthesis was chosen. In addition, a thorough evaluation of skin integrity and soft tissue quality at the stump is crucial to minimize post-operative infection risk. Beyond standard prophylactic antibiotics, some authors recommend isolating the distal stump using sterile adhesive drapes intraoperatively, as it is often considered a potentially contaminated area due to its habitual contact with the prosthetic socket [11,14]. We covered the end of the stump with sterile adhesive drapes to maintain asepsis. Post-operatively, consistent use of appropriate stump bandaging during rehabilitation – especially when fitting the external prosthesis – is essential to reduce the risk of surgical site infection.
Post-traumatic AKAs are frequently associated with complications, such as malunited fractures, heterotopic ossification, and soft tissue contractures. These issues may necessitate surgical interventions – including soft tissue release, excision of ossified masses, or even a greater trochanteric osteotomy – to facilitate adequate exposure and enable safe dislocation of the femoral head during THA [15]. Intra-operative control of the femoral stump can be achieved through various techniques tailored to the patient’s anatomy and surgical requirements. Common methods include the use of a traction pin or bone clamp applied at the subtrochanteric level, or placement of Steinmann pins along the lateral aspect of the distal femur, ensuring they do not interfere with implant positioning [11,16,17]. In cases where the femoral stump is short, a pin may be inserted at the level of the greater trochanter [10,18,19]. Bone clamps can be positioned at the peri-trochanteric or subtrochanteric regions [20,21,22]; however, some surgeons avoid the trochanteric area due to concerns about bone fragility. In view of the long residual stump with healthy skin, soft tissues, and preserved bone mineral density in our patient, the traction pin was placed in the distal femur. This facilitated effective manipulation of the femur while preventing interference with stem insertion into the canal. Alternatively, applying a clamp at the site of gluteus maximus insertion on the femoral shaft has been described as a technique that offers effective limb manipulation while minimizing the risk of iatrogenic fracture, particularly in osteopenic bone or in the presence of prior scarring [11]. Rehabilitation protocols should be tailored to the specific anatomy and muscle involvement dictated by the level of amputation. In amputees, loss of the gastrocnemius – the primary propulsive muscle in gait – necessitates increased reliance on the remaining musculature. During stance phase on the amputated side, the hip flexors, extensors, and external rotators serve as the main power generators, while the abductors and adductors act predominantly as shock absorbers, in contrast to the contralateral limb. Accordingly, beyond the standard post-operative regimen for THA, targeted stretching of the hip flexors and knee extensors is often emphasized [13,19]. For our patient, based on our preoperative assessment, we focused on the strengthening of hip extensors, adductors, which yielded a good functional outcome.
This report demonstrates that THA can be successfully performed in above-knee amputees by prioritizing individualized preoperative planning, intraoperative control of the stump, and tailored rehabilitation. By detailing practical intraoperative strategies and focused post-operative rehabilitation, this report offers original and practical guidance for orthopedic surgeons faced with similar complex scenarios. The case not only adds to the limited literature on THA in above-knee amputees but its broader impact lies in improving functional outcomes, optimizing perioperative protocols, and advancing clinical knowledge about surgical and rehabilitative management after major limb amputation with secondary hip arthritis.
1. Total hip arthroplasty in above-knee amputees presents unique anatomical, biomechanical, and technical challenges that require meticulous preoperative planning.
2. Full-length residual femur imaging, bone density assessment, and careful evaluation of stump skin and soft tissue are essential to reduce intra- and post-operative complications.
3. Intraoperative control of the femoral stump can be optimized using techniques, such as Steinmann pins or bone clamps, adapted to stump length and bone quality.
4. Implant fixation strategy should be guided by bone stock and medullary canal morphology, with cemented components considered to reduce fracture risk and allow early mobilization.
5. Post-operative rehabilitation must be tailored to the level of amputation, focusing on compensating for lost propulsive muscles and restoring functional gait with a prosthesis.
References
- 1. Sherk VD, Bemben MG, Bemben DA. BMD and bone geometry in transtibial and transfemoral amputees. J Bone Miner Res 2008;23:1449-57. [Google Scholar] [PubMed]
- 2. Burke MJ, Roman V, Wright V. Bone and joint changes in lower limb amputees. Ann Rheum Dis 1978;37:252-4. [Google Scholar] [PubMed]
- 3. Kulkarni J, Adams J, Thomas E, Silman A. Association between amputation, arthritis and osteopenia in British male war veterans with major lower limb amputations. Clin Rehabil 1998;12:348-53. [Google Scholar] [PubMed]
- 4. Gailey R, Allen K, Castles J, Kucharik J, Roeder M. Review of secondary physical conditions associated with lower-limb amputation and long-term prosthesis use. J Rehabil Res Dev 2008;45:15-30. [Google Scholar] [PubMed]
- 5. Amtmann D, Morgan SJ, Kim J, Hafner BJ. Health-related profiles of people with lower limb loss. Arch Phys Med Rehabil 2015;96:1474-83. [Google Scholar] [PubMed]
- 6. Potter BK, Burns TC, Lacap AP, Granville RR, Gajewski DA. Heterotopic ossification following traumatic and combat-related amputations. Prevalence, risk factors, and preliminary results of excision. J Bone Joint Surg 2007;89:476-86. [Google Scholar] [PubMed]
- 7. Gottschalk FA, Stills M. The biomechanics of trans-femoral amputation. Prosthet Orthot Int 1994;18:12-7. [Google Scholar] [PubMed]
- 8. Nolan L, Lees A. The functional demands on the intact limb during walking for active trans-femoral and trans-tibial amputees. Prosthet Orthot Int 2000;24:117-25. [Google Scholar] [PubMed]
- 9. Söderman P, Malchau H. Is the harris hip score system useful to study the outcome of total hip replacement? Clin Orthop 2001;384:189-97. [Google Scholar] [PubMed]
- 10. Tripathy S, Varghese P, Khan S, Saha S. Simultaneous above-knee amputation and ipsilateral total hip arthroplasty in a neglected neck of femur fracture with an insensate limb. BMJ Case Rep 2023;16:e255085. [Google Scholar] [PubMed]
- 11. Malagelada F, Coll Rivas M, Jiménez Obach A, Auleda J, Guirao L, Pleguezuelos E. Total hip replacement in an ipsilateral above-the-knee amputation: Surgical technique, rehabilitation, and review of the literature. Int J Low Extrem Wounds 2013;12:39-43. [Google Scholar] [PubMed]
- 12. Pauley T, Devlin M, Madan-Sharma P. A single-blind, cross-over trial of hip abductor strength training to improve timed up and go performance in patients with unilateral, transfemoral amputation. J Rehabil Med 2014;46:264-70. [Google Scholar] [PubMed]
- 13. Masmoudi K, Rbai H, Fradj AB, Saâdena J, Boughattas A. Primary total hip replacement for a femoral neck fracture in a below-knee amputee. J Orthop Case Rep 2016;6:63-6. [Google Scholar] [PubMed]
- 14. Webster J, Alghamdi A. Use of plastic adhesive drapes during surgery for preventing surgical site infection. Cochrane Database Syst Rev 2015;2015:CD006353. [Google Scholar] [PubMed]
- 15. Sathappan SS, Wee J, Ginat D, Teicher M, Meere P, Di Cesare PE. Total hip arthroplasty in above-knee amputees: A case report. Am J Orthop Belle Mead NJ 40:E17-19. [Google Scholar] [PubMed]
- 16. Leonard M, Nicholson P. Total hip arthroplasty in a patient with arthrogryphosis and an ipsilateral above knee amputation. HIP Int 2010;20:559-61. [Google Scholar] [PubMed]
- 17. Boussakri H, Alassaf I, Hamoudi S, Elibrahimi A, Ntarataz P, Elmrini A, et al. Hip arthroplasty in a patient with transfemoral amputation: A new tip. Case Rep Orthop 2015;2015:1-5. [Google Scholar] [PubMed]
- 18. Diamond OJ, Mullan CJ, McAlinden MG, Brown JG. Total hip arthroplasty following an ipsilateral above knee amputation. HIP Int 2013;23:104-7. [Google Scholar] [PubMed]
- 19. Ma C, Lv Q, Yi C, Ma J, Zhu L. Ipsilateral total hip arthroplasty in patient with an above-knee amputee for femoral neck fracture: A case report. Int J Clin Exp Med 2015;8:2279-83. [Google Scholar] [PubMed]
- 20. Patnaik S, Nayak B, Sahoo AK, Sahu NK Minimally invasive total hip replacement in an ipsilateral post-traumatic above-knee amputation: A case report. J Orthop Case Rep 2017;7:3-6. [Google Scholar] [PubMed]
- 21. Pekmezci M, Nunley RM, Barrack RL. Technique for total hip arthroplasty in a patient with through-knee amputation. J Arthroplasty 201025:659.e1-3. [Google Scholar] [PubMed]
- 22. Galloway R, Madanipour S, Lemanu D, Jayadev C, McCulloch R. Short- and long-term outcomes in patients with lower extremity amputations undergoing total hip and knee arthroplasty. Arthroplast Today 2023;20:101117. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Challenging Limb Salvage in a Crural Malignant Peripheral Nerve Sheath Tumor with Pre-existing Long-Stem Implants: A Case Report
March 1, 2026 Challenging Limb Salvage in a Crural Malignant Peripheral Nerve Sheath Tumor with Pre-existing Long-Stem Implants: A Case Report March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting
March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting March 1, 2026 Evaluation of Spine Hip Relation and its Correlation as a Guide to Total Hip Arthroplasty
March 1, 2026 Evaluation of Spine Hip Relation and its Correlation as a Guide to Total Hip Arthroplasty March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes
March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes