
A missed midtarsal injury in a patient with an extra-articular calcaneum fracture and a second metatarsal fracture, but presented with late deformity, which is difficult to diagnose at the acute stage, eventually requiring fusion.
Dr. Smit Shah, Trauma Registrar, Department of Orthopaedics, Ganga Hospitals Private Limited, Coimbatore, Tamil Nadu, India. E-mail: smitshah1997@gmail.com
Introduction: Midtarsal injuries, especially pure dislocations and subluxations, are commonly missed injuries, often misdiagnosed as sprains, due to the occult nature of radiographic findings. The authors present one such case of missed midtarsal and subtalar subluxation with extra-articular calcaneum fracture and 2nd metatarsal shaft fracture, which ended up in equinus, forefoot adduction, midfoot inversion, and missed due to prolonged immobilization.
Case Report: We present the findings in a 24-year-old active male patient, who sustained a fall from his 2 wheeler and was treated for Right Extra articular calcaneum fracture with 2nd metatarsal fracture elsewhere, developing a gradual equinus, adduction and supination deformity at the mid foot over 6 months and was eventually treated by the authors with tendoachilles lengthening with midfoot and tibiotalar with subtalar fusion using tibio-talo-calcaneal nail and beam screws due to the chronicity of the injury.
Conclusion: There are multiple articles describing acute medial swivel midtarsal dislocations, but none portraying a chronic gradual subluxation without fracture. The radiographical findings do not place this patient in any present classification present; the authors consider it a missed medial swivel type midtarsal subluxation with subtalar subluxation of the right side.
Keywords: Midtarsal injury, midfoot fusion, missed injury, foot and ankle deformity.
Midtarsal injuries are rare injuries of the midtarsal joint of the foot, comprising of the talonavicular joint (TNJ) and the calcaneocuboid joint (CCJ), collectively known as the Chopart joint. These joints are involved in movements, such as foot adduction-abduction and foot inversion-eversion. Studies suggest 41 % of these injuries are missed during initial assessment due to difficulties in diagnosing purely through radiographs, suggesting a more clinical mode of diagnosis is more feasible [1]. Main and Jowett first described a classification useful to study midtarsal dislocations, broadly divided into pure dislocations and fracture dislocations [1]. We present one such case that was initially missed on initial management, later diagnosed and treated for the same.
We present a case of a 24-year-old active Male, avidly participating in recreational activities before he suffered a road traffic accident causing a fall from his two-wheeler vehicle in February 2025. He sustained injuries to his right ankle. He was treated at a hospital near his home, where he was diagnosed a closed right extra-articular calcaneum fracture with second metatarsal shaft fracture, along with a deep abrasion over the dorsum of the ankle and foot. He was operated for the same with screw fixation of the calcaneum fracture with percutaneous pinning for the second metatarsal fracture (Fig. 1).

Figure 1: (A, B, C) Radiographs at the time of injury; (D, E, F) Three-dimensional computed tomography scans at the time of injury. (G, H) Post-operative radiographs after index surgery at the previous center.
He was then subject to serial dressings and cast applications for the next 4 months. At the end of 4 months, when the cast was removed, the abrasion was found to be non-healing, along with a deformity in the foot and ankle was noted. He then underwent split-thickness skin grafting for his ankle skin defect in June 2025. He then presented to us at 6 months post-injury to seek consultation for his deformity.
On examination, he had a walker-assisted-non-weight bearing gait with weight on the left lower limb. The right ankle was in equinus, with the forefoot in adduction and a grossly supinated midfoot. There was crowding of the toes with the great toe in varus and the second toe overriding it dorsally. The dorsalis pedis and posterior tibial pulses were well felt. Movements at the tibiotalar joint were restricted in equinus; correcting supination would elicit pain (Fig. 2).

Figure 2: (A, B, C) Clinical images portraying the present deformity of the patient on reception.
Radiographs and computed tomography (CT) were suggestive of an osteopenic bone stock, with dislocated CCJ and medially subluxed TNJ (Fig. 3). The Subtalar joint was also distracted laterally. He underwent the following procedure (Fig. 4): Tendoachilles lengthening (equinus component), Midfoot fusion (midtarsal dislocation), Ankle arthrodesis with fibula osteotomy and iliac crest bone grafting (lateral ligament complex injury and chronicity of injury).
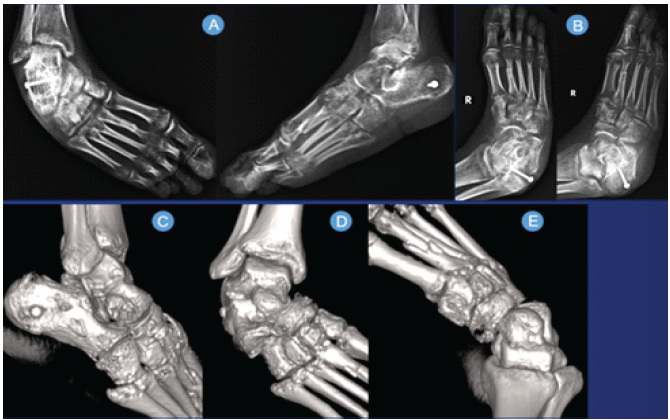
Figure 3: (A, B) Radiographs on reception by authors. (C, D, E) Three-dimensional computed tomography scans on reception by the authors.
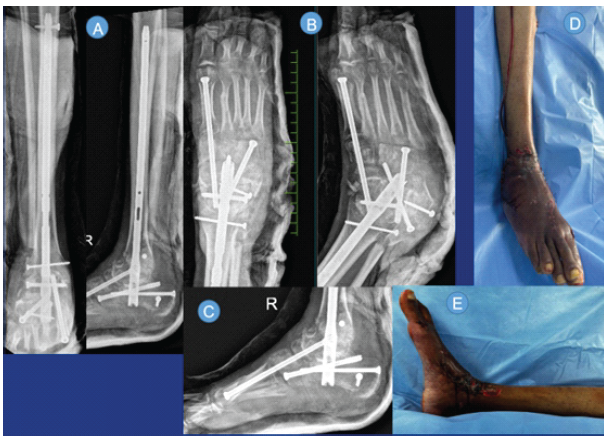
Figure 4: Post-operative radiographs (A, B, C) and clinical images (D, E) after ankle arthrodesis and midfoot fusion with tendoachilles lengthening and Iliac crest bone grafting.
The Chopart joint, including the TNJ and CCJ, while the CCJ takes part in 20–30% of inversion – eversion at the hindfoot [2], TNJ takes part in the pronation and supination of the tarsus [3]. The Chopart joint, comprised of the TNJ and CCJ, is stabilized by the dorsal talonavicular ligament, the bifurcate ligament, the Dorsal calcaneocuboid ligament, with the plantar calcaneocuboid ligament. It is an injury to these ligaments that causes midtarsal dislocation. The Chopart joint can be diagnosed well in the anteroposterior view by drawing the Cyma line, an S-shaped congruent line dividing the midfoot from the hindfoot. Any incongruency may suggest an issue with the Chopart joint. These dislocations often happen due to medial force onto the forefoot in a plantar flexed ankle. The Navicular subluxed medially, with pivot being the intraosseous talocalcaneal ligament; hence, the CCJ remains reasonably intact, with the calcaneum swiveling to face medially underneath the talus, but still maintaining its vertical position with respect to the talus (Fig. 5).

Figure 5: (A) Anatomy of ligaments stabilising the Chopart joint. (B) Image showing mechanism of injury on a 3D model [11]; (C, D) Cyma lines are drawn to portray congruency of Chopart joint; (E, F) Incongruent Cyma lines in this case.
The presented case portrayed a more gradual presentation of deformity, suggesting a ligament insult laterally with the forefoot eventually failing to retain its position, shifting to an inverted and adducted position. Neglection of these injuries has been reported upto 41% in acute midtarsal dislocation, although Howie et al reported five out of seven patients in their study of midtarsal occult subluxation were initially missed [7]. An interesting study by Behrens et al. maps the progressive collapse and foot deformity in peri-talar subluxation using three-dimensional pressure mapping [8]. In case of an acute injury, the treatment recommended for best outcomes is open reduction and internal fixation for both pure type and fracture dislocations [9]. Research articles do suggest that a higher index of suspicion is needed to diagnose such injuries, as neglection may lead to permanent disability [10].
The case presented here can be diagnosed as a case of neglected chronic right medial swivel midtarsal pure subluxation, as this patient has some continuity of the TNJ and CCJ, with a vertical profile of calcaneum. Due to chronicity of the injury, restricted deformities, and the patient’s goals of care, it was planned for tendoachilles lengthening with midfoot fusion and ankle arthrodesis. This injury was missed initially due to deceptively intact TMJ and CCJ, showing only mild subluxation in the initial radiograph and CT [11]. A high index of suspicion must be maintained to diagnose such injuries. A couple of shortcomings in our study include the unavailability of on MRI to document ligament injury, and also that a long-term follow-up is required to understand functional outcome and Gait characteristics.
Missed midtarsal injuries often lead to disabling deformities, which eventually lead to the need for fusion at midtarsal and also the tibio-talo-calcaneal joint, if the disease and deformity progresses. Early diagnosis and prompt treatment are necessary, so that the patient has a chance at full functionality. Although often missed, radiological guidelines do help in diagnosing such injuries.
References
- 1. Main BJ, Jowett RL. Injuries of the midtarsal joint. J Bone Joint Surg Br 1975;57:89-97. [Google Scholar] [PubMed]
- 2. Walter WR, Hirschmann A, Alaia EF, Tafur M, Rosenberg ZS. Normal anatomy and traumatic injury of the midtarsal (Chopart) joint complex: An imaging primer. Radiographics 2019;39:136-52. [Google Scholar] [PubMed]
- 3. Kou JX, Fortin PT. Commonly missed peritalar injuries. J Am Acad Orthop Surg 2009;17:775-86. [Google Scholar] [PubMed]
- 4. Sakharkar NS, Tathe PV, Garg R, Adewar AN, Giri VR, Sakhare KA. Medial swivel dislocation of the talonavicular joint due to high- energy trauma: A case report. J Orthop Case Rep 2023;13:33-7. [Google Scholar] [PubMed]
- 5. Datt N, Rao AS, Rao DV. Medial swivel dislocation of the talonavicular joint. Indian J Orthop 2009;43:87-9. [Google Scholar] [PubMed]
- 6. Milgram JW. Chronic subluxation of the midtarsal joint of the foot: A case report. Foot Ankle Int 2002;23:255-9. [Google Scholar] [PubMed]
- 7. Howie CR, Hooper G, Hughes SP. Occult midtarsal subluxation. Clin Orthop Relat Res 1986;209:206-9. [Google Scholar] [PubMed]
- 8. Behrens A, Dibbern KN, Mansur NS, Ehret A, Chen N, Stebral HJ, et al. Chopart peritalar subluxation in progressive collapsing foot deformity assessed by three- dimensional coverage maps. Foot Ankle Orthop 2022;7:2473011421S00580. [Google Scholar] [PubMed]
- 9. Metcalfe TS, Aamir J, Mason LW. Chopart dislocations: A review of diagnosis, treatment and outcomes. Arch Orthop Trauma Surg 2024;144:131-47. [Google Scholar] [PubMed]
- 10. Van Dorp KB, De Vries MR, Van Der Elst M, Schepers T. Chopart joint injury: A study of outcome and morbidity. J Foot Ankle Surg 2010;49:541-5. [Google Scholar] [PubMed]
- 11. Walter WR, Hirschmann A, Tafur M, Rosenberg ZS. Imaging of chopart (midtarsal) joint complex: Normal anatomy and posttraumatic findings. AJR Am J Roentgenol 2018;211:416-25. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Case Report: Foreign Body-induced Pseudomonas Arthritis Mimicking Tuberculous Ankle Infection in a Child
January 1, 2026 Case Report: Foreign Body-induced Pseudomonas Arthritis Mimicking Tuberculous Ankle Infection in a Child October 10, 2023 Delayed Spontaneous Fracture of the Proximal Tibia after Tibial Tubercle Osteotomy for Treatment of Patella Instability: A Case Report
October 10, 2023 Delayed Spontaneous Fracture of the Proximal Tibia after Tibial Tubercle Osteotomy for Treatment of Patella Instability: A Case Report February 10, 2022 Isolated Luxatio Erecta Femoris – Case Series and Review of Literature
February 10, 2022 Isolated Luxatio Erecta Femoris – Case Series and Review of Literature July 11, 2014 Chondroblastoma of Diaphysis of Radius in a Seven Year Old Child
July 11, 2014 Chondroblastoma of Diaphysis of Radius in a Seven Year Old Child