
This case report investigates a novel cause of failure in a total knee arthroplasty procedure, which highlights the importance of patient lifestyle, implant type, and prosthetic design when selecting components and planning for long-term surgical success.
Mr. Jonathan T Moshe, Orthopedic Associates of Long Island, East Setauket, New York. E-mail: jonathantmoshe@hotmail.com
Introduction: Total knee arthroplasty (TKA) is considered the definitive treatment for advanced degenerative disease in the knee and involves replacing the native joint with prosthetic components. Failure mechanisms have been studied extensively due to the ubiquitous nature of these procedures. In this case report, the failure of a press-fit patellar component in a cementless TKA is investigated as a novel complication.
Case Report: A 58-year-old male patient presented to an orthopedic clinic complaining of severe left knee pain with ambulation and associated varus alignment. He underwent X-ray imaging, where clear advanced osteoarthritis was visualized, with complete loss of joint space in the articulation of the medial compartment of the knee. Due to the patient’s pain levels and decreased mobility, the patient elected to proceed with a TKA. The patient underwent this procedure without immediate complication until he returned 19-months post-operatively. At this time, X-rays demonstrated a failed patellar component from a shear fracture of the single peg prosthesis. A revision surgery was then completed to resolve this issue.
Conclusion: Based on the present reported data on TKA modes of failure, this case describes the first report of a shear fracture of the single peg prosthesis in a cementless TKA.
Keywords: Total knee arthroplasty, patellar component, patella fracture, case report.
A total knee arthroscopy (TKA) is a surgical procedure in which an artificial knee joint replaces a diseased native knee. It is a typical treatment for patients who have advanced osteoarthritic degenerative change to the knee joint [1]. Most patients who undergo TKAs recover well and feel pain relief within 3–6 months, although 10–30% of patients report ongoing pain and dissatisfaction with the procedure [1]. Previous studies have analyzed the most common modes of failure after primary TKA, including infection, aseptic loosening, periprosthetic fracture, instability, arthrofibrosis, and osteolysis [1,2]. In this case, a novel cause of TKA failure of a press-fit patellar component is described. One group of investigators looked into patellar component failure in 5,640 TKAs performed [3]. These investigators defined patella failure as loosening, fracture, wear or fracture of the polyethylene or the base-plate, or the need for patellar revision surgery [4]. These various modes of failure, however, do not deal with the patellar prosthesis fracture in a cementless TKA described in this case study.
A 58-year-old white male with a past medical history of obesity, diabetes, and hypertension presented to the clinic with complaints of severe left knee pain with ambulation. The patient presents with a morbidly obese body habitus, weighing 345 lbs with a height of six feet (body mass index [BMI] 46.8). He is a non-smoker and occasionally drinks alcohol. He also reports exercising on occasion. The patient attempted and failed conservative treatment up until this point. He reports working as a maintenance man, where he bends and kneels for long periods of time daily. The patient underwent X-ray imaging, which included four views of the left knee, including anteroposterior (AP), lateral, patellofemoral, and tunnel views. The imaging provided clear advanced osteoarthritis with bone-on-bone articulation of the medial component of the knee and varus alignment (Fig. 1).

Figure 1: Pre-operative X-rays. Four views of the left knee are visualized on the patient’s initial visit, including anteroposterior, lateral, patellofemoral, and tunnel views, respectively. Bone-on-bone articulation of the medial component of the knee is appreciated.
Imaging and physical exam confirmed end-stage osteoarthritis of the left knee, and he was indicated for a left TKA. After both non-operative and surgical treatment options and their risks were reviewed with the patient, the patient opted to schedule a left TKA. A series of hyaluronic acid injections was administered to temporize the patient until surgery. The patient arrived at the hospital for a left TKA, where he underwent routine perioperative procedures. Spinal anesthesia with an adductor canal block was administered for sedation. A left TKA was then performed through a standard medial parapatellar approach. The patella was exposed, and the soft tissues were removed circumferentially. After everting the patella, a freehand cut with an oscillating saw through the level of the lateral patellar facet was performed. The patella was then sized and prepared for a 38-press-fit patella. The definitive implant was clamped into place. All extraneous osteophytes were removed with a rongeur. The knee was flexed, and a lateral release was not necessary to improve patella tracking. Standard procedure was then followed for closure, and a PRINEO dermabond was placed over the incision.

Figure 2: First post-operative X-rays. Three radiographic views of the left knee are visualized on the patient’s post-operative visit, including anteroposterior, lateral, and patellofemoral views, respectively. These radiographs demonstrate a press-fit total knee arthroplasty in place, well fixed, and well aligned, without periprosthetic fracture.
A post-operative X-ray showed the knee to be in appropriate alignment without evidence of complication (Fig. 2). The patient was transferred to the post-anesthesia care unit (PACU) in good condition, having tolerated the procedure well. Due to the patient’s high quality bone and relatively young age, a press-fit implant was chosen over the more traditional cemented implant, including: A standard width, size 8, Zimmer Persona CR Press-Fit Femoral Component, a size F, 2 peg, Press-Fit, Zimmer Persona tibial baseplate, a size 10 Zimmer Persona Medial Congruent Polyethylene Insert, and a size 38 Zimmer NexGen Press-Fit Patella. The patient continued to present for routine follow-up without evidence of complication for nearly 2 years until he returned to the clinic, stating that he had never been pleased with the operation. He complained of pain while standing, and at times, a sensation of “catching” and “giving out”. The patient underwent a normal physical exam. Three radiographic views of the left knee were examined for potential abnormalities. AP, lateral, and patellofemoral views of the left knee at this time demonstrated a failed patellar component with a shear fracture of the single peg prosthesis (Fig. 3). These findings were shared and discussed with the patient, who agreed to proceed with revision of the patellar component.
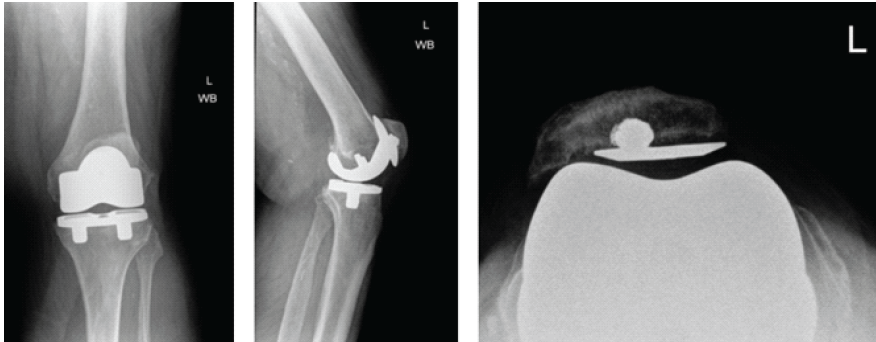
Figure 3: Second post-operative X-rays. Three views of the left knee are visualized at this post-operative visit, including anteroposterior, lateral, and patellofemoral views, respectively. These radiographs demonstrate a broken patellar component with a shear fracture of the single peg prosthesis. The femoral and tibial components appear well fixed and positioned.
The patient arrived at the hospital for his revision surgery and was prepared with routine perioperative procedures. After induction of anesthesia, he was prepped and draped in a sterile fashion. The patient’s previous midline incision was incised, and a medial parapatellar arthrotomy was performed. The soft tissue was elevated from the lateral knee to allow for eversion of the patella, and the component was noted to be grossly loose. Fibrous scarring was removed from the undersurface of the extensor mechanism to remove the polyethylene component. The central peg of the patellar component appeared well fixed within the patellar bone. There was metallosis noted in the synovium for which a synovectomy was performed. Changing the polyethylene was discussed. However, due to the patient’s vasculopathy, the goals to minimize dissection, bleeding, and the time of the surgery were prioritized. The polyethylene was not exchanged. As the other components appeared well fixed, balanced, and in place, only the patella was of concern. A freshening cut was made to flatten the patella and reveal fresh bone. A three-peg clamp was used to place three holes that surrounded the previous peg component (Fig. 4). The well-fixed broken peg was not removed to decrease unnecessary bone loss.
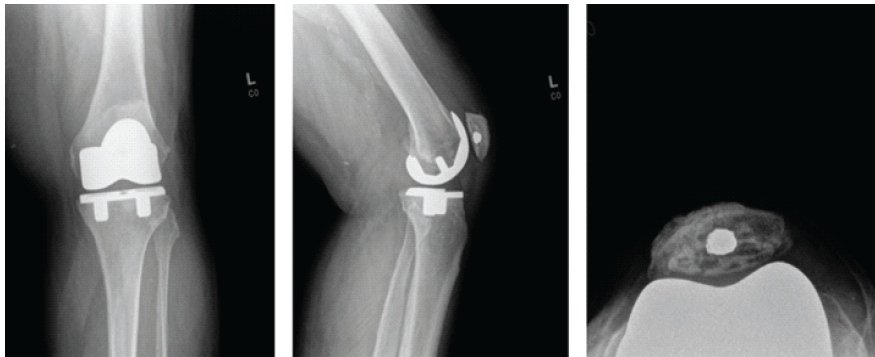
Figure 4: Post-operative X-rays after revision. Three radiographic views of the left knee are visualized on the patient’s post-operative visit, including anteroposterior, lateral, and patellofemoral views, respectively. These radiographs demonstrate the original press-fit total knee arthroplasty in position, with no loosening. The retained trabecular metal peg is appreciated within the patella.
After, cement was placed under the cut surface of the bone as well as on the backside surface of the implant. The patella was then clamped in place, and any extraneous cement was removed. The patella was then held in place until the cement was fully cured. It was ensured that the knee had a centrally tracking patella and was balanced in both flexion and extension. The patient’s incision was sutured closed appropriately, and a PRINEO dressing was applied. A post-operative X-ray showed the knee to be in good alignment. The patient was then taken to the PACU in good condition, having tolerated the procedure well. Since the surgery, the patient has been progressing routinely and describes being generally happier with his knee. The patient was last seen in February 2025. At this time, they report a positive response to treatment with satisfactory progress. Multiple attempts have been made to contact the patient to schedule an additional follow-up appointment 1 year after his last visit in 2025; however, these efforts have been unsuccessful to date. At the time of the past appointment, post-operative radiographs and physical exams all demonstrate appropriate alignment without evidence of complication (Fig. 4).
In the past several years, there has been an upward trend in press-fit TKAs, in an effort to increase survivorship in young, active, and heavy patients [5]. The two main types of patellar implants include the press-fit and cemented polyethylene components. One study looked into the biomechanical advantages of the two types of implants. The force to generate a periprosthetic patella fracture was measured in the press-fit versus the cemented polyethylene patella in a cadaveric model [6]. It was found that the average load to failure was significantly lower in press-fit patellar implants. Based on these findings, lifestyle and body habitus must be considered in determining what type of patellar component is best suited for each patient. In this case, the component was switched from a press-fit to a cemented polyethylene model. There have been multiple studies investigating modes of failure of metal-backed press-fit patellar components. The commonly reported failures include polyethylene wear, polyethylene fracture, and/or metallosis [4,5,7]. In all of these studies, none of the failures reported were a result of the peg shearing from the metal backing. To our knowledge, this case describes the first report of a shear fracture of the single peg prosthesis in a cementless TKA. This investigation also calls attention to the importance and evolution of press-fit TKA implant design. In recent years, the three pegged design for press-fit patellar component has more commonly replaced the single central peg [8]. One study compared the results between groups of patients who received the single versus the triple peg prosthesis. While the results were deemed insignificant, this study was likely underpowered. In ddition, the data did suggest that there were more complications with the single peg prosthesis [8]. It is suspected that this finding is likely due to a high amount of force through the single peg rather than the distribution through multiple pegs. In addition, a single peg prosthetic has less surface area for the bony ingrowth than a multiple-pegged prosthesis. For these reasons, it is surmised that this novel failure may have been caused by the implant only containing a single peg. Another variable that may contribute to the survivorship and performance of the implant is the shape of the patellar component. The three most common designs include the inlay, onlay round, and onlay oval [9]. Each of the implants has shown differing levels of bone coverage, with the onlay oval demonstrating a significantly higher percentage of coverage (85.9%) when compared to the others [9]. While there are different levels of bone coverage across implants, patient-reported outcomes appear to remain consistent, lacking significant differences among study groups at 6 months post-operatively. Alternatively, another study that assessed long-term survivorship of the prosthesis found that onlay options were an overall better choice in TKAs, due to the bone coverage of the patellar implant [10]. The question of resurfacing of the patella itself is another important and controversial question pertaining to this case, as the benefits of patellar resurfacing are not entirely agreed upon. With resurfacing, there is concern of fracturing, maltracking, loosening, and extensor mechanism injury [11]. When the patella is not resurfaced, anterior residual knee pain has been reported due to deterioration over time. In one study, it was found that the rates of anterior knee pain with walking and stairs were significantly less in the group with a resurfaced patella [11]. Eighty percent of the patients with a resurfaced patella were very satisfied with their TKA versus 48% in the group lacking patella resurfacing [11]. However, other investigators have shown that there is no significant difference in patient outcome between those who underwent patella resurfacing versus those who did not [12,13]. In the case study presented, the patient did not undergo a resurfacing procedure during the primary TKA [14]. During the revision, the patella was resurfaced, and subchondral bone was revealed to implant the new patellar prosthesis.
This case study describes an unusual complication of an otherwise normal total knee arthroplasty procedure. The TKA was performed on the patient’s left knee, without flaw, and with no added concern for immediate post-operative complications. The patient then presented 1 year after the operation with a shear fracture of the Zimmer NexGen press-fit, single peg, patellar prosthesis. To our knowledge, this is a novel complication yet to be described. The component was then revised to a Zimmer 3-peg, cemented patella. Based on the unique mode of failure demonstrated in this patient, caution is advised in using this type of implant in patients with obese body habitus who put excessive stress on their knees in their daily life.
It has been reported that complications of the patellofemoral joint are responsible for as much as half of all revision TKA’s. Of these complications, patellar implant fixation continues to be one of the most prevalent issues regarding these failures. Given the morbidity of these types of complications, it is important to consider the type of implant and the fixation method that is used for each patient, given their anatomy, age, and BMI. It is also worth considering the individual’s lifestyle and level of activity. The excessive stress placed on the patient’s knees during his occupation could have played a role in this patellar component failure. This unusual case may suggest exercising caution with the use of a press-fit, single peg, patellar component in heavy patients, particularly those who kneel and put excessive stress on their knees as part of their daily life.
References
- 1. Mathis DT, Lohrer L, Amsler F, Hirschmann MT. Reasons for failure in primary total knee arthroplasty – an analysis of prospectively collected registry data. J Orthop 2020;23:60-6. [Google Scholar] [PubMed]
- 2. Minutillo GT, Karnuta JM, Koressel J, Dehghani B, DeAngelis RD, Donegan DJ, et al. Fixation or revision for periprosthetic fractures: Epidemiology, new trends, and projections in the United States. J Bone Joint Surg Am 2024;106:1054-61. [Google Scholar] [PubMed]
- 3. Meding JB, Fish MD, Berend ME, Ritter MA, Keating EM. Predicting patellar failure after total knee arthroplasty. Clin Orthop Relat Res 2008;466:2769-74. [Google Scholar] [PubMed]
- 4. Bayley JC, Scott RD, Ewald FC, Holmes GB Jr. Failure of the metal-backed patellar component after total knee replacement. J Bone Joint Surg Am 1988;70:668-74. [Google Scholar] [PubMed]
- 5. Gustke KA, Simon P, Meheux CJ. Metal-backed patella implants in knee arthroplasty: Can the past predict the future? J Arthroplasty 2023;38:S131-6. [Google Scholar] [PubMed]
- 6. Patel AH, Wilder JH, Weldy JM, Ross BJ, Kim NE, Wang H, et al. Patella strength characteristics in cemented vs press-fit implants: A biomechanical analysis of initial stability. Arthroplasty Today 2022;14:140-7. [Google Scholar] [PubMed]
- 7. Garcia RM, Kraay MJ, Goldberg VM. Isolated all-polyethylene patellar revisions for metal-backed patellar failure. Clin Orthop Relat Res 2008;466:2784-9. [Google Scholar] [PubMed]
- 8. Larson CM, McDowell CM, Lachiewicz PF. One-peg versus three-peg patella component fixation in total knee arthroplasty. Clin Orthop Relat Res 2001;392:94-100. [Google Scholar] [PubMed]
- 9. Gharaibeh MA, Chen DB, Wood JA, MacDessi SJ. Characteristics of three different patellar implant designs in total knee arthroplasty. ANZ J Surg 2020;90:1303-9. [Google Scholar] [PubMed]
- 10. Gharaibeh MA, Tarassoli P, Chen DB, Wood JA, Beuzeville S, Quinn R, et al. Does choice of patellar implant in total knee arthroplasty matter?: A randomized comparative trial of 3 commonly used designs. J Bone Joint Surg Am 2023;105:145-56. [Google Scholar] [PubMed]
- 11. Mayman D, Bourne RB, Rorabeck CH, Vaz M, Kramer J. Resurfacing versus not resurfacing the patella in total knee arthroplasty: 8- to 10-year results. J Arthroplasty 2003;18:541-5. [Google Scholar] [PubMed]
- 12. Ali A, Lindstrand A, Nilsdotter A, Sundberg M. Similar patient-reported outcomes and performance after total knee arthroplasty with or without patellar resurfacing. Acta Orthop 2016;87:274-9. [Google Scholar] [PubMed]
- 13. Deroche E, Batailler C, Swan J, Sappey-Marinier E, Neyret P, Servien E, et al. No difference between resurfaced and non-resurfaced patellae with a modern prosthesis design: A prospective randomized study of 250 total knee arthroplasties. Knee Surg Sports Traumatol Arthrosc 2022;30:1025-38. [Google Scholar] [PubMed]
- 14. Rosenstein AD, Postak PD, Greenwald AS. Fixation strength comparison of onlay and inset patellar implants. Knee 2007;14:194-7. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 Novel Technique for Fracture Fixation of the Patella Following Unicondylar Knee Replacement: A Clinical Case Report
January 1, 2025 Novel Technique for Fracture Fixation of the Patella Following Unicondylar Knee Replacement: A Clinical Case Report March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report
March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report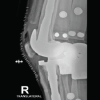 March 1, 2026 Sequential Bilateral Prosthetic Knee Infections Managed with Divergent Surgical Strategies: A Case Report
March 1, 2026 Sequential Bilateral Prosthetic Knee Infections Managed with Divergent Surgical Strategies: A Case Report March 1, 2026 Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review
March 1, 2026 Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review