
Tuberculous synovitis of the elbow with rice body formation is a rare mimicker of chronic inflammatory and neoplastic joint conditions, and requires high clinical suspicion with early surgical synovectomy plus anti-tubercular therapy to prevent irreversible joint destruction.
Dr. P. Ravisankar, Department of General Surgery, Division of Surgical Oncology, Sri Venkateshwaraa Medical College Hospital and Research Centre, Puducherry, India. E-mail: ravisankarpichaia@gmail.com
Introduction: Musculoskeletal tuberculosis accounts for a minority of extrapulmonary tuberculosis cases, with the elbow being an uncommon site. Rice body formation, though described in rheumatoid arthritis and chronic synovitis, are rarely reported in tuberculous arthritis.
Case Report: We describe a 70-year-old female presenting with progressive swelling and restriction of movement of the left elbow. Imaging revealed joint destruction with features suggestive of synovial chondromatosis, while biopsy and sputum studies were inconclusive. Surgical synovectomy revealed multiple intra-articular rice bodies, and histopathology confirmed tuberculous etiology. The patient received standard anti-tubercular therapy with physiotherapy, achieving pain relief and improved functional range of motion within 8 weeks.
Conclusion: This case highlights the diagnostic challenges of rice body tuberculosis, which may closely mimic other joint pathologies. Early surgical exploration, combined with anti-tubercular chemotherapy and rehabilitation, is essential for preventing irreversible joint damage and preserving function in rare extrapulmonary tuberculosis presentations.
Keywords: Musculoskeletal tuberculosis, elbow joint, rice bodies, synovectomy, granulomatous inflammation.
Musculoskeletal tuberculosis constitutes nearly 35% of extrapulmonary tuberculosis cases and accounts for about 1–3% of the total global tuberculosis burden [1]. The most frequently affected joints, in descending order, are the spine, hip, and knee. Tuberculous arthritis of the elbow joint is exceedingly uncommon, comprising only 1–5% of musculoskeletal tuberculosis presentations [1]. Chronic synovial inflammation accompanied by hypertrophy may, on occasion, produce rice bodies [2]. Rice body tenosynovitis represents an infrequent clinical entity linked to diverse causes such as rheumatoid arthritis and tuberculosis. If neglected, the presence of multiple rice bodies may exert mass effect, with potential neurovascular compromise or even secondary osteoporosis in adjacent osseous structures [3].
A 70-year-old female presented with an insidiously developing swelling over the anterior aspect of the left elbow, which gradually increased and led to progressive limitation of movement. On examination, a firm, cystic, and immobile mass measuring approximately 3 × 4 cm was detected on the anterolateral elbow, associated with severe restriction of joint motion (fixed flexion deformity with range 40°–90°) (Fig. 1).

Figure 1: Firm swelling over the anterior aspect of the left elbow, causing limitation of movement.
Neurovascular examination was unremarkable. Plain radiographs demonstrated advanced joint destruction (Martini-Stage 4) (Fig. 2) [4].
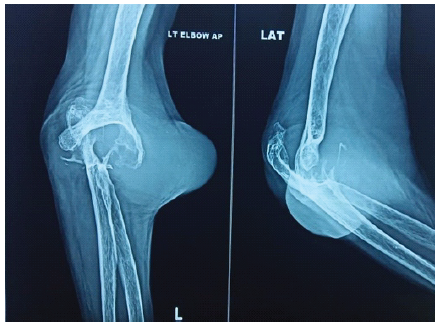
Figure 2: Plain radiographs demonstrated advanced joint destruction (Martini-Stage 4).
Magnetic resonance imaging (MRI) revealed an ill-defined lobulated lesion measuring 10 × 9 × 6 cm involving the synovium, intra-articular and periarticular tissues of the postero-lateral elbow, producing erosions of the distal humerus and proximal radius and ulna, with distortion of joint alignment, radiologically mimicking synovial chondromatosis (Fig. 3).
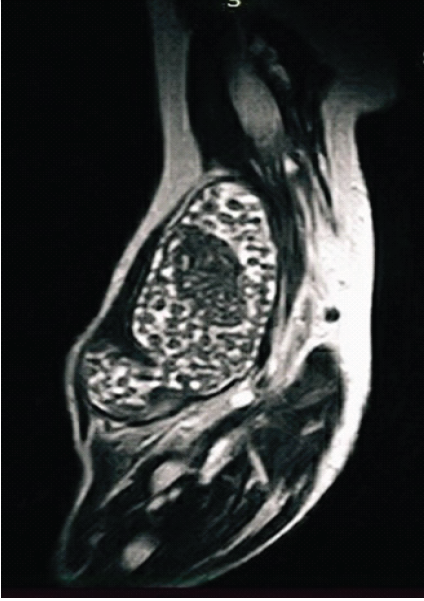
Figure 3: Magnetic resonance imaging revealed an ill-defined lobulated lesion measuring 10 × 9 × 6 cm involving the synovium, intra-articular, and periarticular tissues of the postero-lateral elbow.
Sputum smear for acid-fast bacilli and culture were negative. Core-needle biopsy yielded non-diagnostic results. Total synovectomy was performed, revealing a dislocated elbow joint with intact ligaments. Upon synovium incision, numerous glistening, friable rice bodies were found and excised en bloc. Thorough debridement of the joint was carried out, following which the limb was managed conservatively with an above-elbow immobilization cast for 6 weeks (Fig. 4).
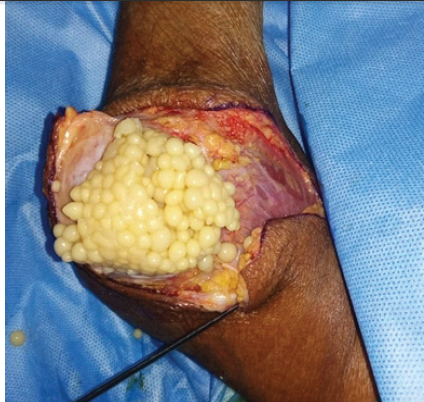
Figure 4: Synovectomy showing numerous glistening, friable rice bodies.
Histopathological examination confirmed chronic granulomatous inflammation with caseous necrosis and multinucleated giant cells, consistent with tuberculosis (Fig. 5).
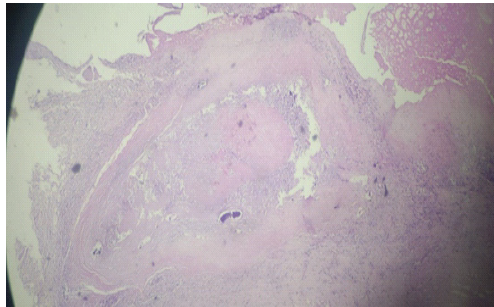
Figure 5: Low-power view of histopathological section demonstrating chronic granulomatous inflammation with caseous necrosis and multinucleated giant cells.
Postoperatively, with anti-tuberculous therapy (ATT) and physiotherapy, the deformity was corrected, and functional motion was regained, maintaining a range of 10°–100° by 8 weeks. The patient was followed up clinically for a period of 6 months, during which she maintained a stable functional range of motion (10°–100°) with clinical resolution of the infection and no evidence of recurrence. Further long-term follow-up was not possible as the patient expired due to an unrelated natural cause.
Skeletal tuberculosis develops from a latent pulmonary or extra-osseous source through hematogenous, lymphatic, or occasionally direct spread. In elbow tuberculosis, the olecranon and distal humerus are most often affected, while primary synovial involvement is rare [5]. Diagnostic challenges frequently arise because symptoms overlap with more common disorders such as rheumatoid arthritis, chronic pyogenic arthritis of low virulence, gout, pigmented villonodular synovitis, or even neoplastic lesions [6]. Rice bodies, initially described in 1895, are intra-articular particles resembling grains of rice [7]. Their exact pathogenesis remains controversial. They are thought to arise from chronic inflammation with features of osteomyelitis and arthritis [6]. The process begins with synovial inflammation and granulation tissue proliferation, leading to effusion and fibrin deposition, which eventually organizes into rice bodies. Cheung et al. demonstrated their protein composition resembled synovium, while Berg et al. described microvasculature within certain rice bodies [8,9]. While many originate intra-synovially, extra-articular rice bodies have also been reported, implying a non-synovial source. They are associated with chronic inflammatory conditions such as both seropositive and seronegative rheumatoid arthritis, osteoarthritis, and juvenile arthritis [10]. Rice bodies in extrapulmonary tuberculosis have been documented and are often slightly larger compared to those in autoimmune disorders. Eventually, pannus formation causes cartilage destruction, bone rarefaction, and caseous necrosis, though joint space may remain preserved for a considerable duration, influencing clinical outcomes [6]. Patients with elbow tuberculosis usually complain of pain, swelling, and stiffness, sometimes with localized warmth. Constitutional symptoms such as fever, malaise, and weight loss are infrequent. Because clinical features are non-specific, the disease often masquerades as other inflammatory or septic arthritis [11,12]. Delay in diagnosis can thus result in progressive and potentially irreversible joint destruction. Radiographic findings may demonstrate Phemister’s triad, characterized by juxta-articular osteopenia, marginal erosions, and progressive narrowing of the joint space [13]. Martini et al. categorized the radiological evolution of osteoarticular tuberculosis into four grades: Stage 1 – localized osteoporosis; Stage 2 – erosions or cavities in bone; Stage 3 – diffuse joint involvement without major destruction; Stage 4 – gross joint destruction [4]. MRI provides the most sensitive characterization. Rice bodies appear as uniformly hypointense loose bodies across sequences, with low signal intensity on T2 and proton-density weighted images. In contrast, synovial chondromatosis manifests as hyperintense nodules on T2-weighted images, assisting in differentiation [14]. Confirmatory diagnosis relies on biopsy with demonstration of caseating granulomas or culture positivity for Mycobacterium tuberculosis [1]. Management of rice body synovitis lacks standardized protocols. Conservative approaches are not endorsed in current literature [15]. Standard recommendations advocate a 9-month course of anti- ATT: An intensive 2-month phase with isoniazid (INH), rifampicin (RMP), pyrazinamide, and ethambutol, followed by a 7-month continuation phase with INH and RMP [16]. Early treatment combined with mobilization ensures favorable functional results [1]. Rice body excision is generally considered in symptomatic cases. Advanced peripheral joint tuberculosis can be addressed successfully with synovectomy, debridement, and abscess drainage, often obviating the need for arthrodesis [5]. However, studies report recurrence rates up to 60% when surgical intervention was undertaken without concurrent chemotherapy [17]. Hence, optimal outcomes require both prompt pharmacological therapy and appropriate surgical management when indicated. Surgical goals should prioritize joint preservation and function, as medical therapy primarily focuses on eradicating the infection.
Tuberculous arthritis of the elbow with rice body formation is rare and often mimics rheumatoid arthritis, synovial chondromatosis, or chronic septic arthritis, delaying diagnosis and causing joint damage. In our patient, definitive diagnosis was confirmed only after synovectomy and demonstration of caseating granulomatous inflammation in histopathological examination. Surgical removal of rice bodies, combined with anti-tubercular therapy and physiotherapy, restored functional mobility. This case highlights the need to consider tuberculosis in atypical elbow lesions and underscores the importance of combined surgical and medical management.
Elbow tuberculosis with rice body formation is an uncommon but important differential in chronic painless swelling and stiffness of the joint. Non-specific imaging may mimic synovial chondromatosis or inflammatory arthritis, delaying diagnosis. Early synovectomy with histopathological confirmation, followed by appropriate anti-tubercular therapy and physiotherapy, is crucial to restore function and prevent permanent joint destruction outcomes.
References
- 1. Khetpal N, Khalid S, Kumar R, Betancourt MF, Khetpal A, Wasyliw C, et al. Tuberculous arthritis of the elbow joint: An uncommon location with a diagnostic dilemma. Cureus 2018;10:e2462. [Google Scholar] [PubMed]
- 2. Suleman FE, Velleman MD. Intra-articular rice bodies: Imaging for persistent joint pain. S Afr Orthop J 2011;10:80-2. [Google Scholar] [PubMed]
- 3. Moein SA, Fereidooni R, Niakan R, Kousari A. Mycobacterium tuberculosis-induced multiple tenosynovial masses with rice bodies: A case report. Clin Case Rep 2023;11:e8228. [Google Scholar] [PubMed]
- 4. Domingo A, Nomdedeu M, Tomás X, García S. Elbow tuberculosis: An unusual location and diagnostic problem. Arch Orthop Trauma Surg 2005;125:56-8. [Google Scholar] [PubMed]
- 5. Davidson PT, Horowitz I. Skeletal tuberculosis. A review with patient presentations and discussion. Am J Med 1970;48:77-84. [Google Scholar] [PubMed]
- 6. Chavan S, Sable SS, Tekade S, Punia P. Tuberculous tenosynovitis presenting as ganglion of wrist. Case Rep Surg 2012;2012:143921. [Google Scholar] [PubMed]
- 7. Cheung HS, Ryan LM, Kozin F, McCarty DJ. Synovial origins of rice bodies in joint fluid. Arthritis Rheum 1980;23:7286. [Google Scholar] [PubMed]
- 8. Berg E, Wainwright R, Barton B, Puchtler H, McDonald T. On the nature of rheumatoid rice bodies: An immunologic, histochemical, and electron microscope study. Arthritis Rheum 1977;20:1343;9. [Google Scholar] [PubMed]
- 9. Guo JJ, Wu K, Xu Y, Yang H. Hundreds of rice bodies in the subacromial Hundreds o bursa: Report of two cases and literature review. BMC Musculoskelet Disord 2020;21:539. [Google Scholar] [PubMed]
- 10. Chen ST, Zhao LP, Dong WJ, Gu YT, Li YX, Dong LL, et al. The clinical features and bacteriological characterizations of bone and joint tuberculosis in China. Sci Rep 2015;5:11084. [Google Scholar] [PubMed]
- 11. Manske J, Tille E, Schlüßler A, Biewener A, Nowotny J. Tuberculosis of the elbow joint: The complexity of diagnosis and treatment-A case report and review of literature. J Med Case Rep 2025;19:88. [Google Scholar] [PubMed]
- 12. Ludwig B, Lazarus AA. Musculoskeletal tuberculosis. Dis Mon 2007;53:39-45. [Google Scholar] [PubMed]
- 13. Martini M, Benkeddache Y, Medjani Y, Gottesman H. Tuberculosis of the upper limb joints. Int Orthop 1986;10:17-23. [Google Scholar] [PubMed]
- 14. Tian Y, Zhou HB, Yi K, Wang KJ. Idiopathic tenosynovitis of the wrist with multiple rice bodies: A case report and review of literature. World J Clin Cases 2022;10:11908120. [Google Scholar] [PubMed]
- 15. Haibo Z, Tianrui W, Wenlian S, Shenjie S, Chunpu L, Xia Z, et al. A case of rice body synovitis of the knee joint. Orthop Surg 2022;14:628232. [Google Scholar] [PubMed]
- 16. Schaberg T, Brinkmann F, Feiterna-Sperling C, Geerdes-Fenge H, Hartmann P, Häcker B, et al. Tuberculosis in adulthood – The Sk2-Guideline of the German Central Committee against Tuberculosis (DZK) and the German Respiratory Society (DGP) for the diagnosis and treatment of adult tuberculosis patients. Pneumologie 2022;76:727-819. [Google Scholar] [PubMed]
- 17. Woon CY, Phoon ES, Lee JY, Puhaindran ME, Peng YP, Teoh LC. Rice bodies, millet seeds, and melon seeds in tuberculous tenosynovitis of the hand and wrist. Ann Plast Surg 2011;66:61017. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report
January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report November 1, 2025 Primary Synovial Chondromatosis of the Hip Joint: A Case Report
November 1, 2025 Primary Synovial Chondromatosis of the Hip Joint: A Case Report September 1, 2025 Humeroulnar Bridging Myositis Ossificans Traumatica: A Case Report
September 1, 2025 Humeroulnar Bridging Myositis Ossificans Traumatica: A Case Report August 1, 2025 Isolated Scapular Spine Involvement: A Rare Presentation of Osteoarticular Tuberculosis
August 1, 2025 Isolated Scapular Spine Involvement: A Rare Presentation of Osteoarticular Tuberculosis