
The combined use of osteocutaneous vascularized fibular flaps and external fixation enables successful reconstruction of complex foot gunshot injuries.
Dr. Marco Domenicucci, Department of Emergency Urgency, ASST Grande Ospedale Metropolitano Niguarda, Milano (MI), Italy. E-mail: marco.domenicucci@ospedaleniguarda.it
Introduction: Gunshot injuries to the foot can result in complex composite defects requiring comprehensive reconstructive strategies to restore both bony architecture and soft-tissue integrity. These injuries pose significant challenges due to extensive tissue destruction and the need for vascularized bone transfer.
Case Report: In this study, we present two cases of foot reconstruction using customized osteocutaneous vascularized fibular flaps following shotgun and rifle injuries, and we compare our approach with existing literature. Despite considerable soft-tissue loss, the primary arterial supply to the foot was preserved, allowing for successful microsurgical reconstruction. Our staged strategy, combining external fixation with vascularized fibular transfer, achieved favorable structural and functional outcomes.
Conclusion: These cases support the feasibility of using vascularized fibular flaps in severe foot trauma and emphasize the importance of meticulous surgical planning to optimize results.
Keywords: Fibula, surgical flap, wounds, gunshot, bone loss.
Gunshot injuries to the foot result in composite defects involving both bone and soft tissue, and the extent of damage is influenced by the type of ammunition used and the distance from which the shot was fired. These complex injuries typically require advanced reconstructive techniques, with the restoration of both soft-tissue coverage and bone. In this article, we present two cases of gunshot-related foot injuries treated with this reconstructive approach, which, to our knowledge, has been previously described in the literature for firearm injuries in only three patients [1,2,3].
Case 1
A 61-year-old male hunter was transferred to Sant’Anna Hospital in Como (Italy) from an orthopedic center in Croatia, where he had been treated 1 week earlier with local debridement and provisional external fixation following a short-distance (50 cm) smoothbore shotgun injury to the right foot during a hunting accident. On admission, the patient presented with a dorsal soft-tissue defect measuring 35 cm2 and a plantar defect of 18 cm2. X-rays revealed extensive bone loss, including the first, second, and third cuneiforms, the navicular bone, and the bases of the first and second metatarsals. Fractures of the third and fourth metatarsals and the proximal phalanx of the great toe were also observed, along with retention of multiple lead pellets. Computed tomography (CT) angiography showed no significant vascular damage, with patency of the anterior tibial, posterior tibial, interosseous, and dorsalis pedis arteries. Immediate local debridement and removal of visible lead pellets were performed, followed 2 days later by a second-look procedure. This included removal of devitalized bone fragments from the navicular, metatarsals, and cuneiform bones, removal of the previously applied external fixator, and stabilization with a Hoffmann 3 (Stryker) external fixator spanning from the distal tibia to the rearfoot (calcaneal tuberosity) and forefoot (first and fifth metatarsals). Gentamicin-loaded bone cement (Refobacin Bone Cement R, Zimmer Biomet) was interposed into the bone defects, covered with a reverse sural artery pedicle flap (Fig. 1). Vacuum-assisted closure (VAC) therapy was also applied.
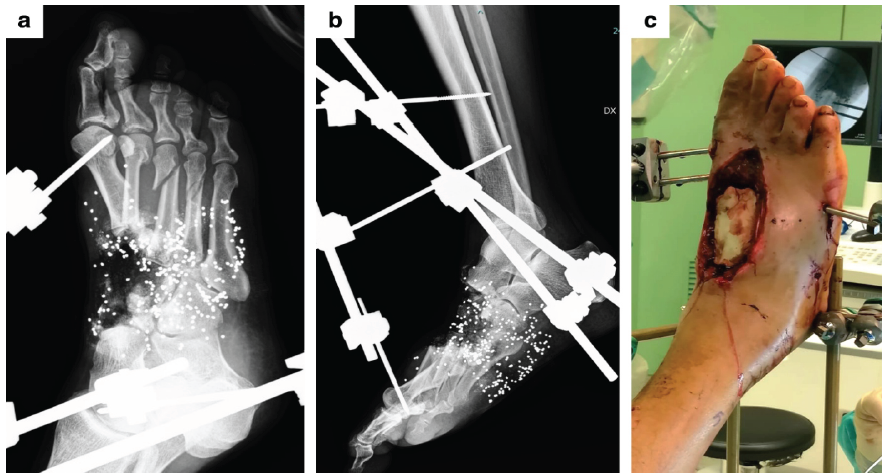
Figure 1: Case 1. (a and b) Radiographic images after the first surgical procedure of debridement and stabilization with an external fixator. (c) Clinical photograph showing the dorsal soft-tissue defect after placement of antibiotic-loaded cement.
During hospitalization, the initial antibiotic regimen included amoxicillin/clavulanic acid, gentamicin, and metronidazole, later modified to sulfamethoxazole combined with trimethoprim, following the identification of Enterobacter cancerogenous colonies. No further clinical signs of infection or bacterial growth were observed. The patient subsequently underwent reconstruction with an osteofasciocutaneous vascularized fibular graft. This included removal of the bone cement and remaining devitalized bone fragments, with harvesting of a contralateral osteofasciocutaneous fibula measuring 16.5 cm. Of this, 6.5 cm were used to reconstruct the first metatarsal and 7.5 cm for the second metatarsal, with a 2.5 cm interposed gap to avoid kinking of the pedicle during flap doubling. Flap insetting was stabilized with internal osteosynthesis using 2.0 mm plates and monocortical screws. Microvascular end-to-end anastomoses were performed between the flap pedicle and the anterior tibial artery and accompanying veins. A tenodesis of the distal tendon of the extensor hallucis longus to the extensor digitorum longus was also performed (Fig. 2).
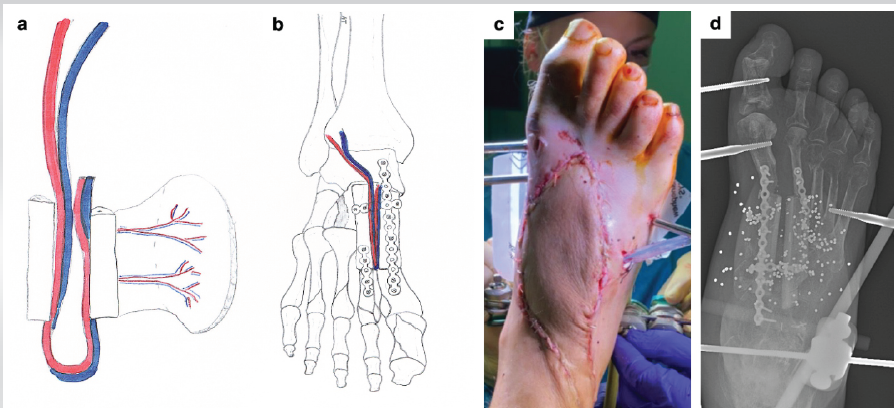
Figure 2: Reconstructive surgery in Case 1. (a and b) Preoperative planning for reconstruction with an osteofasciocutaneous vascularized fibular graft. (c and d) Clinical photograph and X-ray of the foot after surgery.
Subsequent procedures included removal of the external fixator and arthrodesis of the interphalangeal (IP) joint of the hallux, due to failure of the tenodesis. Partial weight bearing was allowed for 1 month, followed by full weight bearing. At 24-month follow-up, radiographs confirmed complete bone consolidation (Fig. 3). The patient was able to walk wearing normal shoes with a customized insole, without the aid of crutches, and without pain or limp.
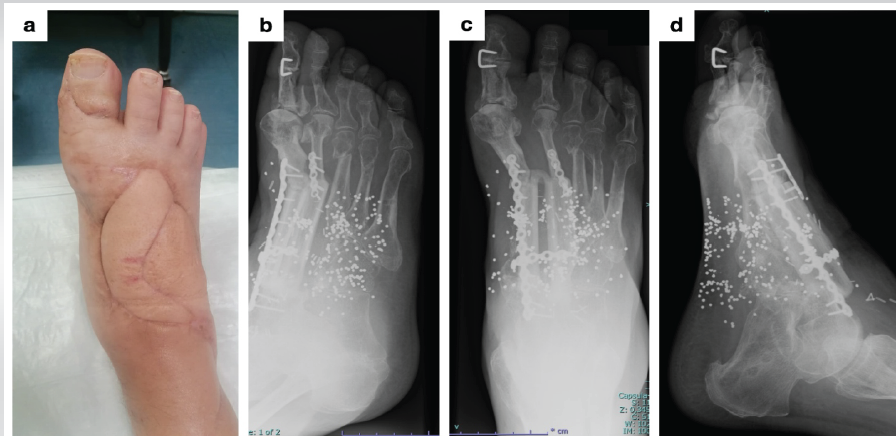
Figure 3: 24-month follow-up in Case 1. (a) Clinical photograph showing skin condition. (b-d) X-rays of the foot.
The American Orthopaedic Foot and Ankle Society (AOFAS) Hallux metatarsophalangeal-IP (MTP-IP) score was 80, and the AOFAS Hindfoot score was 90. Range of motion of the ankle joint was complete, and toe-off was preserved. The patient has returned to mountain hunting activities.
Case 2
A 67-year-old male hunter was admitted to Sant’Anna Hospital in Como with a composite right foot injury sustained during a boar hunting accident at close range (50 cm) involving a high-velocity rifle projectile. The soft-tissue defect measured 25 cm2 dorsally and 24 cm2 plantarly. Radiological evaluation revealed loss of the base and diaphysis of the first metatarsal, fracture of the first metatarsal head, loss of the base and diaphysis of the second metatarsal, fractures of the third and fourth metatarsals, and fracture of the proximal phalanx of the third toe. CT angiography demonstrated patency of the posterior tibial, anterior tibial, and peroneal arteries, with interruption of the dorsalis pedis artery at the base of the second metatarsal. An antibiotic regimen (amoxicillin, gentamicin, and metronidazole) was initiated immediately. Urgent debridement was performed, with removal of devitalized bone fragments from the first and second rays. Osteosynthesis of the third metatarsal was achieved using an intramedullary K-wire, and stabilization was provided with a Hoffmann 3 (Stryker) external fixator spanning from the distal tibia to the calcaneal tuberosity and the fifth metatarsal (Fig. 4).
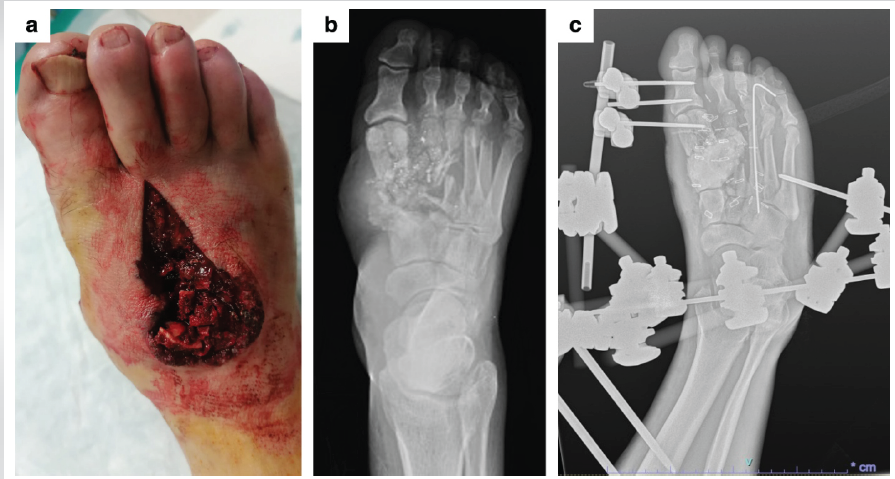
Figure 4: Initial presentation in Case 2. (a) Dorsal soft-tissue defect of the foot. (b) Initial X-rays at admission. (c) X-rays after surgical debridement and stabilization with an external fixator and Kirschner wire.
Due to fragmentation of the first metatarsal head, the first ray was stabilized using thinner half-pins (two in the proximal phalanx and one in the metatarsal head) connected to a Ministylo (Mikai) external fixator, which was connected to the Hoffmann frame. Gentamicin-loaded bone cement (Refobacin Bone Cement R, Zimmer Biomet) was used to fill the bone defects. The wound edges were approximated, and a VAC device was applied to the plantar side. In the following days, a second-look debridement was performed, along with dorsal soft-tissue coverage using a split-thickness skin graft. The main surgical procedure included the removal of the bone cement and residual bone fragments, followed by the harvesting of a free pedicled osteofasciocutaneous ipsilateral fibular flap. The harvested fibula measured 17 cm in length, with 7 cm dedicated to reconstruction of the first metatarsal, 7.5 cm to the second metatarsal, and a 2.5 cm interposed gap to prevent pedicle kinking. The skin paddle measured 35 cm2. The flap was inset using a 2.0 mm plate with bicortical screws to fix the graft to the first metatarsal, and an intramedullary K-wire for the second metatarsal. End-to-end microvascular anastomoses were performed between the fibular pedicle and the anterior tibial artery, anterior tibial vein, and great saphenous vein (Fig. 5).
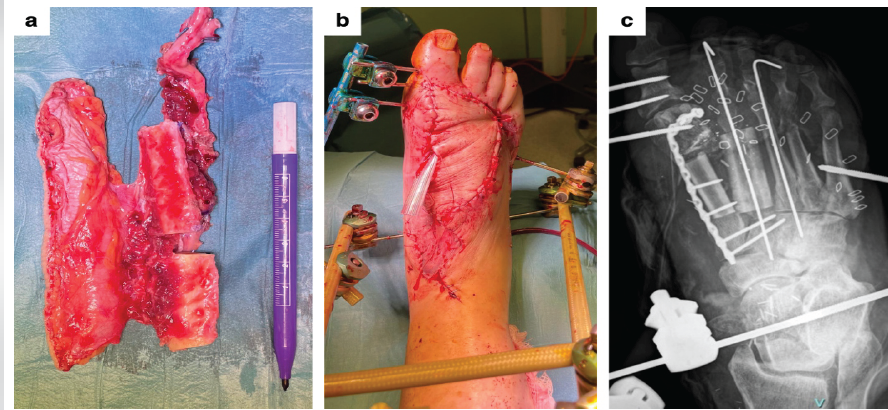
Figure 5: Reconstructive surgery in Case 2. (a) Free pedicled osteofasciocutaneous fibular flap harvested from the ipsilateral leg. (b and c) Clinical photograph and X-ray at the end of the surgical procedure.
The external fixator was maintained during the early post-operative period. At 9-month follow-up, the patient was ambulating without pain or limp. Functional scores were favorable, with an AOFAS Hallux MTP-IP score of 80 and a AOFAS Hindfoot score of 87. The patient resumed mountain treks.
Although the skin damage in the two patients differed according to the type of ammunition used, the underlying composite defects exhibited notable similarities, specifically, extensive bone loss involving the medial column and preservation of the major arteries responsible for foot perfusion. To our knowledge, the first report of three cases of foot reconstruction using a vascularized fibula dates back to 1993. Our literature review allowed us to collect a total of 21 cases in which this procedure was utilized for composite foot injuries. Patients with these injuries were typically young (mean age 29 years, range 10-51), with a predominance of males (89.4%). The etiology of the composite foot injuries was most often a crush injury [3,4,5,6,7,8,9,10], related to traffic [4,7,8] or work [9] accidents, or landmine explosions [1,2,3]. In three cases, firearm injuries were the cause of the damage, as in our patients. The mean skin paddle area of the osteofasciocutaneous graft was 102 cm2 (range 50–238), which is 43.6% larger than the initial soft-tissue defect. In our cases, we used a mean skin flap of only 25.5 cm2. In our patients, dorsal soft-tissue coverage was performed as a first-stage procedure before the vascularized fibula transfer. We harvested a fibula with a mean length of 16.75 cm, which falls at the upper end of the range reported in the literature (mean 9.9 cm, range 5–16 cm). This extended length was due to the use of a double-barreled fibula configuration, with the resection of an intermediate 2.5 cm segment to reduce stress on the vascular pedicle. In the literature, a double-barreled fibula has been employed in only two cases, and a triple-barreled configuration was reported in one case [6,9]. Stabilization of the graft was performed in all reviewed cases except one [10], with Kirschner wires and/or plates and screws [1,3,9]. In both our cases, we combined internal and external fixation, as reported in only one other article [1]. In the initial stage, the external fixator served to prevent mobilization of the cement spacer, misalignment of bone segments, and soft-tissue retraction. This strategy represents the first stage of the masquelet-induced membrane technique (IMT) [11], which allowed us to create a biological chamber that provided an optimal environment for the subsequent vascularized fibula graft. To the best of our knowledge, this is the first reported application of the IMT as a preparatory step for vascularized fibula grafting in composite foot defect reconstructions. The decision to retain the external fixator after placement of the graft was made to prevent displacement of the bone ends and to promote consolidation, particularly given the use of thin internal plates to minimize damage to the fibular graft. Regarding the type of microsurgical anastomosis, in our patients, the arterial pedicle was sutured to the anterior tibial artery, a technique also reported by other authors [3,5,7,9]. Alternative recipient arteries described in the literature include the posterior tibial artery [5,12] and the dorsalis pedis artery [2,6]. A reverse flow pedicle technique has been reported in one case [5], but it was associated with post-operative venous congestion and marginal graft necrosis [13]. In some cases, to minimize tension on the anastomoses, bypass grafting techniques were employed [6,9]. Venous anastomoses reported in the literature include connections to the anterior tibial veins, posterior tibial veins, and saphenous veins [2,3,4,5,6,7,9,12]. In our cases, we connected the pedicle veins to both the anterior tibial and saphenous veins. Only one Author [3] described a nerve coaptation, suturing the lateral sural cutaneous nerve to the dorsal cutaneous nerve to restore sensitivity to the skin paddle. Early complications reported include venous congestion and marginal necrosis in the case with reverse flow pedicle, subcutaneous hematoma requiring re-exploration and subsequent skin grafting [5], venous congestion and thrombosis managed with repeated anastomoses and a second cutaneous flap [4], and persistence of infection associated with venous congestion [8]. In our patients, no such complications were observed; the post-operative course was uneventful. In both cases, we aimed to preserve mobility of the first two MTP joints, to reduce mechanical stress on the grafts, and maintain proper gait mechanics, particularly during toe-off in the stance phase. In the short term, clinical results validated this approach: both patients achieved a plantigrade, pain-free foot, able to walk more than one kilometer without crutches or limping. They reported satisfactory aesthetic outcomes, were able to wear normal shoes with insoles, and returned to recreational hunting activities. At present, they show no signs or symptoms related to abnormal plantar pressure distribution. However, joint instability in the first case and MTP articular irregularities in the second suggest that painful MTP osteoarthritis may develop over time, potentially requiring arthrodesis.
Vascularized fibular flaps represent a reliable reconstructive option for firearm-related composite foot defects. Our staged approach, combining external fixation with Masquelet technique principles, led to stable and functional outcomes. This method not only restores weight-bearing capacity but also helps prevent long-term complications. Further studies are needed to evaluate the role of secondary joint stabilization procedures, particularly in cases with severe MTP joint involvement.
In our experience, the association of osteocutaneous vascularized fibular flaps with external fixation provided effective bone and soft-tissue reconstruction, leading to satisfactory functional recovery in complex foot gunshot injuries.
References
- 1. Gupta R, Pfennig M, Gannon J, Young D, Gupta R, Hart J, et al. Utilization of the free fibular flap for first metatarsal reconstruction. Plast Reconstr Surg Glob Open 2022;10:e4706. [Google Scholar] [PubMed]
- 2. Lykoudis EG, Dimitrios P, Alexandros BE. One-stage reconstruction of the complex midfoot defect with a multiple osteotomized free fibular osteocutaneous flap: Case report and literature review. Microsurgery 2010;30:64-9. [Google Scholar] [PubMed]
- 3. Zor F, Bayram Y, Kulahci Y. Functional reconstruction of arches of the foot with vascularized fibula flap. Ann Plast Surg 2023;91:571-7. [Google Scholar] [PubMed]
- 4. Arnež ZM, Troisi L, Colavitti G, Papa G, Leuzzi S, Stocco C, et al. Reconstruction of the weightbearing area of the foot with vascularized chimeric osteocutaneous fibular flap: A case report. J Foot Ankle Surg 2020;59:128-30. [Google Scholar] [PubMed]
- 5. Rajacic N, Ebrahim MK, Grgurinovic S, Starovic B. Foot reconstruction using vascularised fibula. Br J Plast Surg 1993;46:317-21. [Google Scholar] [PubMed]
- 6. Song L, Zhang Z, Wang Y, Liu Y, Liu Z, Chen L, et al. Reconstruction of a complex foot injury with free remodeled fibular osteocutaneous flap: A case report and literature review. J Foot Ankle Surg 2018;57:610-4. [Google Scholar] [PubMed]
- 7. Shet SM, Joseph S, Kalathinga K, Koyappathody HM, Samantaray SA, Latheef S. Lateral plantar arch reconstruction using vascularized fibula osteocutaneous flap. J Surg Case Rep Images 2021;4:1-5. [Google Scholar] [PubMed]
- 8. Wang CY, Han P, Chai YM, Lu SD, Zhong WR. Pedicled fibular flap for reconstruction of composite defects in foot. Injury 2015;46:405-10. [Google Scholar] [PubMed]
- 9. Yamashita Y, Hashimoto I, Goishi K, Fukunaga Y, Abe Y, Nakanishi H. Reconstruction of metatarsal bone defects with a free fibular osteomyocutaneous flap incorporating soleus muscle. J Plast Reconstr Aesthet Surg 2013;66:277-80. [Google Scholar] [PubMed]
- 10. Unal MB, Seker A, Demiralp B, Sahin M, Cift HT, Oltulu I. Reconstruction of traumatic composite tissue defect of medial longitudinal arch with free osteocutaneous fibular graft. J Foot Ankle Surg 2016;55:333-7. [Google Scholar] [PubMed]
- 11. Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am 2010;41:27-37. [Google Scholar] [PubMed]
- 12. Tan O, Atik B, Ergen D. Management of a composite foot defect due to mine explosion using the free fibula osteocutaneous flap. J Reconstr Microsurg 2008;24:53-6. [Google Scholar] [PubMed]
- 13. Minami A, Itoga H, Suzuki K. Reverse‐flow vascularized fibular graft: A new method. Microsurgery 1990;11:278-81. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Humerus Non-union with Segmental Bone Loss Treated with 3D-printed Prosthesis: A Case Report
February 1, 2026 Humerus Non-union with Segmental Bone Loss Treated with 3D-printed Prosthesis: A Case Report December 1, 2025 Fixation of Distal Fibula Fractures Associated with Extra-articular Distal One-third Tibia Fractures – Is It Necessary?
December 1, 2025 Fixation of Distal Fibula Fractures Associated with Extra-articular Distal One-third Tibia Fractures – Is It Necessary? October 1, 2025 Comparative Study of Minimally Invasive Plate Osteosynthesis Versus Open Reduction and Internal Fixation in the Treatment of Distal Fibular Fractures
October 1, 2025 Comparative Study of Minimally Invasive Plate Osteosynthesis Versus Open Reduction and Internal Fixation in the Treatment of Distal Fibular Fractures June 1, 2025 Clinical Significance of Vacuum assisted Closure in Management of Infected Wound: An Observational, Comparative Study
June 1, 2025 Clinical Significance of Vacuum assisted Closure in Management of Infected Wound: An Observational, Comparative Study