
A newly described magnetic resonance imaging sign—the “Head in the Sand sign”—provides an intuitive and easily recognizable visual cue that can improve diagnostic accuracy for bucket handle meniscal tears.
Dr. Rajkumar Amaravati, Division of Arthroscopy, Sports Injury, Joint Preservation and Regenerative Medicine, St John’s Medical College and Hospital, Bengaluru, Karnataka, India. E-mail: rajkumar_as@yahoo.co.in
Introduction: Bucket handle tears of the meniscus are frequently diagnosed using magnetic resonance imaging (MRI), with classical signs such as the double posterior cruciate ligament sign and the absent bow-tie sign aiding recognition. However, atypical fragment orientations may obscure these features. We describe a new MRI sign—the “Head in the Sand sign”—seen in a medial meniscus bucket handle tear.
Case Report: A 20-year-old male presented with right knee pain, locking, and restricted flexion after a twisting injury. MRI revealed a displaced bucket handle tear of the medial meniscus. In addition to typical findings, a novel MRI configuration was observed: The displaced fragment formed an inverted U-shape with the posterior horn, resembling the posture “Head in the Sand sign.” Arthroscopy confirmed a bucket handle tear with intact articular cartilage and cruciate ligaments. Meniscal repair was performed using an all-inside technique. The patient regained a full range of movements by 6 weeks.
Conclusion: The “Head in the Sand sign” is a newly described MRI sign that may assist in diagnosing medial meniscus bucket handle tears when classical findings are subtle or absent.
Keywords: Arthroscopy, meniscus, bucket handle tear, knee, magnetic resonance imaging.
Bucket-handle meniscal tears constitute approximately 10% of all meniscal injuries and are commonly associated with twisting trauma in young, active individuals [1]. Clinically, meniscal tears often present with joint line tenderness, episodic locking, clicking, and pain during deep flexion. Several static and dynamic bedside tests aid diagnosis. Static tests include joint line palpation and the Thessaly test in extension, while dynamic tests—such as McMurray’s test, Thessaly test at 20° flexion, Apley’s compression test, and Ege’s test—aim to reproduce pain or mechanical symptoms by stressing the meniscus under rotational or axial load. Although these tests provide useful clinical guidance, their diagnostic accuracy varies widely and may be influenced by examiner experience, patient guarding, or associated injuries. Comparatively, magnetic resonance imaging (MRI) offers significantly higher sensitivity and specificity for meniscal pathology and is considered the gold standard for non-invasive diagnosis. While clinical examination alone may miss tears or misclassify the pattern of displacement, MRI provides detailed anatomical visualization, enabling accurate identification of tear morphology, fragment orientation, and associated injuries [2]. Studies consistently show that MRI outperforms clinical examination in detecting complex configurations such as bucket-handle tears, where displaced fragments may alter joint mechanics or mimic other intra-articular pathology. MRI diagnosis traditionally relies on classical signs, including the double posterior cruciate ligament (PCL) sign, fragment-in-notch sign, and absent bow-tie sign. However, displaced fragments may occasionally assume atypical positions, rendering these signs subtle or incomplete [3]. We describe a newly identified MRI feature—the “Head-in-the-Sand Sign”—which offers an intuitive visual clue that may enhance diagnostic confidence in bucket-handle tears of the medial meniscus.
A 20-year-old male athlete presented with right knee pain, episodic locking, and reduced flexion following a twisting injury while playing football for 1 week.
Clinical examination
In our institution, for suspected meniscus injury, we perform Static tests include joint line palpation and the Thessaly test in extension, while dynamic tests, such as McMurray’s test, Thessaly test at 20° flexion, and Apley’s compression test, all of them were positive for the medial meniscus. Lachman and pivot-shift tests were negative, ruling out ACL insufficiency.
MRI findings
MRI demonstrated a displaced bucket handle tear of the medial meniscus, with the torn fragment flipped into the intercondylar notch [4,5]. On sagittal and coronal views, the displaced fragment formed an inverted U-shaped silhouette with the posterior horn, resembling a person in the “Head in the Sand sign” (Fig. 1). The posterior horn represented the “torso,” while the anteriorly displaced inner fragment angled sharply downward as the “arms and head.”
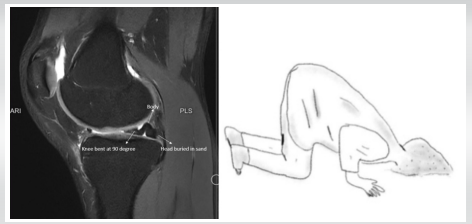
Figure 1: Magnetic resonance imaging finding and head-in-the-sand posture.
Arthroscopy
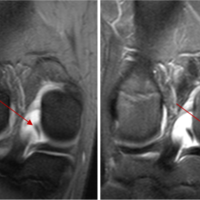
Diagnostic arthroscopy was performed using standard anterolateral and anteromedial portals. A systematic diagnostic sweep of all compartments—suprapatellar pouch, patellofemoral compartment, medial compartment, lateral compartment, and intercondylar notch—confirmed a displaced bucket-handle tear involving the body and posterior horn of the medial meniscus, with the fragment lying within the intercondylar notch (Fig. 2).

Figure 2: Bucket handle tear of medial meniscus
Freshening of the edges
The torn edges were prepared to enhance healing. This included rasping of the meniscal surfaces, trephination of the peripheral red-red/red-white zone, and minimal debridement to stimulate vascular access channels.
Reduction and stabilization
The displaced meniscal fragment was mobilized using a probe, carefully reduced into its anatomic position, and the stability of the reduction was assessed through knee flexion-extension cycles.
Plan of repair at our center
A structured repair strategy was followed based on tear location and morphology:
- Mid-third tear: Repaired using inside-out (Sironix) or outside-in sutures, ensuring robust fixation of the central segment
- Posterior root/Posterior horn region: Secured using all-inside vertical sutures, providing stable fixation in the posterior compartment with minimal risk to neurovascular structures. (Sironix/smith and nephew)
- Meniscal body: Reinforced using continuous running sutures, restoring hoop stress continuity along the length of the body. (Conmed-sequent)
- Anterior root component: A complete anterior root tear was repaired using an outside-in technique or an all-inside device based on accessibility and construct stability.
Following completion of the repair, the Microfracture procedure was performed to promote healing, and then the meniscus was probed and taken through a full range of motion to confirm stability, anatomical contour restoration, and absence of displacement. The articular cartilage and both cruciate ligaments were visualized and found to be intact (Fig. 3).

Figure 3: Post-repair of the tear.
Postoperative rehabilitation
Postoperative rehabilitation was initiated immediately following surgery. The patient was placed in a hinged knee brace locked at 60° of flexion, which was maintained for the first 6 weeks to protect the repair and minimize shear forces across the meniscus. Early passive range-of-motion exercises within the safe arc were permitted under supervision, avoiding deep flexion [6]. Weight-bearing was restricted to toe-touch/partial weight-bearing during the first 6 weeks, followed by progressive weight-bearing between 6 and 12 weeks, guided by pain, quadriceps control, and clinical assessment. Strengthening of the quadriceps and hip stabilizers was gradually introduced, along with closed-chain kinetic exercises, after adequate healing was established. By the end of 6 weeks, the patient regained a full range of motion, and functional rehabilitation continued with a focus on proprioception, neuromuscular control, and return-to-sport conditioning.
MRI remains the gold standard for evaluating meniscal pathology, particularly complex tear patterns such as bucket-handle tears. Classical MRI signs—including the double PCL sign, fragment-in-notch sign, and absent bow-tie sign—have traditionally aided diagnosis; however, these signs rely heavily on the orientation of the displaced meniscal fragment [7]. When the fragment assumes an atypical position or rotates partially, these signs may become subtle or even absent, increasing the risk of delayed or missed diagnosis. Early recognition is essential, as prompt repair has been shown to significantly improve healing rates and long-term meniscal preservation [8]. In the present case, the displaced fragment created an inverted U-shaped configuration with the posterior horn of the medial meniscus, resembling a “Head-in-the-Sand” posture on MRI. This intuitive visual pattern provides an additional interpretive clue that may assist radiologists and clinicians when classical signs are equivocal. Similar to the “double PCL” or “absent bow-tie” signs, this newly described sign builds on the concept of recognizing geometric or anatomic configurations to guide diagnosis [9,10]. Its value lies in its simplicity: it does not depend on duplication of ligaments or complete fragment rotation but instead focuses on the angulation between the torn fragment and the intact posterior horn. The importance of recognizing such variations is highlighted in recent literature. Studies have demonstrated that while MRI accuracy for meniscal tears is high, partial displacement or intermediate configurations may reduce sensitivity [11]. Quantitative MRI techniques—including synthetic MRI—have been proposed to improve tissue characterization and enhance detection of subtle tear patterns [12]. However, in routine clinical practice, pattern recognition on standard sequences continues to be the most widely used diagnostic approach. Arthroscopically, bucket-handle tears are repairable in most young patients, particularly when tissue quality is adequate, and the tear extends into the vascular zones. Multiple studies have demonstrated good healing outcomes and favorable long-term results after repair of bucket-handle tears, especially when combined with biologic augmentation or stable fixation constructs [13]. The technique used in this case—combining inside-out, outside-in, all-inside vertical sutures, and continuous running stitches—follows principles confirmed in biomechanical and clinical studies, which emphasize restoring the circumferential hoop stresses that are critical for meniscal function [14]. Preservation of the meniscus is preferred over meniscectomy, as loss of meniscal tissue significantly increases joint contact pressures and accelerates degenerative changes. Timing of surgery has also emerged as a key factor. Delayed repair has been associated with inferior healing and higher re-tear rates. Early identification using distinctive MRI signs, therefore, facilitates timely intervention and may improve clinical outcomes. In the current case, early repair allowed for anatomic restoration of the meniscus, and the patient achieved full range of motion by 6 weeks, consistent with reported outcomes in the literature [15]. Overall, the “Head-in-the-Sand Sign” offers a practical diagnostic addition to existing MRI signs for bucket-handle tears. It is especially useful in cases where the fragment is not fully displaced or where classical signs are incomplete. By improving diagnostic confidence, this sign may contribute to earlier recognition and more effective surgical management of bucket-handle meniscal tears [16].
Limitations
Being a single case report, the findings cannot be generalized, and further studies with larger sample sizes are required to establish the diagnostic utility of this MRI sign.
The “Head in the Sand sign” is a new and easily recognizable MRI sign associated with medial meniscus bucket handle tears. It may serve as a useful adjunct when classical MRI findings are incomplete or equivocal, improving diagnostic confidence and aiding timely management.
Recognition of the “Head in the Sand sign” on MRI can assist clinicians in diagnosing bucket handle meniscal tears, especially when traditional signs are subtle or absent.
References
- 1. Keyhani S, Movahedinia M, LaPrade RF, Qoreishy M, Vosoughi F. Long-term clinical results of using a posteromedial all-inside and anteromedial inside-out approach to repair unstable or irreducible bucket-handle medial meniscal tears. J Orthop Traumatol 2023;24:12. [Google Scholar] [PubMed]
- 2. Muench LN, Achtnich A, Krivec L, Diermeier T, Woertler K, Braun S, et al. Clinical outcome and healing rate after meniscal bucket handle tear repair. BMC Musculoskelet Disord 2022;23:1063. [Google Scholar] [PubMed]
- 3. Dzidzishvili L, Berreta RS, Jackson GR, Mowers CC, Cotter EJ, Allahabadi S, et al. All-inside and inside-out repair techniques for bucket-handle meniscus tears both result in improved patient outcomes and a broad range of failure rates: A systematic review. Arthroscopy 2024;40:2477-90.e1. [Google Scholar] [PubMed]
- 4. Zhang L, Mai W, Mo X, Zhang R, Zhang D, Zhong X, et al. Quantitative evaluation of meniscus injury using synthetic magnetic resonance imaging. BMC Musculoskelet Disord 2024;25:292. [Google Scholar] [PubMed]
- 5. Bashir S, Akhtar RR, Mirza AN, Sajid M, Javaid MZ, Arif A. Diagnostic accuracy of magnetic resonance imaging (MRI) in the diagnosis of meniscal tears, keeping arthroscopy as the gold standard. J Rawalpindi Med Coll 2025;29:e2922. [Google Scholar] [PubMed]
- 6. Rhamelani P, Mahdhiya NZ, Yoviana I, Jessica J, Komariah M. Early mobilization in post-orthopedic surgery patients: A scoping review. J Multidiscip Healthc 2025;18:305-17. [Google Scholar] [PubMed]
- 7. Bottomley J, Al-Dadah O. Diagnostic accuracy of magnetic resonance imaging in meniscal tears. Cureus 2025;17:e92155. [Google Scholar] [PubMed]
- 8. Herschmiller TA, Anderson JA, Garrett WE, Taylor DC. The trapped medial meniscus tear: An examination maneuver helps predict arthroscopic findings. Orthop J Sports Med 2015;3:2325967115583954. [Google Scholar] [PubMed]
- 9. Ganesan A, Alakhras M, Brennan PC, Mello-Thoms C. A review of factors influencing radiologists’ visual search behaviour. J Med Imaging Radiat Oncol 2018;62:747-57. [Google Scholar] [PubMed]
- 10. Javid K, Akins X, Lemaster NG, Ahmad A, Stone AV. Impact of time between meniscal injury and isolated meniscus repair on post-operative outcomes: A systematic review. World J Clin Cases 2025;13:95004-19. [Google Scholar] [PubMed]
- 11. Dorsay TA, Helms CA. Bucket-handle meniscal tears of the knee: Sensitivity and specificity of MRI signs. Skeletal Radiol 2003;32:266-72. [Google Scholar] [PubMed]
- 12. Jeevo J, D’Souza AD, Selvin B, Gupta GK, Babu VM, Amaravathi RS. Restoring stability – a case of a decade old triple bucket handle meniscus tear with an anterior cruciate ligament injury: Case report. J Orthop Case Rep 2025;15:113-9. [Google Scholar] [PubMed]
- 13. Lecas LK, Helms CA, Kosarek FJ, Garret WE. Inferiorly displaced flap tears of the medial meniscus: MR appearance and clinical significance. AJR Am J Roentgenol 2000;174:161-4. [Google Scholar] [PubMed]
- 14. Kouzelis A, Solou K, Panagopoulos A, Kokkalis Z, Gliatis J. Arthroscopic treatment of a “bucket-handle like tear” lesion of the medial meniscus. Cureus 2022;14:e22830. [Google Scholar] [PubMed]
- 15. Stensby JD, Pringle LC, Crim J. “MRI of the meniscus”. Clin Sports Med 2021;40:641-55. [Google Scholar] [PubMed]
- 16. Haas AL, Schepsis AA, Hornstein J, Edgar CM. “Meniscal repair using the FasT-Fix all-inside meniscal repair device. Arthroscopy 2005;21:167-75. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2024 Flag Sign: A Case Report of an Unusual Magnetic Resonance Imaging Finding of a Medial Meniscal Root Fragment in an Adolescent Water Polo Player
November 1, 2024 Flag Sign: A Case Report of an Unusual Magnetic Resonance Imaging Finding of a Medial Meniscal Root Fragment in an Adolescent Water Polo Player August 6, 2024 A Comparative Study on Correlation between Magnetic Resonance Imaging and Arthroscopic Findings in the Knee Joint Injuries
August 6, 2024 A Comparative Study on Correlation between Magnetic Resonance Imaging and Arthroscopic Findings in the Knee Joint Injuries February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report
February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report July 1, 2025 Locked Knee and Inferior Patellar Dislocation in an Elderly Patient: A Case Report and Review of the Literature
July 1, 2025 Locked Knee and Inferior Patellar Dislocation in an Elderly Patient: A Case Report and Review of the Literature