
[box type=”bio”] What to Learn from this Article?[/box]
Greater tuberosity union is a major criteria to get good range of movements, early diagnosis and management of shoulder dislocations is of prime impotence.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 53-56 | Tejas Upasani,Abhinav Bhatnagar, Sonu Mehta. DOI: 10.13107/jocr.2250-0685.432
Authors: Tejas Upasani[1,2], Abhinav Bhatnagar[1], Sonu Mehta[1]
[1] Department of Orthopaedics, Fortis Hospital, Mulund, Mumbai. Maharashtra. India.
[2] Upasani Nursing Home, Mulund, Mumbai. Maharashtra. India.
Address of Correspondence
Dr. Sonu Mehta,
7/2 Race Course Road, Silver Stud Building, Indore (M.P) -452003. India.
E-mail: sonu_mehta1987@yahoo.com
Abstract
Introduction: Shoulder dislocations are a very common entity in routine orthopaedic practice. Chronic unreduced anterior dislocations of the shoulder are not very common. Neurological and vascular complications may occur as a result of an acute anterior dislocation of the shoulder or after a while in chronic unreduced shoulder dislocation. Open reduction is indicated for most chronic shoulder dislocations.
We report a case of neglected bilateral anterior shoulder dislocation with bilateral displaced greater tuberosity fracture. To the best of our knowledge, only a handful cases have been reported in literature with bilateral anterior shoulder dislocation with bilateral fractures. Delayed diagnosis/reporting is a scenario which makes the list even slimmer and management all the more challenging.
Case Report: We report a case of a 35-year-old male who had bilateral anterior shoulder dislocation and bilateral greater tuberosity fracture post seizure and failed to report it for a period of 30 days. One side was managed conservatively with closed reduction and immobilization and the other side with open reduction. No neurovascular complications pre or post reduction of shoulder were seen.
Conclusion: Shoulder dislocations should always be suspected post seizures and if found should be treated promptly. Treatment becomes difficult for any shoulder dislocation that goes untreated for considerable period of time
Keywords: anterior shoulder dislocation, greater tuberosity fracture, late presentation.
Introduction
Ninety-five per cent of all shoulder dislocations are anterior [1]. The most common bilateral shoulder dislocation is posterior resulting from seizure or convulsion due to epilepsy, electric shock or other reasons [2, 3]. Simultaneous bilateral anterior shoulder dislocation is usually of traumatic origin and occurs rarely [4, 5]. Isolated displaced greater tuberosity fractures are thought to occur in less than 2% of proximal humeral fractures, and are normally associated with anterior shoulder dislocations. The greater tuberosity fragment detaches with its attached rotator cuff. The greater tuberosity fragment is pulled superiorly by the supraspinatus and posteriorly by infraspinatus and teres minor [8, 9]. Neglected anterior dislocations are less frequent than neglected posterior dislocations, because anterior shoulder dislocations are more familiar to the orthopaedic surgeon, and their radiological diagnosis is relatively easy [10]. The purpose of this paper is to report a case of neglected bilateral anterior shoulder dislocation with bilateral fracture, its occurrence, diagnosis and management.
Case Report
A 35-year-old male presented to the casualty 30 days after his first episode of seizure with pain in both shoulders and difficulty in movements. Patient had not taken any consultations with any doctor post the episode of seizure. Past history failed to shed any light as to the cause of the seizure with no history indicating earlier episodes involving head trauma, substance abuse/withdrawl or any pre-existing neurological cause. No previous episodes of shoulder dislocation were reported by the patient. On initial evaluation, the patient complained of decreased bilateral shoulder function and motion. On examination, normal shoulder contour was lost, shoulder movement was restricted especially abduction with arm in attitude of external rotation and pain was elicited with movement. Diagnosis of bilateral anterior shoulder dislocation was made clinically. Distal motor, sensory and vascular function was preserved. X-rays showed bilateral anterior shoulder dislocations with displaced greater tuberosity fractures (Fig.1).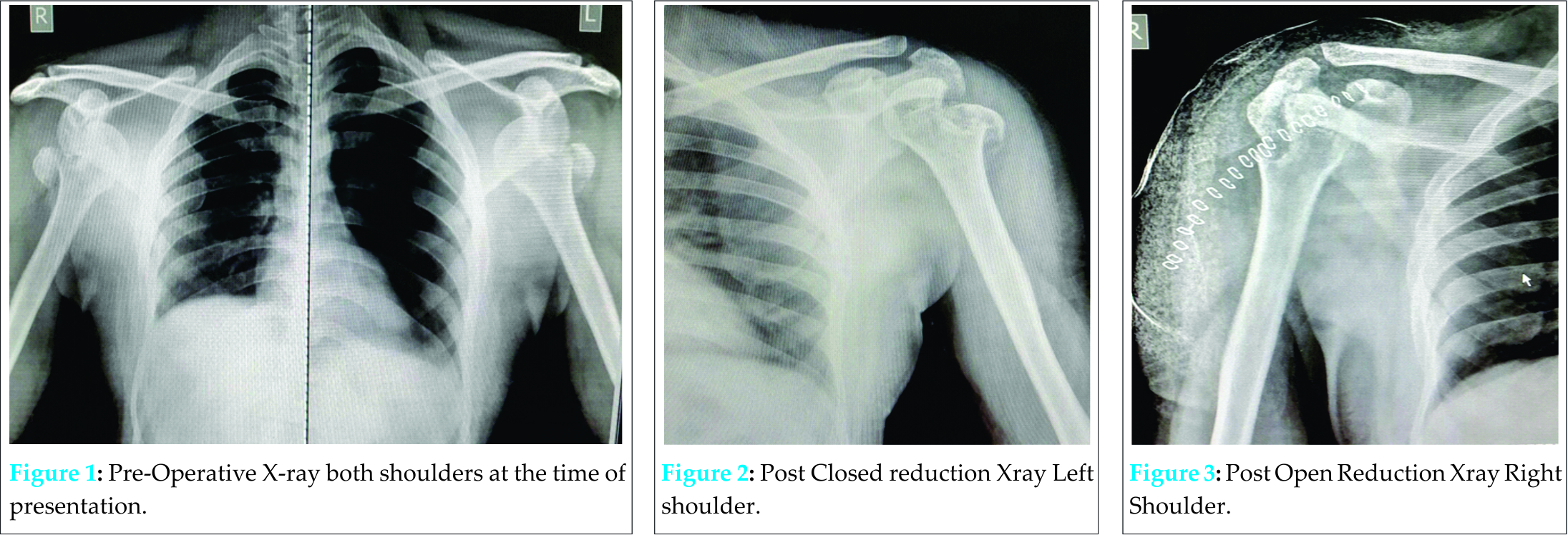
Left side closed reduction was done under general anesthesia followed by 3 weeks of immobilization and intermittent physiotherapy (Fig.2). Closed reduction of the right shoulder had been attempted but the shoulder was locked and attempts proved futile. During second sitting, open reduction was performed. Even after complete release, shoulder did not relocate, the gt was adhered to underlying bone. The gt was freed, repositioned and fixed with ethibond after repositioning ,the joint was reduced, capsule repaired, joint was stable and was put in an immobilizer. Details of open reduction- Standard deltopectoral approach was used. Conjoint tendon was retracted . humeral head was seen to pierce through the subscapularis muscle. After subscapularis was released, still there had been difficulty in reduction due to capsular adhesions. After releasing the capsule, reduction was attempted again, but was found to be unstable. Greater tuberosity was malpostioned and was adhered to proximal part of humerus. Adhesions were released and greater tuberosity was brought back into position fixed with ethibond and joint was reduced. Capsullorhaphy was done, subscapularis repaired. Joint found stable and greater tuberosity was well reduced and in position under C arm. Patient was put in a shoulder immobilizer and continued for 3 weeks. For rehabilitation, gentle pendulum exercises were started post operatively, but the patient was non compliant and moved his shoulder joint inspite of instructions. Patient came for follow up after 3 weeks and X- ray showed partial displacement of greater tuberosity. However, for displaced greater tuberosity, we decided to continue rehabilitation and monitor progress . At 6 weeks follow up, patient had active assisted forward flexion of 110 degrees, active abduction of 60 degrees. At 12 weeks follow up active abduction was 150-160 degrees. We report post-operative follow up of 3 weeks and 3 months wherein at the end of 3 weeks the side that underwent closed reduction had full abduction and the side that underwent open reduction had no wound complications, had started pendular movements and was under physiotherapist care for gradual mobilization (Fig. 4, 5). 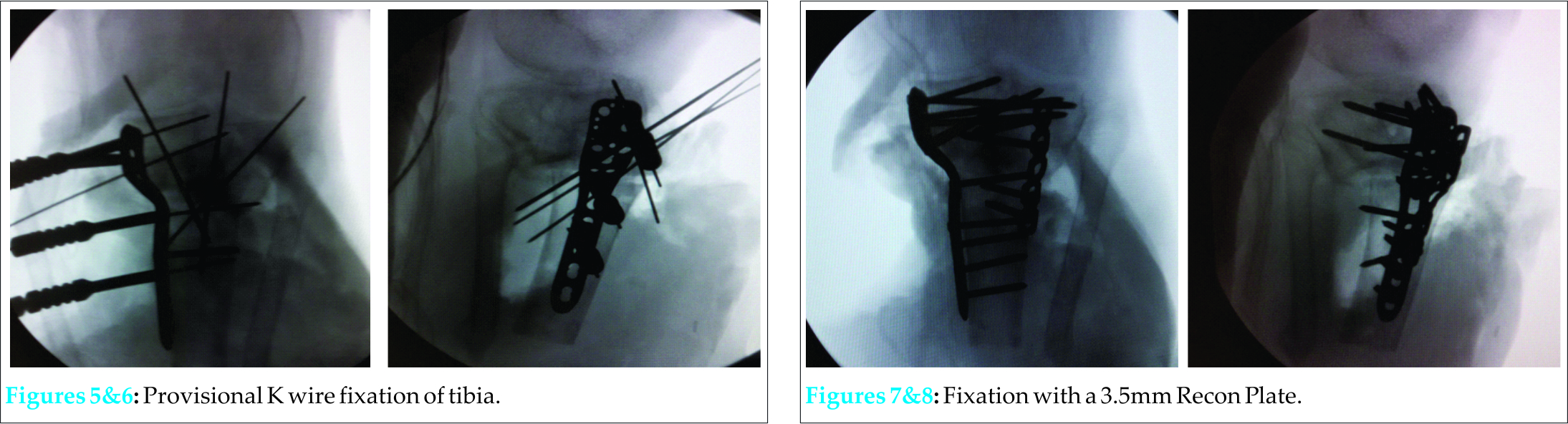 At the end of 3 months, the side reduced closed had full abduction, no complaints of pain and the side reduced open had 150-160 degrees range of motion (Fig. 6, 7, 8) with 3 month follow up X-ray also posted showing union of greater tuberosity (Figs. 9, 10).
At the end of 3 months, the side reduced closed had full abduction, no complaints of pain and the side reduced open had 150-160 degrees range of motion (Fig. 6, 7, 8) with 3 month follow up X-ray also posted showing union of greater tuberosity (Figs. 9, 10).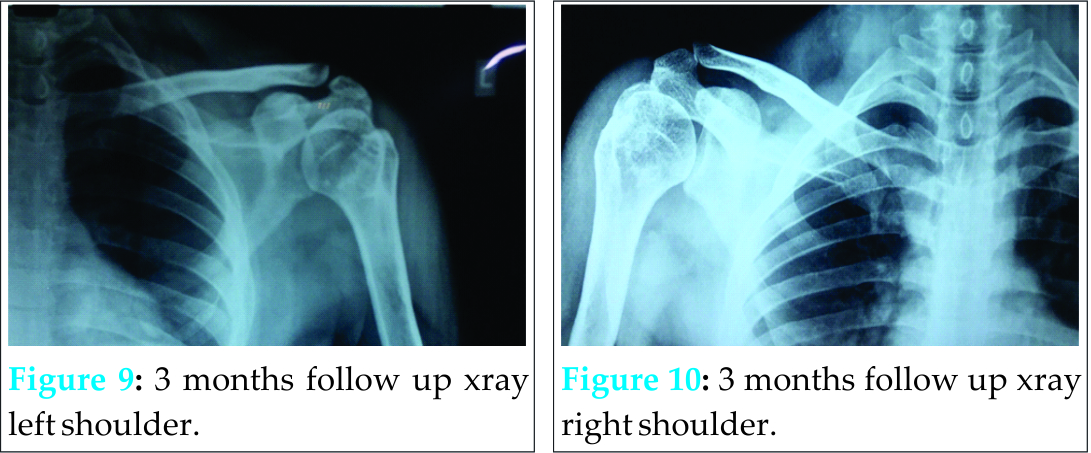
Discussion
Anterior shoulder dislocations, unlike posterior happen almost always, secondary to trauma. Posterior shoulder dislocations usually occur following unbalanced muscle contractions (electric shock, epileptic seizure etc) [5]. The posterior dislocations are more common after seizure since the contraction of the relatively weak teres minor and infraspinatus and the posterior fibers of the deltoid are overcome by the more powerful subscapularis leading to internal rotation and posterior subluxation [11]. Keeping the above in mind, it is difficult to explain why an episode of seizure would lead to bilateral anterior shoulder dislocation. Connor-Read L et al suggested that anterior dislocation with seizure may occur not during the muscle contractions but from the trauma of the shoulders striking the floor, after the collapse [11]. This could have been so in the case presented here as well but the patient did not report fall post seizure or could not remember but the presence of similar looking fracture dislocation patterns on both sides is perplexing. Even with trauma bilateral anterior shoulder fracture dislocation pattern is difficult as almost always one extremity takes the brunt of the impact [5,11]. Simultaneous bilateral anterior shoulder dislocations are rare. They have a unique mechanism of injury and were first described in 1902 in patients in whom excessive muscular contraction occurred as a result of camphor overdose by Mynter [17]. Associated fracture of the greater tuberosity occurs in 15% of the anterior dislocation cases and indicates an associated rotator cuff tear [12]. This may cause long term instability and functional impairment if the fragment is not anatomically reduced [5]. Thus, internal fixation after the reduction must be the ruled out in such cases. However with regards to the demands of the patient, cost constraints, closed reduction on one side and open reduction on the other without any implant aided fixation was done. MRI was not done on either side to evaluate rotator cuff but open reduction was done on one side due to block in closed reduction. This block usually can be caused by either soft tissue interposition esp. Long head of biceps or subscapularis tendon [24], or as is more likely in our case a bony block. A displaced glenoid labrum, a bony fragment from the glenoid rim, greater tuberosity fragment or an impacted humeral head into inferior lip of glenoid are the mentioned osseous causes of an irreducible anterior shoulder dislocation [25-28]. In our case, both soft tissue interposition caused by tissue and capsular contractures as well as bony block due to adherent greater tuberosity seen while doing open reduction were the cause causing interference in reduction. We could find only 5 other reports of bilateral anterior fracture dislocation patterns involving the greater tuberosity which were chronic. Yadav reported a case (also caused by seizure) of a 56-years-old man, which was reported 6 weeks after injury but the patient was treated with benign neglect and, at 6-month follow-up, no union was seen at fracture site but the patient could perform some functional activities and had accepted possibility of future ailments like arthritis and periarthritis[18]. Carew-McColl described a case that had been caused by electrocution and treated with open reduction and no fixation. At final follow-up, the 78-year-old female patient had abduction 80° bilaterally and no external rotation [19]. Thomas and Graham treated a similar injury in a 65-year -old woman who had fallen from a bus but not been diagnosed until 8 months later. The patient was treated with staged bilateral hemiarthroplasties [20]. Salem reported the same injury in a 37-year-old man who had been electrocuted at work. Diagnosis was delayed 9 weeks, and he was treated with bilateral open reductions without fixation [21]. Seth D. Dodds published a report involving a 27-year-old man having similar injury post seizure 2 month late presentation treated bilaterally by open reduction internal fixation [22]. Closed reduction of a neglected anterior shoulder dislocation can be performed only up to six weeks post injury. After this period the danger of an iatrogenic fracture or neurovascular damage rises too high and operative procedures shall be followed [13]. Hence, we tried to attempt closed reduction on both the sides. Looking at literature, the neglect of this dislocation is thankfully rarely reported. There is, however, significant variability of this injury. Shoulder hemiarthroplasty has been used with these injuries [14]. However, it is recommended that the head should be preserved in young patients [15]. Sometimes neglect of these injuries is recommended with acceptance of subnormal function [16]. Given the delay in presentation in our patient the possibility of avascular necrosis must also be considered and should be followed up at intervals to assess the same. Closed reduction without hampering the soft tissue attachments and blood vessels which would otherwise be in jeopardy in open surgery could be construed as naive as incidence of AVN is more common in fracture dislocations involving surgical or anatomical humeral neck [23].
Conclusion
Shoulder fracture dislocations best treated acutely. In Old cases special attention needs to be given to patient expectations, functional motion, risk of AVN and management given taking into account all relevant factors.
Clinical Message
Shoulder dislocation is extremely common after episodes of seizure and should be evaluated clinically as well as radiologically. Fractures of greater tuberosity may also be associated with it, hence any attempt at closed reduction should be made only after radiological evaluation with preparedness for open reduction if the need arises.
References
1. Devalia KL, Peter VK. Bilateral post traumatic anterior shoulder dislocation. J Postgrad Med.2005.
2. Cave EF, Burke JF, Boyd JF. Trauma Management: Year Book Medical Publishers. Chicago;1974.
3. Honner R. Bilateral posterior dislocation of the shoulder. Aust N Z J Surg. 1969.
4. Peiro A, Ferrandis R, Correa F. Bilateral erect dislocation of the shoulders. Injury 1975.
5. Dinopoulos HT, Giannoudis PV, Smith RM, et al. Bilateral anterior shoulder fracture-dislocation. A case report and a review of the literature. Int Orthop 1999.
6. Segal D, Yablon IG, Lynch JJ, et al. Acute bilateral anterior dislocation of the shoulders. Clin Orthop Relat Res 1979.
7. Markel DC, Blasier RB. Bilateral anterior dislocation of the shoulders with greater tuberosity fractures. Orthopedics 1994.
8. MS George. Fractures of the greater tuberosity of the humerus. Journal of the American Academy of Orthopaedic 2007.
9. A Green, J Izzi. Isolated fractures of the greater tuberosity of the proximal humerus Fractures. Journal of shoulder and elbow surgery 2003.
10. Abdelhady AM. Neglected anterior shoulder dislocation: open remplissage of the Hill-Sachs lesion with the infraspinatus tendon. Acta Orthop Belg 2010.
11. Connor-Read L, Bloch B, Brownlow H. A missed orthopaedic injury following a seizure: a case report. J Med Case Reports 2007.
12. Neer CS. Displaced proximal humeral fractures. J Bone Joint Surg [Am] 1970.
13. Solomon L, Warwick D, Nayagam S. Injuries of the shoulder, upper arm and elbow. In: Solomon L, Warwick D, Nayagam S, editor. Apleys System of Orthopaedics and Fractures. London: Arnold;2001.
14. Kumar AJS, Oakley J, Wootton J. Dynamic posterior stabilization of shoulder hemiarthroplasty in long-standing neglected posterior dislocation of the glenohumeral joint. Int J Should Surg. 2008.
15. Chalidis BE, Papadopoulos PP, Dimitriou CG. Reconstruction of a missed posterior locked shoulder fracture–dislocation with bone graft and lesser tuberosity transfer: a case report. J Med Case Rep.2008;
16. Ghafil D, Putz P. Subnormal functional activity in a neglected posterior dislocation of the shoulder. Acta Orthop Belg 1998.
17. Ng A.B., Rix T.E. Roy B.R. Acute bilateral anterior destructions of the shoulders. UlsterMed J 2000.
18. Yadav SS. Bilateral simultaneous fracture-dislocation of the shoulder due to muscular violence. J Postgrad Med. 1977;23(3):137-139.
19. Carew-McColl M. Bilateral shoulder dislocations caused by electric shock. Br J Clin Pract. 1980;34(8-9):251-254.
20. Thomas DP, Graham GP. Missed bilateral anterior fracture dislocations of the shoulder. Injury. 1996;27(9):661-662.
21. Salem MI. Bilateral anterior fracture-dislocation of the shoulder joints due to severe electric shock. Injury. 1983;14(4):361-363.
22. Dodds SD and Medvecky MJ. Chronic Bilateral Locked Anterior Shoulder Fracture-Dislocations. Am J Orthop. 2008;37(7):364-368.
23. Suso S, Peidro L, Ramon R. Avascular necrosis of the humeral head after dislocation with fracture of the greater tuberosity. Acta Orthop Belg. 1992;58(4):457-459.
24. Wen DY. Current concepts in the treatment of anterior shoulder dislocation
Am J Emerg Med 1999;17 (4):401–407.
25. Guha AR, Jago ER. Irreducible acute anterior shoulder dislocation. Int J Clin Pract. 2004;58(12):1184-1186.
26. Inao S, Hirayama T, Takemitsu Y. Irreducible acute anterior shoulder dislocation; interposed bicipital tendon. J Bone Joint Surg 1990;72B:1079-1080.
27. Ilahi OA. Irreducible anterior shoulder dislocation with fracture of the greater tuberosity. Am J Orthop 1998;576-578.
28. Seradge H, Orme G. Acute irreducible acute anterior dislocation of the shoulder. J Trauma 1982;22:330-332.
| How to Cite This Article: Mehta S, Upasani T, Bhatnagar A. Bilateral Neglected Anterior Shoulder Dislocation with Greater Tuberosity Fractures. Journal of Orthopaedic Case Reports 2016 April-June;6(2): 53-56. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-432-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2022 Asymmetric Bilateral Chronic Shoulder Dislocation in a Young Patient – A Rare Case Report
October 10, 2022 Asymmetric Bilateral Chronic Shoulder Dislocation in a Young Patient – A Rare Case Report November 1, 2025 Management of Solitary Osteochondroma Arising from Mammillary Process of D12 Vertebra in an 11-Year-Old Female: A Rare Case Report and Literature Review
November 1, 2025 Management of Solitary Osteochondroma Arising from Mammillary Process of D12 Vertebra in an 11-Year-Old Female: A Rare Case Report and Literature Review July 10, 2017 Articular Reconstruction using Subchondral Cementation and Threaded Kirschner-wires in Giant Cell Tumor: A Novel Technique
July 10, 2017 Articular Reconstruction using Subchondral Cementation and Threaded Kirschner-wires in Giant Cell Tumor: A Novel Technique February 1, 2025 Suprapatellar Technique for Tibia Fractures: Is the Fracture Level Important?
February 1, 2025 Suprapatellar Technique for Tibia Fractures: Is the Fracture Level Important?