
[box type=”bio”] What to Learn from this Article?[/box]
We should always look for DVT in high risk paediatric in-patients especially with sepsis and major trauma. When in doubt, it should be ruled out with proper investigations.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 72-74| Chandrashekara CM, Mulamoottil Abraham George. DOI: 10.13107/jocr.2250-0685.442
Authors: Chandrashekara CM[1], Mulamoottil Abraham George[1]
[1]Department of orthopedic surgery, Al-Buraimi Hospital, P.O.B 8, P.code 512. Al-Buraimi. Sultanate of Oman.
Address of Correspondence
Dr. Chandrashekara.C.M,
Department of Orthopaedic Surgery, Al-Buraimi Hospital, P.O.Box 8, P.code 512.AL-BURAIMI. OMAN.
E-Mail: drshekar76@rediff.com
Abstract
Introduction: The incidence of deep vein thrombosis (DVT) in pediatric patients is significantly much lower than adults. Most of the pediatric in-patients with major trauma, sepsis do not undergo routine screening for DVT.
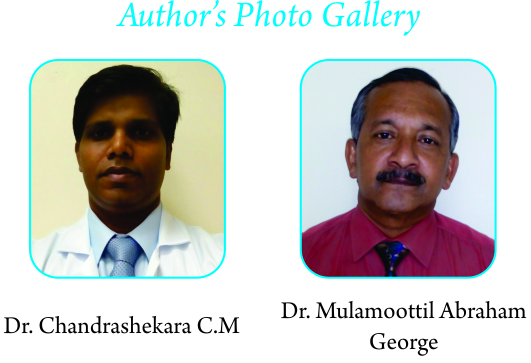
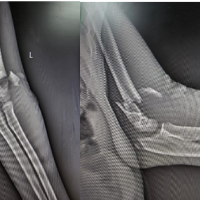
Case report: We present a case of a 12-year-old boy presented to us with minor trauma to right ankle associated with swelling, pain and had associated cough, and fever. On investigation with plain X-ray of right ankle/chest, and blood parameters, patient was suspected of having cellulitis of right leg with chest infection. Patient was treated with IV Cloxacillin and ample of rest. During the course of treatment, patient’s condition deteriorated with fever, tachycardia and a swollen leg without much pain. Duplex scan was performed where the right leg revealed thrombosis of popliteal vein, while CT scan of chest with angiogram ruled out possibility of pulmonary embolism. However, CT chest showed pneumonia with pulmonary effusion. Patient was treated with low molecular heparin and IV Cloxacillin for pneumonia. Patient recovered completely and there was no recurrence during follow up period of 6 months.
Conclusion: The possibility of DVT in pediatric should be kept in mind and when suspected, should be properly investigated and treated.
Keywords: Venous thrombosis, Popliteal vein, Pediatrics, Case reports.
Introduction
Incidence of deep vein thrombosis (DVT) is significantly low in paediatric patients in comparison to the adults. These days, more children are hospitalized for longer duration due trauma and various medical problems. However, the disease is very much under-diagnosed and under-reported probably due to less awareness among treating physicians, a significantly large number pediatric patients may be asymptomatic. Furthermore, routine screening for DVT is not done in this age group despite longer duration of immobilization and intensive care treatments. Most of the reported cases in literature are related to malignancy, central catheters site infections and neurosurgical injuries. We are presenting this case report after receiving consent from patient’s father & approval by the hospital ethical committee.
Case Report
12-year-old boy presented with history of trauma to his right ankle three days back. He complained of pain and swelling of right ankle. He also gave a history of associated cough and fever since 5 days. The personal and past history was insignificant.
Patient was febrile with 38.5 degree Celsius temperature; tachycardia at 125/min and respiratory rate 25/min. Right ankle was mildly swollen with redness, local rise of temperature, tenderness over lateral malleolus, lower 3rd leg laterally (Fig. 1). There was restriction of ankle movements. No neurovascular deficits. Rest of the limb was normal. Plain X-ray of right ankle with leg was normal. His blood parameters were; haemoglobin-12.5gm%;total count-21.28K/uL; neutrophils-19.77K/uL; lymphocytes-0.75K/uL%, CRP-360.1mg/L(positive); ESR–60mm/hr; RAfactor-negative; ASO-titre-400IU/ML; sickling-negative. Urine routine was performed and found to benormal. Patient was admitted for treatment of suspected cellulitis, pediatric opinion was sought for cough. Chest X-ray: revealed pneumonia, therefore he was started on IV Cloxacillin 1gm four times daily. Later blood culture revealed growth of Staphylococcus aureus which was sensitive to Cloxaciilin. On the 3rd day, patient’s general condition deteriorated with persistently elevated temperature, tachycardia (140/min), respiratory rate at 40/min and SPO2- 87% at room air with moderate swelling on whole of right leg with tender calf and a positive Homan sign. D-Dimer test was negative. CT angiogram of chest was carried out to rule out pulmonary embolism. There was no evidence of embolism, but showed right sided pleural effusion and bilateral patchy pneumonia. The duplex scan of right lower limb was suggestive of popliteal vein thrombosis (Fig. 2, 3),thrombophilia work up for protein C &S; anti-thrombin III was negative. Patient was treated with low molecular heparin and IV cloxacillin (for pneumonia) in intensive care unit. Patient improved clinically, calf swelling was reduced and blood parameters were also reverting to normalcy at the time of discharge. Patient was discharged on 14th day and was treated with warfarin for next 3 months. Repeat duplex scan at 6 weeks was normal. Patient was followed up for period of 6 months, and there were no signs of recurrence.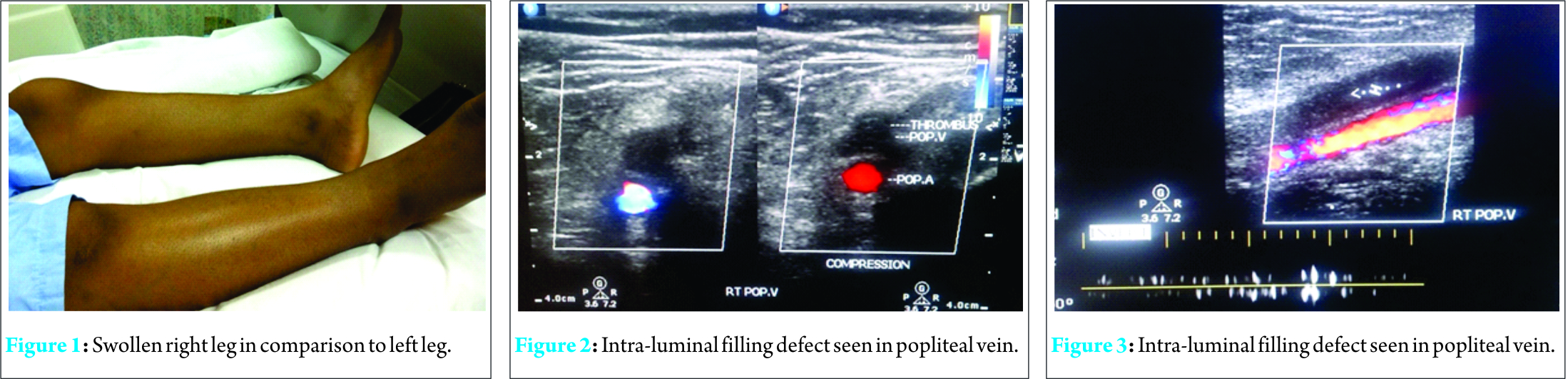
Discussion
The incidence of popliteal vein thrombosis in children is significantly lower than the adults. Although the development of deep venous thrombosis in pediatric patients is unusual, it certainly does occur and can be complicated by the development of pulmonary embolism and the long-term sequelae of the postphlebitic syndrome [1]. Most of the cases reported in the literature are often associated with long term hospitalizations, intensive care treatment and central lines/deep musculoskeletal structures associated sepsis.[1, 2, 3, 4, 5]. It is possible that the disease is significantly under diagnosed in children because the index of suspicion of pediatric practitioners is low, a substantial number of patients may have no symptoms, and DVT screening is not routinely performed [1]. There are many risk factors identified to be associated with DVT among children. Among them, sepsis, immobility, trauma, operative procedures, indwelling femoral venous line and malignancy are more frequently reported. While, obesity, hypercoagulability state and previous history of DVT /pulmonary embolism are less frequent [1]. Our patient had trauma to his right ankle followed by superficial soft tissue infection and an associated pneumonia, but he did not have rest of the risk factors mentioned above. Despite moderate swelling of leg, patient did not have any other local symptoms. In order to diagnose DVT, there is need for objective tests rather than just a clinical assessment alone. The low incidence of DVT noted in this study suggests that DVT screening in patients who are at low risk and have no symptoms is not appropriate and that DVT prophylaxis is unnecessary in pediatric patients with fewer than three risk factors for the development of DVT [1]. The risk of clinically significant thromboembolic event in trauma patients under age 13 is negligible. Therefore, VTE prophylaxis is unnecessary in pediatric patients with traumatic injury [6]. Our hospital does not have the policy of routine screening and prophylaxis therapy for DVT in pediatric patients. Although contrast venography is considered the standard criterion for diagnosis of DVT, time, personnel, cost, exposure to radiation and invasive nature of the study (need for venous access) potentially limit the ability to perform the study in emergency settings. Ultrasonography is an alternative method for thrombus detection and is widely preferred [7]. Although the D-dimer test was negative, as the clinical suspicion of DVT was high, we went on to do duplex scan; which confirmed popliteal vein thrombosis. Incorporating D-dimer testing into a diagnostic strategy with clinical estimation of pretest probability and ultrasound imaging simplifies the diagnosis of deep-vein thrombosis in outpatients without compromising safety [8]. We further investigated our patient with computer tomographic pulmonary angiography to rule out pulmonary embolism, as he had respiratory symptoms with Staphylococcus aureus growth on blood culture. In S. Bouchoucha et al study, the occurrence of DVT was significantly associated with septic pulmonary locations. Three patients developed respiratory distress associated with pulmonary lesions suggestive of pleuropulmonary Staphylococcus infection [9]. Furthermore, our patient was treated with low molecular heparin and warfarin. Low-molecular weight heparin therapy has many benefits over unfractionated heparin agents and may be more appropriate for the prophylaxis or treatment of children and adolescents with DVT because of its acceptable safety and efficacy [10]. There was no recurrence during follow-up period.
Conclusion
The incidence of DVT in a pediatric in-patient is still a possibility in trauma and sepsis. The careful clinical assessment of pediatric in-patient is important to the diagnosis of deep vein thrombosis. Ultrasound scan can be used as an effective tool in confirmation of diagnosis. Adequate and early treatment can prevent thromboembolic complications. The possibility of septic emboli should be kept in mind while treating such patients.
Clinical Message
The incidence of popliteal vein thrombosis is on rise in pediatric trauma & septic patients. When suspected, it should be adequately investigated & properly treated to prevent further complications.
References
1.Rohrer M J, Cutler B S, MacDougall E, . Herrmann J B, Anderson F A Jr. et al. A prospective study of the incidence of deep venous thrombosis in hospitalized children. Journal of Vascular Surgery 1996;24(1): 46–50.
2.Sandoval JA, Sheehan MP, Stonerock CE, Shafique S, Rescorla FJ, Dalsing M C et al. Incidence, risk factors, and treatment patterns for deep venous thrombosis in hospitalized children: an increasing population at risk. J Vasc Surg. 2008;47(4):837-43.
3. Lan T. Vu, Kerilyn K. Nobuhara,Hanmin Lee,Diana L. Farmer. Determination of risk factors for deep venous thrombosis in hospitalized children. Journal of Paediatric Surgery.2008; 43(6):1095–1099.
4.Wang JSYin HH, Zhu YF, Yao C, Lin Y, Chang GQ et al. Risk factors and therapeutic management of deep venous thrombosis in hospitalized children.[Article in Chinese]. Zhonghua Yi Xue Za Zhi. 2010; 90(15):1051-3.
5.S. Bouchoucha, Trifa B M, SaiedW , Douira W, Nessib M Na et al. Deep venous thrombosis associated with acute hematogenous osteomyelitis in childrenOrthopaedics & Traumatology. Surgery & Research 2010; 96(8): 890–893.
6. Michelle A C, Jane M E, Richard S J, Brebbia et al. Venous Thromboembolic Events in Pediatric Trauma Patients: Is Prophylaxis Necessary? Journal of Trauma-Injury Infection & Critical Care 2005; 59 (6):1345-1349.
7.Tay ET, Stone MB, Tsung JW. Emergency ultrasound diagnosis of deep venous thrombosis in the pediatric emergency department: a case series. Pediatr Emerg Care 2012; 28(1):90-5.
8. Wells P S, , Anderson D R, , Rodger M, Forgie M,Kearon C, Dreyer J et al. Evaluation of D-Dimer in the Diagnosis of Suspected Deep-Vein Thrombosis. N Engl J Med 2003; 349:1227-1235.
9..Bouchoucha S Trifa B M, Saied Wa, Douira W, Nessib M N, Ghachem M B et al, Deep venous thrombosis associated with acute hematogenous osteomyelitis in children. Orthopaedics & Traumatology: Surgery & Research 2010; 96(8):890–893.
10.Levy M L, Hart D, and Meltzer H . Deep venous thrombosis in children and adolescents. Journal of Neurosurgery: Pediatrics 2004; 101(2):32-37.
| How to Cite This Article: Chandrashekara CM, George MA. The Popliteal Vein Thrombosis in A Pediatric Patient: A Case Report. Journal of Orthopaedic Case Reports 2016 April – June;6(2): 72-74. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-442-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2025 Novel Case of Ipsilateral Supracondylar Fracture with Distal Radio-Ulna Fracture with Acute Compartment Syndrome: A Rare Case Report
February 1, 2025 Novel Case of Ipsilateral Supracondylar Fracture with Distal Radio-Ulna Fracture with Acute Compartment Syndrome: A Rare Case Report December 1, 2024 Patellofemoral Arthritis after Conservative Management for Post-operative Arthrofibrosis: A Case Report
December 1, 2024 Patellofemoral Arthritis after Conservative Management for Post-operative Arthrofibrosis: A Case Report April 10, 2024 Tibial Eminence Fracture and Pediatric ACL Avulsion Diagnosis and Treatment: A Case Report
April 10, 2024 Tibial Eminence Fracture and Pediatric ACL Avulsion Diagnosis and Treatment: A Case Report March 10, 2024 Operative Treatment of a Patient with a Pathological Fracture through a Large Non-ossifying Fibroma: A Case Report
March 10, 2024 Operative Treatment of a Patient with a Pathological Fracture through a Large Non-ossifying Fibroma: A Case Report