
[box type=”bio”] What to Learn from this Article?[/box]
To minimize later complications and prevent salvage procedures it is important to remove a Kuntscher nail in a young patient as soon as possible.
Case Report | Volume 6 | Issue 3 | JOCR July-Aug 2016 | Page 10-12 | Marí R, Valverde Vilamala D, León García A, Guirro P, Marqués López F. DOI: 10.13107/jocr.2250-0685.476
Authors: Marí R[1], Valverde Vilamala D[1], León García A[1], Guirro P[1], Marqués López F[1]
[1]Department of Orthopaedic Surgery, Parc de Salut Mar, Hospital de l’Esperança, Sant Josep de la Muntanya 12. 08024 Barcelona. Spain.
Address of Correspondence
Dr. Fernando Marqués-Lopez,
Department of Orthopaedic Surgery, Parc de Salut Ma, Hospital de l’Esperança, Universitat Autonoma Barcrlona, Sant Josep de la Muntanya 12. 08024 Barcelona. Spain.
E-mail: fmarques@parcdesalutmar.cat
Abstract
Introduction: The use of the Kuntscher nail has been the most important advancement in trauma surgery. One of the problems is the difficulty to remove it. A new extraction technique is described in the present case report.
Case Report: A 46-year-old man was referred for hip osteoarthritis. He had an acetabulum fracture and a femoral shaft fracture treated 30 years ago with a reamed Kuntscher femoral nail. Lateral hip approach was performed and after attempting to remove the nail with the specific tools being unsuccessful we decided to be more aggressive. Firstly, we performed a simple unicortical osteotomy on the lateral side from the proximal part to below the callus in order to decompress the femoral canal without success. Secondly, a trench in the greater trochanter around the proximal hole was performed to hit the nail from below which was still insufficient and furthermore, the hole broke when hitting the nail so we needed to drill a new hole distally. Finally, the Kuntscher nail was removed. Several cerclages closed the osteotomy and a bone graft was used to close the trench. The patient had a good evolution at one year of follow-up.
Conclusion: With this case report, we present a new salvage technique to remove an incarcerated Kuntscher nail when all the described methods have failed.
Keywords: Femoral nail, Incarcerated nail, Nail removal.
Introduction
The use of the Kuntscher nailing system for the treatment of long bone fractures has been the most important advancement in trauma surgery in recent history. Since its first implementation in a German hospital in the late 30’s, most femoral and tibial shaft fractures have been treated with it.
Removal of a Kuntscher nail is considered a routine procedure but could be really challenging. Bone ingrowth or overgrowth, damage to the proximal threads of the nail, and broken nails or locking screws may complicate the removal of intramedullary nails. Multiple techniques have been described for the removal of Kuntscher nail . The biggest challenge appears when all the described methods result in failure of removal of the nail. This article presents a case of an incarcerated femoral nail and describes a salvage procedure for nail extraction after all previously described methods have failed.
Case Report
A 46-year-old man was referred for left chronic leg pain. The patient was involved in a plane accident 30 years before sustaining a femoral shaft fracture treated with a reamed Kuntscher nail and a posterior wall acetabulum fracture treated with open reduction and internal fixation with lag screws (Fig.1).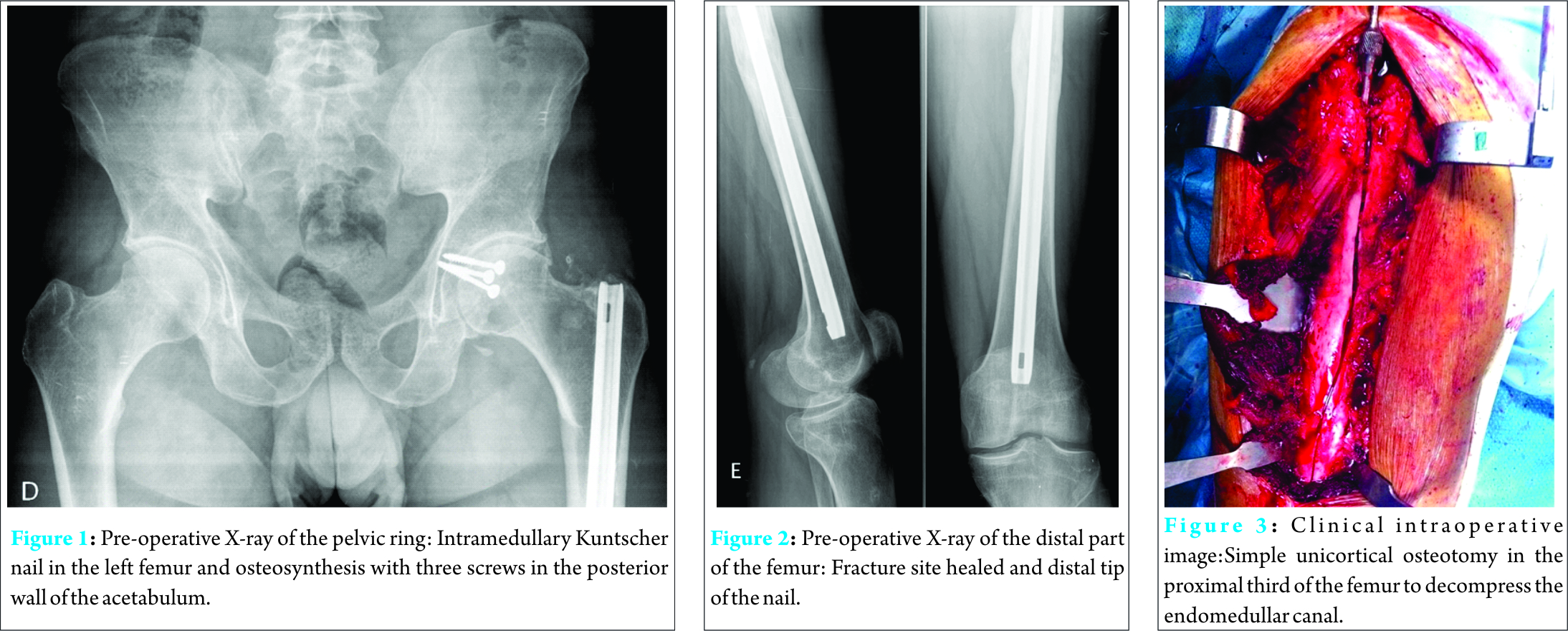
The patient came to our outpatient clinic complaining about inguinal pain and chronic leg pain with limitation of activities of daily living , although he was able to walk for more than one hour. On physical examination, the patient had no limitation of the hip range of motion. The ipsilateral knee had full range of motion and the patient did not need any crutches to walk without limping. Neurovascular examination was normal. The PostelMerléd’Aubigné scale was 14 points (4 for pain, 5 for walking and 5 for range of motion). Overall alignment of the extremity was anatomic. As a part of the initial evaluation, a blood test with infection parameters was performed and was negative for infection. Preoperative radiographs showed a healed femoral fracture in all 4 cortices with an intramedullary Kuntscher nail without locking screws and cortical thickening at the fracture site (Fig. 2). The patient was informed about the incipient arthritis of the hip and the possibility to perform a one-stage or two-stage surgery. The surgical risks were discussed with the patient, including pain after hardware removal and failure to remove the nail, specially this last point because other surgeons had tried to do the same procedure few years before and had failed after many hours of surgery. The patient decided to have two-stage surgery. Firstly, remove the nail at all costs and depending on the outcome of this first surgery he would assess the hip replacement surgery. The patient was put in a lateral position and a lateral hip approach was done. The first step was to find the proximal tip of the nail which was found seated deep in the great trochanter. The initial device used to remove the nail was the conical extraction tool that was unsuccessful after several attempts. After the overgrowth bone was removed of the proximal part of the nail a hook extraction system was engaged with difficulty. However, the nail did not move after multiple hits with a 1 kg hammer and finally the hook broke itself.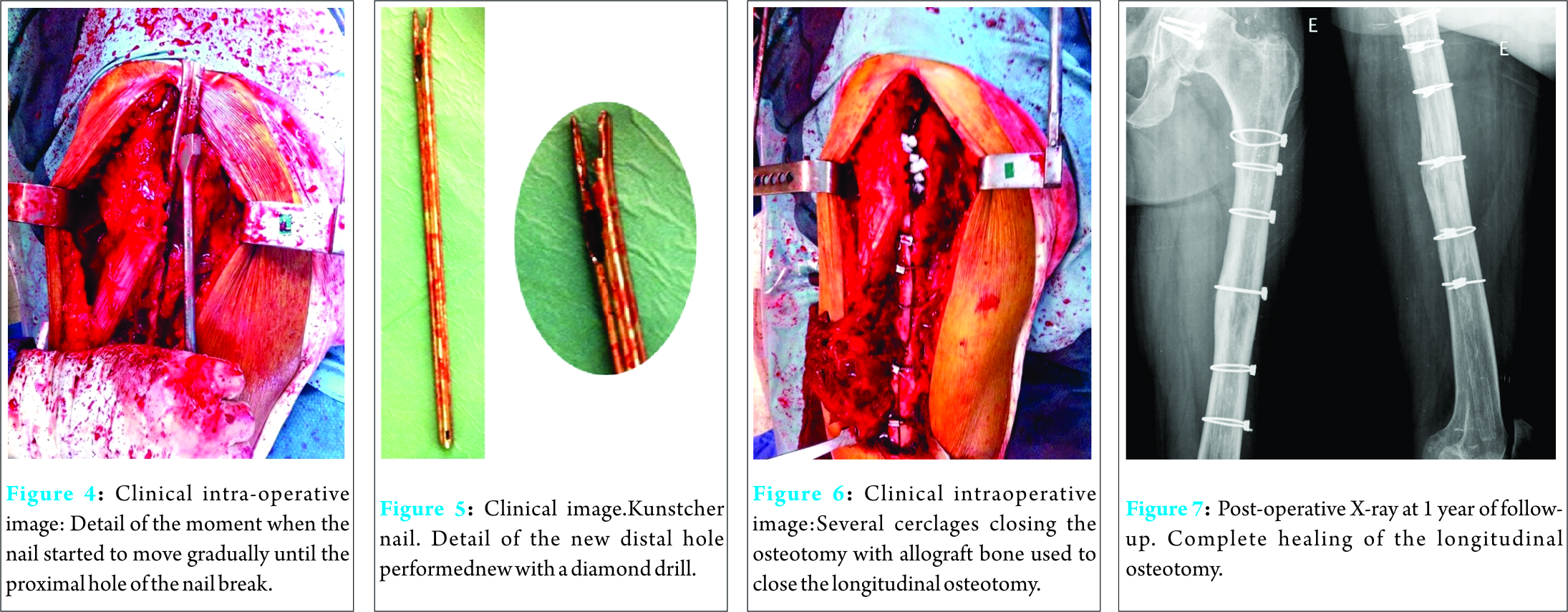
At this point, we decided to use the saw to perform a simple unicortical osteotomy in the proximal third of the femur to decompress the endomedullar canal (Fig. 3). After this decompression osteotomy we tried to hit the nail from below with an impactor engaged in the proximal hole of the nail. However, the implant remained in the same position. After trying all these different ways to remove the nail being unsuccessful, we decided to continue the longitudinal osteotomy from proximal to distal in the lateral side of the femur. The nail was found in place with on growth and overgrowth in almost entire length of the nail. A new attempt to hammer the nail from below was performed and the nail started to move gradually until the proximal hole of the nail broke (Fig. 4). After so many attempts, we did not give up and proceeded to drill a new hole distally with a diamond drill (Fig. 5) to finish the nail removal. Finally, the Kuntscher nail was removed in its entirety without any other complications. Subsequently, several cerclages and a bone allograft was used to close the longitudinal osteotomy (Fig. 6). The patient was admitted to the hospital for pain and bleeding control. On the second day of hospitalization, the patient underwent a blood transfusion as his hemoglobin was reported to be 7.1 g/dl. The patient was discharged on day 4 after antibiotic prophylaxis, deep vein thrombosis prophylaxis with low-weight-molecular heparin and ambulation with crutches without weight bearing. At 8 weeks of follow-up, patient was allowed to walk with gradual weight bearing. The patient was satisfied at 1 year of follow-up with no complications and the X-ray showed complete healing of the longitudinal osteotomy (Fig. 7). At the time of this case report, the patient is free from pain in the leg with only sporadic hip pain, so there is no indication of hip replacement surgery for the time being.
Discussion
Incarcerated intramedullary nails have been described since the beginning of their use. Various reasons have been described in the literature for nail incarceration, including excessive callus formation closing the intramedullary canal, ingrowth of bone into the nail, bone ingrowth through the locking holes and bent or broken nails. There are different techniques to remove retained intramedullary nails, most of these techniques are designed for broken nails, but others are for incarcerated nails. There is only one case similar to our case report byLindeque et al which describes removal of tibial nail using a large longitudinal osteotomy. We decided to perform a two-stage procedure especially due to the incipient arthritis of the hip. If our patient would have had advanced stage of arthritis, we could have considered a single-staged procedure with nail removal and hip replacement or a hip replacement without removing the nail. Goosen et al treated a similar case in which they cut the proximal end of the nail to the length needed in order to implant a hip arthroplasty at the top of the nail. Another possibility is to carry out a hip replacement with a resurfacing system. Mont et al used this technique on fifteen patients with femoral implants or extraarticular deformities.
Conclusion
When implant removal is difficult, a lot of techniques can be applied. We explained an aggressive procedure to remove an incarcerated nail. however, despite the aggressiveness of the procedure, the patient had a good result, and the osteotomy healed normally with no complications. This is the first case published in the literature using this longitudinal osteotomy to remove a femoral nail.
Clinical Message
The Kuntscher nail is known for its removal difficulty. In young patients, it is recommended to remove it as soon as it possible to minimize later complications. This technique is a new salvage procedure to remove a femoral Kuntscher nail.
References
1. Georgiadis GM, Heck BE, and Ebraheim NA. Technique for removal of intramedullary nails when there is failure of the proximal extraction device: a report of three cases. J Orthop Trauma 1997;11(2): 130-2.
2. Seligson D, Howard PA, and Martin R. Difficulty in removal of certain intramedullary nails. Clin Orthop Relat Res 1997;340:202-6.
3. Randall RL, Hall RJ, and Slabaugh PB. Closed removal of a segmental intramedullary rod: a technical report. J Orthop Trauma 1996; 10(5):363-5.
4. Kuntscher G, M.R., Hardware Removal of Intramedullary Nails: A surgical Technique. Georg Thieme Verlag 1945: 63-94.
5. Seibert FJ, et al. Technique tip for the removal of a “non-removable” tibial nail (Expert Tibial Nail). Injury Extra 2010;41(4):47-49.
6. Milia MJ, Vincent AB, and Bosse MJ. Retrograde removal of an incarcerated solid titanium femoral nail after subtrochanteric fracture. J Orthop Trauma 2003;17(7):521-4.
7. SonanisSV, et al. A simple technique to remove a bent femoral intramedullary nail and broken interlocking screw. J Trauma 2007;63(2): 435-8.
8. Whalley H, et al. Surgeon versus metalwork–tips to remove a retained intramedullary nail fragment. Injury 2009; 40(7):783-9.
9. Lindeque BG, Agudelo J. Incarcerated tibial nail. Orthopedics 2009;32(2):126.
10. de Amorim Cabrita HA, et al. Anterograde removal of broken femoral nails without opening the nonunion site: a new technique. Clinics (Sao Paulo), 2010;65(3):279-83.
11. Liodakis E., et al. A new technique for removal of an incarcerated expandable femoral nail. Clin Orthop Relat Res 2010; 468(5):1405-9.
12. Goosen JH and Van Hellemondt GG. Primary total hip arthroplasty with a retained intramedullary femoral nail. Acta Orthop Belg 2013;79(1): 114-6.
13. Mont MA, et al. Metal-on-metal total hip resurfacing arthroplasty in the presence of extra-articular deformities or implants. J Bone Joint Surg Am, 2008;90(3):45-51.
| How to Cite This Article: Marqués López F, Marí R, Valverde Vilamala D, León García A, Guirro P. A Technical Note for Extracting an Incarcerated Femoral Kuntscher Nail. Journal of Orthopaedic Case Reports 2016 July-Aug;6(3):10-12. Available from: https://www.jocr.co.in/wp/2016/07/10/2250-0685-476-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 Outcome of a Nail-plate Fixation Combination for a Distal Femur Fracture in a 99-year-old Patient
January 1, 2025 Outcome of a Nail-plate Fixation Combination for a Distal Femur Fracture in a 99-year-old Patient May 10, 2021 Extraction of Broken Tibial Interlock Nail with a Retrograde Hooked Guide Wire: A Novel Surgical Technique
May 10, 2021 Extraction of Broken Tibial Interlock Nail with a Retrograde Hooked Guide Wire: A Novel Surgical Technique July 10, 2024 A Perspective of Growth of Unicompartmental Knee Replacement in India – Registry Data and Global Trends
July 10, 2024 A Perspective of Growth of Unicompartmental Knee Replacement in India – Registry Data and Global Trends August 6, 2024 Avascular Necrosis of Proximal Tibia Associated with Pathological Fracture – A Rare Entity – A Case Report
August 6, 2024 Avascular Necrosis of Proximal Tibia Associated with Pathological Fracture – A Rare Entity – A Case Report