
[box type=”bio”] Learning Point for the Article: [/box]
Occupational ionizing radiation exposure monitoring for health care workers is recommended to confirm compliance with annual dose limit.
Case Report | Volume 8 | Issue 3 | JOCR May – June 2018 | Page 81-84| Abdulbaset Abosala. DOI: 10.13107/jocr.2250-0685.1122
Authors: Abdulbaset Abosala[1]
[1]Department of Orthopaedics, Dr. Gray’s Hospital, IV30 1SN, National Health Service Grampian, Elgin, Scotland, United Kingdom.
Address of Correspondence:
Dr. Abdulbaset Abosala,
Department of Orthopaedics, Dr. Gray’s Hospital, IV30 1SN, National Health Service Grampian, Elgin, Scotland, United Kingdom.
E-mail: abosala@hotmail.com
Abstract
Introduction: The purpose of the study was to have a general overview of the current understanding of occupational ionizing radiation exposure among health care workers and to explore the potential risks of such exposure to orthopedic surgeons working in national health-care setting.
Methods: The author conducted 4 months measurement of ionizing radiation exposure using body and finger dosimeter. The result used to estimate the annual occupational ionizing radiation exposure. The final results compared to previously published data with general exploration of the risk associated with such exposure through literature review.
Results: The results indicate that the current exposure is below that of the dose limit set by the International Commission on Radiological Protection (ICRP) and found to be similar to previously published data.
Conclusion: Health-care employees are the largest group exposed to ionizing radiation [1, 2]. The carcinogenic effect of high dose of radiation on humans is well documented [1, 2], but the long-term effect of exposure to low doses of ionizing radiation is not clear. Some published studies indicate increased risk of cancer among female orthopedic surgeon which may or may not be directly linked to ionizing radiation exposure. We should reinforce the main principles recommended by the ICRP: Justification, optimization of protection, and dose limitation.
Keywords: Ionizing radiation, occupational exposure, orthopedic surgeon, healthcare.
Introduction
Health-care employees are the largest group exposed to ionizing radiation [1, 2]. The carcinogenic effect of high dose of radiation on humans is well documented [1, 2], but the long-term effect of exposure to low doses of ionizing radiation is not clear. Ionizing radiation has two types of harmful effects on human tissue. The deterministic effect can be avoided when the dose is kept below the tissue-specific threshold for that particular effect [3]. However, the stochastic effect can cause cancer after a latent period that can vary from years to decades [3]. The International Commission on Radiological Protection (ICRP) has been involved in advising about radiation hazards since 1928 [3]. The ICRP also recommends radiation dose limits for both the public and workers [4] (Table 1). What is more, our current definition of occupational and public ionizing radiation exposure, as well as the definition of the stochastic and deterministic effect of radiation, is produced by the ICRP (Table 2). The ICRP also promotes three fundamental radiological principles: Justification, optimization of protection, and dose limitation [4]. In the National Health Service (NHS), it is mandatory to undergo training in the safe use of ionizing radiation. However, staff exposure is not well monitored in some areas. Orthopedic surgeons and trainees, in particular, do not carry personal dosimeters to track their individual exposure, even though they are required to the use of safety equipment including lead gowns and thyroid shields that are always available in orthopedic and trauma theaters. Large numbers of orthopedic procedures require the use of image intensifiers including fracture manipulation and fixation and joint injections. The number of cases needing the use of ionized radiation varies among orthopedic surgeons, depending largely on their sub specialities and workload [5].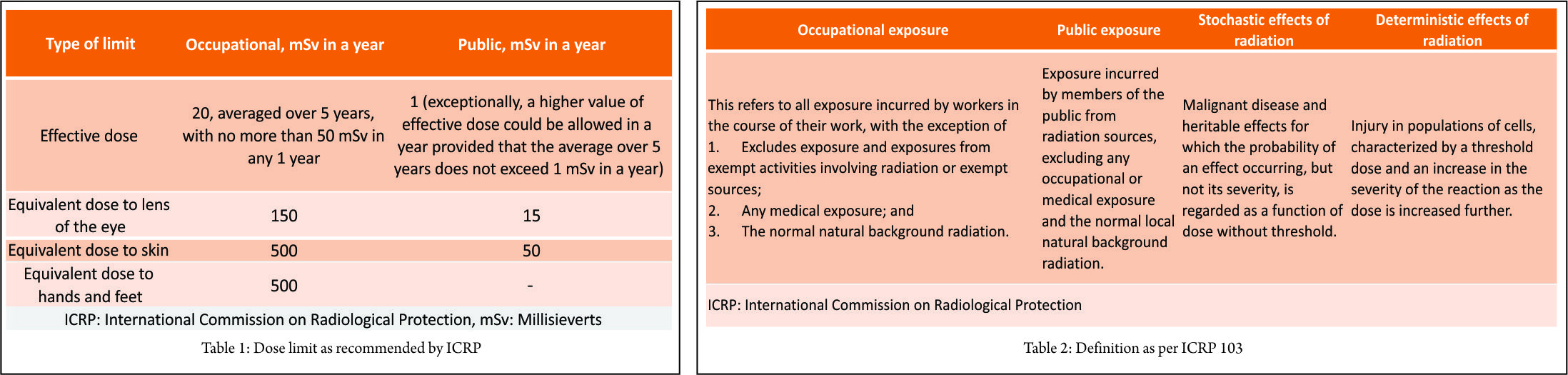
Materials and Methods
The author performs trauma and orthopedic procedures in an NHS facility in the UK. The author used dosimeters over a 4-month period, one worn over the chest area and one finger dosimeter in each hand. Dosimeters were changed every 2 months. During the trial period, the author performed in total of 82 procedures requiring the use of image intensifiers. Table 3 summarizes examples of procedures performed during the trial period. Table 4 summarizes the workload during the same period. Dose area product (DAP) and screening time are obtained directly from the image intensifier machine. Analysis of the dosimeter and the collected data were carried out after the completion of the trial period.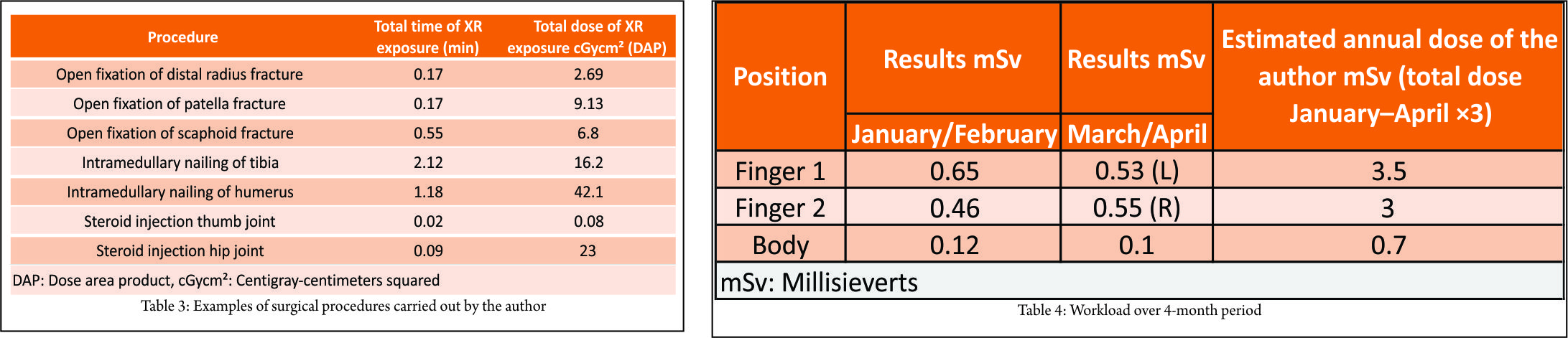
Results
The estimated annual dose in millisieverts is calculated by obtaining the total dose over the 4-month trial and multiplying it by three (Table 4). There is a large range in DAP values, varying from 0.08 to 70 centigray-centimeters squared. This indicates that the use of fluoroscopy varies significantly between the different procedures. Hence, the dose per procedure would be expected to vary depending on the case mix. Theoretically, the DAP should give the best indicator of likely operator dose because the scattered radiation is strongly linked to both incident dose and area of the beam. The monitoring indicates that doses are currently below the “others” category, which includes members of the public (Table 1). The dose is currently relative well controlled, so no further measures are required. However, monitoring should be reviewed at suitable intervals, when workloads or members of staff change or if procedures change.
Discussion
Those who are employed in health facilities represent the largest group of individuals exposed occupationally to artificial radiation sources [1, 2]. Medical surveillance is only required for classified radiation workers in the UK (i.e., those who may exceed three-tenths of a relevant dose limit during a calendar year). Literature indicated that there is a lack of understanding among health-care professional about the stochastic and deterministic effects of ionizing radiation exposure [6, 7, 8, 9, 10]. This worrisome trend seems to occur in both developing and developed countries. There is emphasis on mandatory training and use of protective measures; however, there also seems to be a casual attitude toward ionizing radiation risk because its effect is not instantaneous and not visible. Some studies indicate that the use of mini-C arm fluoroscopy can significantly reduce ionizing radiation exposure compared to that of conventional C-arm [11]. However, the use of mini-c arm is limited due to its size to procedures mainly of the wrist and hand. The risk to the eye of orthopedic surgeon due to ionizing radiation exposure is less charted territory. Certainly using protective lead eye wear is not a common practice among orthopedic surgeons practicing in the NHS. Some studies indicated that the heavy workload can reach the annual estimated dose to the lens and sometimes can exceed this level, so the use of protective lead glasses is recommended [12, 13]. Some publications have indicated that increased patient body mass index (BMI) increases a surgical team’s occupational exposure to ionizing radiation [14, 15]. Because we are seeing a current influx of large numbers of patients requiring surgery who have high BMIs, this factor must be taken into consideration. This might be an indication for regular monitoring of occupational radiation exposure for surgeons who deal with obese patients. It is well known that acute exposure to high levels of ionizing radiation carries carcinogenesis effects [1, 2]. However, the long-term effect of exposure to very low levels of ionizing radiation is less established. In particular, exposure among medical professional is not extensively studied. Two published studies [16, 17] identified an increase of breast cancer among female orthopedic surgeons compared to the general United States population. In other studies [18, 19], there is evidence of increased prevalence of cancer among orthopedic female surgeons, which may or may not be directly linked to ionizing radiation exposure. As per ICRP 2007, the cancer estimate due to low dose of radiation is 5.5×10-2 per sievert [4].
Conclusion
Our monitoring results seem similar to previously published figures in the literature [3, 20, 21]. Even though it is reassuring that the figures indicate the occupational exposure is currently below that of the dose limit set by the ICRP, this situation should not promote a culture of complacency when it comes to ionizing radiation. We should promote the culture of the main three principles recommended by the ICRP [4]: Justification, optimization of protection, and dose limitation.
Clinical Message
Occupational ionizing radiation exposure among health care worker can cause harmful effect on health. Monitoring of occupational ionizing radiation is recommended to establish the annual exposure dose and determine that it is within the recommended level based on the recommendation by ICRP.
References
1. United Nations Scientific Committee on the Effects of Atomic Radiation Sources and Effects of Ionising Radiation, Report to the General Assembly, with Scientific Annex; 2000.
2. United Nations Scientific Committee on the Effects of Atomic Radiation, Effects of Ionizing Radiation. UNSCEAR 2006 Report to the General Assembly with Scientific Annexes; 2008.
3. Hynes DE, Conere T, Mee MB, Cashman WF. Ionising radiation and the orthopaedic surgeon. J Bone Joint Surg Br 1992;74:332-4.
4. International Commission on Radiological Protection. The 2007 Recommendation of the International Commission on Radiological Protection. ICRP Publication 103. Ann 2007;37:2-4.
5. Hardman J, Elvey M, Shah N, Simson N, Patel S, Anakwe R. Defining reference levels for intra-operative radiation exposure in orthopaedic trauma: A retrospective multicentre study. Injury 2015;46:2457-60.
6. Jacob K, Vivian G, Steel JR. X-ray dose training: Are we exposed to enough? Clin Radiol 2004;59:928-34.
7. Soye JA, Paterson A. A survey of awareness of radiation dose among health professionals in Northern Ireland. Br J Radiol 2008;81:725-9.
8. Zakeri F, Shakeri M, Rajabpour MR, Farshidpour MR, Mianji F. Physicians’ knowledge about radiation dose and possible risks of common medical tests: A survey in Iran. Radiat Prot Dosimetry 2016;172:311-6.
9. Hager K, Anissa B, Khaled AK, Mondher K, and Azza H. Radiation protection in orthopedic surgery at the Charles Nicolle hospital of Tunis. Tunis Med 2014;92:311-7.
10. Khan IA, Kamalasekaran S, Fazal MA. Risk of ionising radiation to trainee orthopaedic surgeons. Acta Orthop Belg 2012;78:106-10.
11. Sung KH, Min E, Chung CY, Jo BC, Park MS, Lee K. Measurements of surgeons’ exposure to ionizing radiation dose: Comparison of conventional and mini C-arm fluoroscopy. J Hand Surg Eur 2016;41:340-5.
12. Romanova K, Vassileva J, Alyakov M. Radiation exposure to the eye lens of orthopaedic surgeons during various orthopaedic procedures. Radiat Prot Dosimetry 2015;165:310-3.
13. Burn’s S, Thornton R, Dauer LT, Quinn B, Miodownik D, Hak DJ. Leaded eyeglasses substantially reduce radiation exposure of the surgeon’s eyes during acquisition of typical fluoroscopic views of the hip and pelvis. J Bone Joint Surg Am 2013;17:1307-11.
14. Canham CD, Williams RB, Schiffman S, Weinberg EP, Giordano BD. Cumulative radiation exposure to patients undergoing arthroscopic hip preservation surgery and occupational radiation exposure to the surgical team. Arthroscopy 2015;31:1261-8.
15. Baratz MD, Hu YY, Zurakowski D, Appleton P, Rodriguez EK. The primary determinants of radiation use during fixation of proximal femur fractures. Injury 2014;45:1614-9.
16. Valone LC, Chambers M, Lattanza L, James MA. Breast radiation exposure in female orthopaedic surgeons. J Bone Joint Surg Am 2016;98:1808-13.
17. Chou LB, Chandran S, Harris AH, Tung J, Butler LM. Increased breast cancer prevalence among female orthopedic surgeons. J Womens Health (Larchmt) 2012;21:683-9.
18. Chou LB, Lerner LB, Harris AH, Brandon AJ, Girod S, Butler LM, et al. Cancer prevalence among a cross-sectional survey of female orthopedic, urology, and plastic surgeons in the united states. Womens Health Issues 2015;25:476-81.
19. Zielinski JM, Garner MJ, Band PR, Krewski D, Shilnikova NS, Jiang H, et al. Health outcomes of low-dose ionizing radiation exposure among medical workers: A cohort study of the Canadian national dose registry of radiation workers. Int J Occup Med Environ Health 2009;22:149-56.
20. Barry TP. Radiation exposure to an orthopaedic surgeon. Clin Orthop Relat Res 1984;182:160-4.
21. Sugarman ID, Adam I, Bunker TD. Radiation dosage during AO locking femoral nailing. Injury 1988;19:336-8.
 |
| Dr. Abdulbaset Abosala |
| How to Cite This Article: Abosala A. A Report on Occupational Ionizing Radiation Exposure by an Orthopedic Surgeon in a National Health-care Setting – Clinical Case Perspective. Journal of Orthopaedic Case Reports 2018. May- June; 8(3): 81-84. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 December 4, 2020 Reconstruction of Capitellar Defect using Freeze-dried Cadaveric Allograft – A Case Report
December 4, 2020 Reconstruction of Capitellar Defect using Freeze-dried Cadaveric Allograft – A Case Report October 28, 2014 Auto Bone Banking: Innovative Method for Bone Preservation
October 28, 2014 Auto Bone Banking: Innovative Method for Bone Preservation January 10, 2016 Identical Twins with Infantile Systemic Hyalinosis: Case study and review of literature
January 10, 2016 Identical Twins with Infantile Systemic Hyalinosis: Case study and review of literature May 10, 2019 A Case Report of Congenital Hallux Valgus from an Incomplete Preaxial Polydactyly without a Supernumerary Digit
May 10, 2019 A Case Report of Congenital Hallux Valgus from an Incomplete Preaxial Polydactyly without a Supernumerary Digit