
[box type=”bio”] Learning Point of the Article: [/box]
Risk of Heterotopic Ossification with suprapatellar intramedullary nailing needs to be included in consent process.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 15-17 | Nasiur Rehman, Alex Trompeter, Hugo Guthrie, Martin Goddard. DOI: 10.13107/jocr.2250-0685.1348
Authors: Nasiur Rehman[1], Alex Trompeter[1], Hugo Guthrie[1], Martin Goddard[1]
[1]Department of Trauma and Orthopaedics, St George’s University Hospital, London.
Address of Correspondence:
Mr. Nasiur Rehman,
Department of Trauma and Orthopaedics, St George’s University Hospital NHS Foundation Trust, Blackshaw Road, Tooting, London, SW17 0QT, UK.
E-mail: drnaseerrehman@yahoo.co.uk
Abstract
Introduction: Tibial shaft fractures are common fractures seen in trauma and orthopedic practice today. The majority of these fractures are treated with intramedullary nailing (IMN) which is rapidly becoming a gold standard. The procedure itself is performed by either a suprapatellar approach or infrapatellar approach. Suprapatellar approach is gaining popularity due to relative ease of insertion, decreased associated risk of anterior knee pain, and more accurate reduction. We report a case of heterotopic ossification noted in the knee following IMN of tibia performed using a suprapatellar approach.
Case Report: A 27-year-old male, having sustained a left, Gustilo IIIB tibial shaft fracture following a motor vehicle accident, underwent a reamed intramedullary nail fixation performed through a suprapatellar approach. Two months later, he presented with intra-articular heterotopic ossification which was limiting his knee movement. He then underwent arthroscopic removal of the bony fragments which resolved his symptoms.
Conclusion: An extensive search of literature did not yield any reported incidence of heterotopic ossification associated with IMN performed through a suprapatellar approach. We present this case report to raise awareness that although IMN through a suprapatellar approach is a safe approach, it does have associated risk of heterotopic ossification which needs to be included in the consent process.
Keywords: Tibial shaft fracture, Intramedullary nailing, Suprapatellar approach, Heterotopic ossification.
Introduction
Tibial shaft fractures are common with a reported incidence of 16.9/100,000/year [1]. The majority of tibial shaft fractures are treated within tramedullary nailing (IMN) which can be performed using suprapatellar or infrapatellar approach. Suprapatellar approach is increasing in popularity due to relative ease of nail insertion and decreased incidence of anterior knee pain; this has led many surgeons to use it as a preferred technique. A recent meta-analysis by Wang et al. [2] reported reduced fluoroscopy time, better functional outcome, and more accurate reduction of fractures with suprapatellar IMN (SPN) which is a significant advantage in contrary to infrapatellar approach. Our extensive search of literature did not suggest any increase in risk associated with SPN and it seems that it is rapidly becoming a standard approach to treating tibial shaft fractures.
Case Report
A 27-year-old male presented to our major trauma center having sustained a left Gustilo IIIb tibial shaft fracture following a motor vehicle accident. His injury was initially managed with wound debridement, irrigation, topical negative pressure dressing, and temporary external fixator. He subsequently underwent an anterolateral thigh free flap and reamed locked SPN with 1 cm tibial shortening to improve cortical apposition. After a period of rehabilitation, he was discharged from our institute. Two months later, he presented with a 30° block to full extension of knee. Radiographs demonstrated an intra-articularbony fragment (Fig. 1). Arthroscopy was performed which bony fragment impinging in the anterior aspect of the knee joint blocking full extension (Fig. 2a and b). The fragment was removed arthroscopically and his symptoms completely resolved (Fig. 3).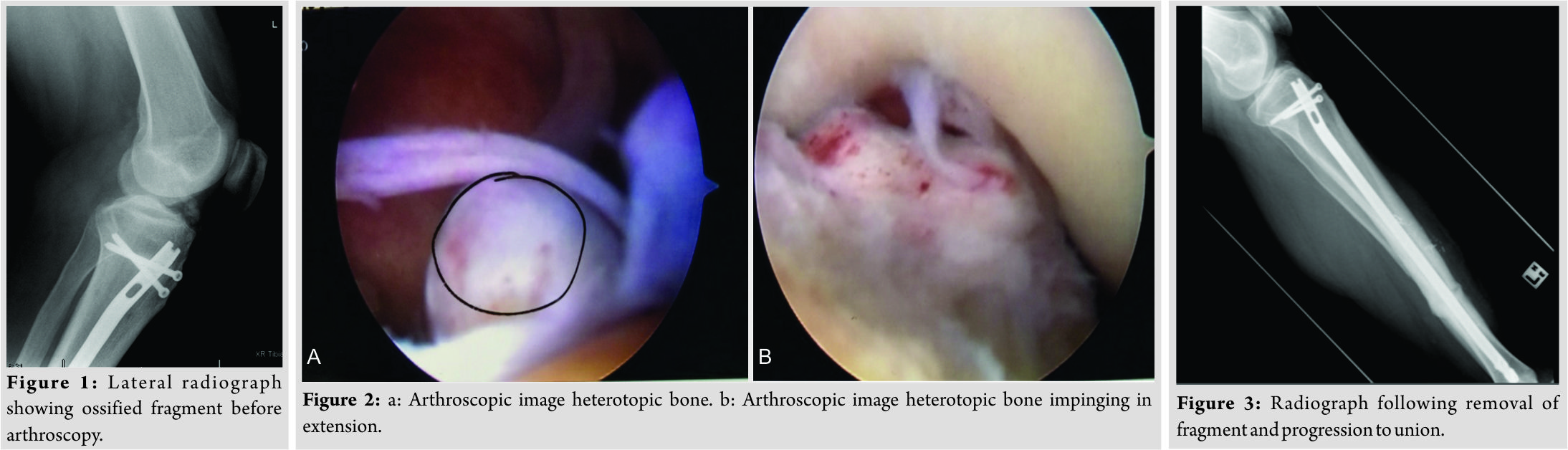
Discussion
Supra patellar nailing for tibial shaft fractures is a relatively new technique increasing in popularity due to simple operative setup, protection of soft tissues in open fractures, facilitation of fracture reduction in proximal third fractures and decreased incidence of anterior knee pain compared to the infra patellar approach [3-7]. Disadvantages may include increased risk of injury to the menisci, intermeniscal ligament and articular surfaces [8, 9]. We believe that it is essential to keep the sleeve through which reamers are passed in close contact with the entry point on the tibia and to thoroughly irrigate the knee at the end of the procedure to ensure that any reaming debris generated is not retained in the knee. Failure to do so can result in the formation of heterotopic bone. Trauma surgeons should take particular care with these parts of the procedure and potential complication of HO should be included in the consent process.
Conclusion
Heterotopic bone formation in the knee is not a reported complication with SPN, we believe that reaming debris generated during suprapatellar nailing is a contributing factor; hence, the knee should be thoroughly washed to remove the debris to avoid this potential complication.
Clinical Message
SPN is a relatively new technique, complication associated with its use is not common, but we believe that they should be reported in order that experience with this technique is shared. Our case report highlights potential risk of developing heterotopic ossification with this approach which a trauma surgeon should be aware of while consenting and performing the procedure.
References
1. Larsen P, Elsoe R, Hansen SH, Graven-Nielsen T, Laessoe U, Rasmussen S. Incidence and epidemiology of tibial shaft fractures. Injury 2015;46:746-50.
2. Wang C, Chen E, Ye C, Pan Z. Suprapatellar versus infrapatellar approach for tibia intramedullary nailing: A meta-analysis. Int J Surg 2018;51:133-9.
3. Brink O. Suprapatellar nailing of tibial fractures: Surgical hints. Curr Orthop Pract 2016;27:107-12.
4. Katsoulis E, Court-Brown C, Giannoudis PV. Incidence and aetiology of anterior knee pain after intramedullary nailing of the femur and tibia. J Bone Joint Surg Br 2006;88:576-80.
5. Jones M, Parry M, Whitehouse M, Mitchell S. Radiologic outcome and patient-reported function after intramedullary nailing: A comparison of the retropatellar and infrapatellar approach. J Orthop Trauma 2014;28:256-62.
6. Väistö O, Toivanen J, Paakkala T, Järvelä T, Kannus P, Järvinen M.Anterior knee pain after intramedullary nailing of a tibial shaft fracture: An ultrasound study of the patellar tendons of 36 patients. J Orthop Trauma 2005;19:311-6.
7. Morandi M, Banka T, Gaiarsa GP, Guthrie ST, Khalil J, Hoegler J. Intramedullary nailing of tibial fractures: Review of surgical techniques and description of a percutaneous lateral suprapatellar approach. Orthopedics 2010;33:172-9.
8. Beltran MJ, Collinge CA, Patzkowski JC, Masini BD, Blease RE, Hsu JR. Intra-articular risks of suprapatellar nailing. Am J Orthop (Belle Mead NJ) 2012;41:546-50.
9. Polonet D. Suprapatellar nailing technique for tibial fractures. TechOrthop 2014;29:145-9.
 |
 |
 |
 |
| Mr. Nasiur Rehman | Mr. Alex Trompeter | Mr. Hugo Guthrie | Mr. Martin Goddard |
| How to Cite This Article: Rehman N, Trompeter A, Guthrie H, Goddard M. Heterotopic Ossification following Suprapatellar Intramedullary Nailing. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2):15-17. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Management of a Case of Adult Mid-Shaft Femur Fracture in Osteogenesis Imperfecta by Long Proximal Femoral Nail: A Case report
December 1, 2025 Management of a Case of Adult Mid-Shaft Femur Fracture in Osteogenesis Imperfecta by Long Proximal Femoral Nail: A Case report November 1, 2025 Incidence and Functional Impact of Malrotation after Intramedullary Nailing of Femoral Shaft Fractures: A Prospective Computed Tomography-based Observational Study
November 1, 2025 Incidence and Functional Impact of Malrotation after Intramedullary Nailing of Femoral Shaft Fractures: A Prospective Computed Tomography-based Observational Study November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre
November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre October 1, 2025 Analysis of proximal plating versus intramedullary nailing in the treatment of extra-articular proximal tibial fracture: A randomized prospective study
October 1, 2025 Analysis of proximal plating versus intramedullary nailing in the treatment of extra-articular proximal tibial fracture: A randomized prospective study