
[box type=”bio”] Learning Point of the Article: [/box]
Our case highlights the benefit of using a ring fixator device to achieve good purchase and traction in osteoporotic bone when managing gap non-union patella fractures in elderly patients.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 69-71 | Ossama Al-Obaedi, Raj RThakrar, Rik Kundra, Mohammad J Iqbal. DOI: 10.13107/jocr.2250-0685.2250-0685.1376
Authors: Ossama Al-Obaedi[1], Raj RThakrar[1], Rik Kundra[2], Mohammad J Iqbal[1]
[1]Department of Trauma and Orthopaedic Surgery, Walsall Healthcare NHS Trust, Walsall, United Kingdom.
[2]Department of Trauma and Orthopaedic Surgery, Mediclinic Park view Hospital, Dubai, UAE.
Address of Correspondence:
Dr. Ossama Al-Obaedi,
Moat Road, Walsall, WS2 9PS, United Kingdom.
E-mail: oalobaedi@gmail.com
Abstract
Introduction: Gap non-union patella fractures are rare but can be particularly challenging for the orthopedic surgeon. We report a case of a 12 cm gap non-union patella fracture in a patient with osteoporosis and its surgical management, functional outcome, and implications on clinical practice.
Case Report: A 73-year-old fully independent female with a background of osteoporosis was referred to our outpatient knee clinic. She reported a fall from stairs following an initial soft-tissue injury to the left knee 6 months prior. She has had progressive decline in mobility since the injury and was restricted to a wheelchair when she was seen in clinic. On examination, she had significant wasting of the quadriceps on the left side. Her range of movement was from 40° extensor lag to 90° flexion actively. Passive movements of the knee were preserved. She was unable to straight leg raise. Plain radiographs revealed a 12 cm gap non-union of her left patella. The patient was managed operatively in a two-staged approach. The first stage involved application of ring fixator device to achieve gradual skeletal traction from 5 to 12 lbs over a period of 10 days. The second stage involved conventional tension band wiring.
Conclusion: At 1-year follow-up, the patient achieved full independent mobility. This case highlights the efficacy of a two-staged approach in the management of gap non-union patella fractures in patients with poor bone quality.
Keywords: Elderly, Fracture fixation, Non-union, Patella fracture
Introduction
The management of gap non-union patella fractures continues to be a challenge in orthopedic practice. It is often quoted in the literature that the incidence of these cases ranges between 2.7 and 12.5% [1, 2]. The particular challenges relate to soft-tissue contractures, proximal migration of the bony fragment with associated extensor lag and knee stiffness [3]. In addition, if the extensor retinaculum is torn, the quadriceps tendon will displace the superior fragment proximally which becomes impossible to manage non-operatively [4]. There is limited evidence to help guide clinicians in the management of these complex cases which is clear from the various treatments offered by orthopedic surgeons in different centers [5]. There are several case series in the literature that describes surgical techniques involving single-staged versus two-staged approaches to reconstruction of the extensor mechanism with variable functional outcomes. The vast majority of these case series present experience in a young population with good bone stock allowing for good bone fixation. Our case demonstrates a novel technique of a two-staged repair of the extensor mechanism in an elderly patient with poor bone quality following delayed presentation of a 12 cm gap non-union of the patella.
Case Report
A 73-year-old fit and active female with a background of osteoporosis presented to our outpatient knee clinic following a fall from stairs after an original soft-tissue injury to the left knee 6 months prior. She reported progressive decline in mobility with difficulty extending the left knee. The patient did not want to seek medical attention and was referred by the general practitioner when her mobility became restricted to a wheelchair. On examination, the patient was dependent on a wheelchair. There was significant wasting of the quadriceps on the left. Her left knee range of movement was from 40° extensor lag to 90° flexion actively. Passive movements of the left knee were preserved. She was unable to straight leg raise (SLR). Plain radiographs of the left knee demonstrated a 12 cm gap non-union of the left patella (Fig. 1). A decision was made to proceed with a two-staged reconstruction of the extensor mechanism. The first stage involved application of skeletal traction on the proximal fragment (Fig. 2 and 3). Due to the patient’s poor bone quality, the decision was made to apply tension wire skeletal traction using a ring fixator device with one wire passing through the bone and a second wire through the quadriceps tendon (Fig. 4). Following this, progressive traction was applied from 5 to 12 lbs over a period of 10 days. Once adequate mobilization of the proximal patella fragment was achieved, we proceeded to the second stage which involved a conventional tension band wiring to achieve definitive fixation (Fig. 4). At 1-year follow-up, the patient had achieved full independent mobility. She demonstrated full extension of the knee joint with preserved active SLR. She was subsequently discharged from follow-up.
A decision was made to proceed with a two-staged reconstruction of the extensor mechanism. The first stage involved application of skeletal traction on the proximal fragment (Fig. 2 and 3). Due to the patient’s poor bone quality, the decision was made to apply tension wire skeletal traction using a ring fixator device with one wire passing through the bone and a second wire through the quadriceps tendon (Fig. 4). Following this, progressive traction was applied from 5 to 12 lbs over a period of 10 days. Once adequate mobilization of the proximal patella fragment was achieved, we proceeded to the second stage which involved a conventional tension band wiring to achieve definitive fixation (Fig. 4). At 1-year follow-up, the patient had achieved full independent mobility. She demonstrated full extension of the knee joint with preserved active SLR. She was subsequently discharged from follow-up.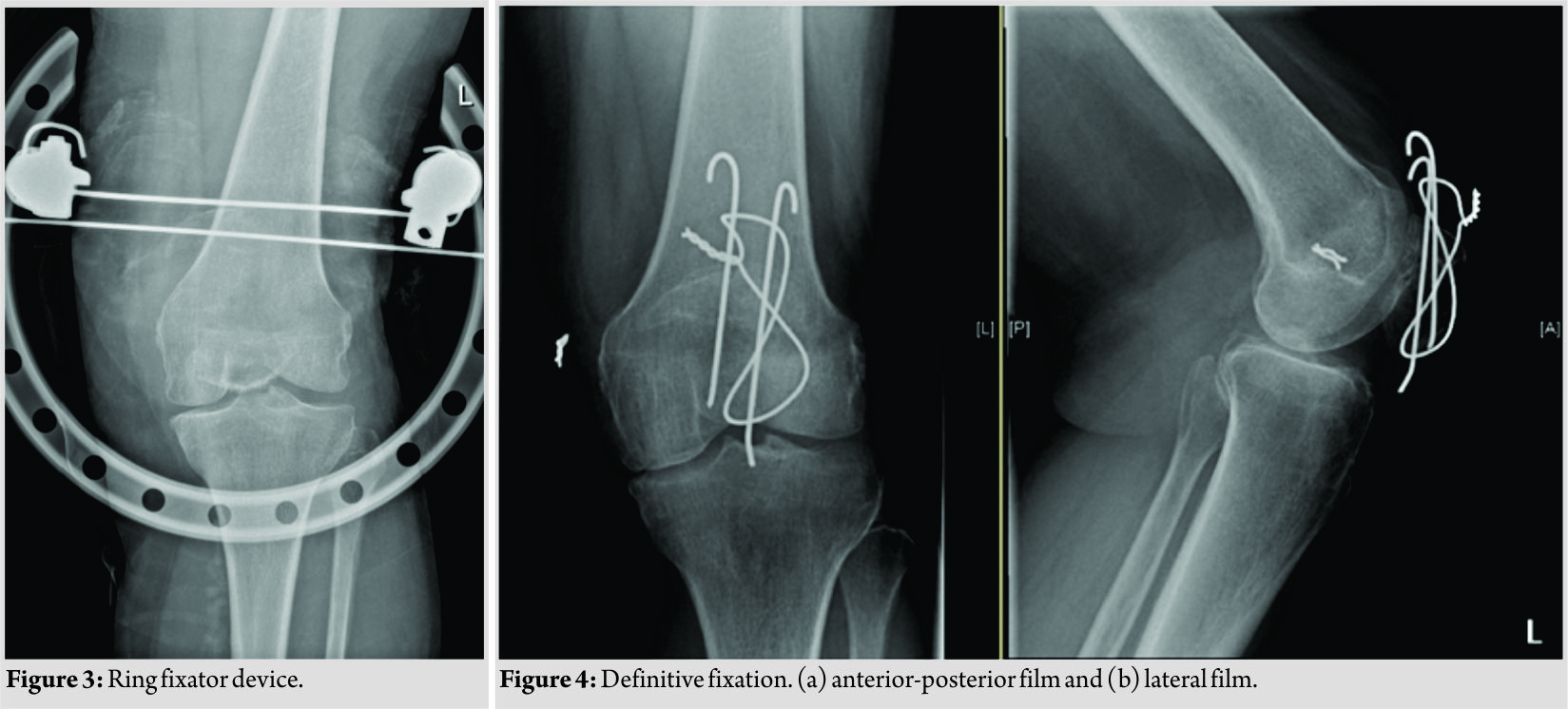
Discussion
The biggest challenge with gap non-union patella fractures is the difficulty of joining the displaced fragments due to soft-tissue contractures from long-standing injury [6]. In general, the management options for patella fractures depend on the patient’s functional demands [5]. Patients with high functional demands depend on the patella’s function as a lever for knee extension to supplement the force of the quadriceps [7]. In these group of patients, surgical management is advocated. A study by Garg et al. compared the various surgical methods of treating patellar non-unions. They compared v-y quadsplasty and tension band wiring, patellar traction and tension band wiring (without v-y quadsplasty), and patellar traction followed by partial or total patellectomy [8]. In terms of best functional outcome, their results showed that patients who had patellar traction followed by tension band wiring had the best results. The group of patients who had a patellectomy had the second-best outcomes. However, patients who underwent a v-y quadsplasty had the worst outcomes with poor functional results and higher complication rates [8]. Another study by Uvaraj et al. compared tension band wiring to patellectomies in neglected fractures of the patella. They noted that the function of the quadriceps after a patellectomy was significantly compromised. They reported a reduction of the efficiency of the extensor mechanism by about 30% [9]. In addition, it is believed that calcifications of the quadriceps tendon following a patellectomy also contribute to poor functional results [10]. They concluded that tension band wiring is superior to patellectomies in terms of patient functional outcomes [9]. There are several case reports that have tested both the one-staged and two-staged approaches to the management of non-union patella fractures. In one case, aIlizarov technique was implemented to bring the fragment pieces together and allow union without definitive fixation with good results [6]. In another case, a two-staged approach was used and a compressing assembly was implemented followed by tension band wiring as the second stage for definitive fixation [3]. Interestingly, there is little literature on the management of such fractures in the elderly population with all studies focusing on patients under the age of 60. Our patient shared the morphology of fractures described in other studies but differed in the biology of the fracture. Achieving traction in osteoporotic bone is a real challenge that can compromise the success of the procedure. Our technique of using a ring fixator device to pass a wire through the patella fragment and another wire through the quadriceps tendon is unique. This allowed good purchase in poor quality bone and contributed to the success of the procedure and the excellent functional outcome. From our experience, we advocate that these cases should be managed with a two-staged reconstruction of the extensor mechanism. The period of traction allows adequate stretching of the soft tissue to prevent the need for aggressive release in the form of a v-y quadsplasty.
Conclusion
The two-staged approach to the management of gap non-union patella fractures is an effective way of restoring the extensor mechanism. Use of a ring fixator with wires passing through the patella and quadriceps tendon in the first stage allows for good purchase and traction in osteoporotic bone. This in turn facilitates the definitive fixation in the second stage. Our case shows that good functional outcome is achievable without the need for a v-y quadsplasty or a patellectomy.
Clinical Message
Gap non-union patella fractures remain a challenge in orthopedic practice. We hope our case will help orthopedic surgeons consider a two-staged approach in the management of these injuries. Our technique has proven successful in managing a patient with osteoporotic bone quality which we hope will give confidence in managing patients of this age group.
References
1. Tripathi SK, Pant A, Agarwal NK, Kumar S, Krishna V. Two staged surgery for gap non-union of patella fracture: A good alternative. Ann Int Med Dent Res 2016;2:1-3.
2. Klassen JF, Trousdale RT. Treatment of delayed and nonunion of the patella. J Orthop Trauma 1997;11:188-94.
3. Singhal V, Mittal D, Lal H, Khare R, Sharma SC. Gap non-union of patella: A treatment dilemma. J Orthop 2010;12:8-11.
4. Carpenter JE, Kasman RA, Patel N, Lee ML, Goldstein SA. Biomechanical evaluation of current patella fracture fixation techniques. J Orthop Trauma 1997;11:351-6.
5. Nathan ST, Fisher BE, Roberts CS, Giannoudis PV. The management of nonunion and delayed union of patella fractures: A systematic review of the literature. IntOrthop 2011;35:791-5.
6. Baruah RK. Modified ilizarov in difficult fracture of the patella. A case report. J Orthop Case Rep 2016;6:26-8.
7. Scolaro J, Bernstein J, Ahn J. Patellar fractures. ClinOrthopRelat Res 2011;469:1213-5.
8. Garg P, Sahoo S, Satyakam K, Biswas D, Garg A, Mitra S, et al. Patellar nonunions: Comparison of various surgical methods of treatment. Indian J Orthop 2012;46:304-11.
9. Uvaraj NR, MayilVahanan N, Sivaseelam A, Mohd Sameer M, Basha IM. Surgical management of neglected fractures of the patella. Injury 2007;38:979-83.
10. Sorensen KH. The late prognosis after fracture of the patella. ActaOrthopScand 1964;34:198-212.
 |
 |
 |
 |
| Dr. Ossama Al-Obaedi | Dr. Raj R Thakrar | Dr. Rik Kundra | Dr. Mohammad J Iqbal |
| How to Cite This Article: Al-Obaedi O, Thakrar R R, Kundra R, Iqbal M J. Gap Non-union Patella Fractures: Case Report and Review of the Literature. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 69-71. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2025 A Case Report Scaphoid Non-Union Management: With Dual Bone Grafting
July 1, 2025 A Case Report Scaphoid Non-Union Management: With Dual Bone Grafting December 1, 2025 An Unusual Case of Patellar Osteochondroma in an Elderly Woman: A Rare Site and Age of Presentation
December 1, 2025 An Unusual Case of Patellar Osteochondroma in an Elderly Woman: A Rare Site and Age of Presentation December 1, 2025 Hook Plate Fixation of an Isolated Pisiform Fracture with a Small Proximal Fragment: A Case Report
December 1, 2025 Hook Plate Fixation of an Isolated Pisiform Fracture with a Small Proximal Fragment: A Case Report November 1, 2025 Simultaneous Bilateral Extracapsular Proximal Femur Fracture in an 85-year-old Male Patient. A Case Report
November 1, 2025 Simultaneous Bilateral Extracapsular Proximal Femur Fracture in an 85-year-old Male Patient. A Case Report