
[box type=”bio”] Learning Point of the Article: [/box]
In the Indian setting, double-loaded suture anchors can be easily created from the technique described to pass sutures through non-loaded suture anchor.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 80-83 | Karthik Vishwanathan. DOI: 10.13107/jocr.2250-0685.1382
Authors: Karthik Vishwanathan[1]
[1]Department of Orthopaedics, Pramukhswami Medical College, Karamsad, Gujarat, India.
Address of Correspondence:
Dr. Karthik Vishwanathan,
Department of Orthopaedics, Pramukhswami Medical College and Shri Krishna hospital, Gokal Nagar, Karamsad, Gujarat – 388325, India.
E-mail: karthik_vishwanathan@yahoo.com
Abstract
Introduction: Suture anchors are used in the repair of rotator cuff repair, bankart’s repair, SLAP repair, tendoachilles avulsion type injury, bony avulsion of medial collateral ligament of the knee, etc. The cost of preloaded suture anchors varies from INR 4500 to 10,000. Double-loaded suture anchors are better than single-loaded suture anchors in terms of having more hold in the soft tissues and having multiple anchoring points. Non-loaded screw type suture anchors are available with their inserter devices through which one suture stranded can be passed to create single-loaded suture anchor. However, passing two sutures through the eyelet of the suture anchor and subsequently passing two sutures through the long tubular cannulated suture anchor inserter device can be fiddly, time-consuming and difficult to pass because the sutures can get entangled within this device and not pass inside the inserter device. Hence, a technique was devised to simultaneously pass both sutures through the eyelet of the suture anchor and subsequently through the suture anchor inserter device. This method of loading suture anchors has not been described previously in literature.
Technique: A single number 1–0 Ethilon is used to shuttle two sutures of number 2 Ethibond through the suture anchor insertion device after passing the two Ethibond sutures through the eyelet of a 5mm non-loaded suture anchor. This technique saves considerable time during the surgical procedure and can be easily taught to scrub nurses. The greatest cost benefit is seen in cases where more than two suture anchors have to be inserted. The above technique has been used in patients with rotator cuff repair, biceps tenodesis, tendoachilles avulsion repair with great degree of success and no case of failure of suture or suture anchor seen in any of the cases.
Conclusion: The cost of a double-loaded suture anchor using our method is INR 1950 which is much cheaper compared to the available preloaded suture anchors. This is a novel, time saving, simple, cheap, and easy and easily replicable method to create an effective twin-loaded suture anchor from a non-loaded suture anchor.
Keywords: Rotator cuff, Suture, Suture anchor, Tendo Achilles, Tendon repair.
Introduction
When tendons rupture from/near their insertion then lack of soft tissue distally precludes end-to-end repair and in these instances, suture anchors have revolutionized treatment of such injuries. Suture anchors are implants that are used to repair broken soft tissues to its anatomical footprint and they promote soft tissue to bone healing. Suture anchors are classified as single-loaded suture anchor if single suture passes through the eyelet of the anchor (Fig. 1) and as double-loaded suture anchor if there are two sutures passing through the eyelet of the suture anchor (Fig. 1). Double-loaded suture anchors increase the strength of fixation of the suture material onto the tendon by increasing the number of sutures passed in the tendon [1]. It is better to use double suture anchors because lesser holes need to be drilled in bone and fewer implants are required to complete similar pattern of repair as compared to single-loaded suture anchors [2, 3]. This leads to reducing of cost and double-loaded suture anchors might be biomechanically superior to single-loaded suture anchors [2, 3]. Suture anchors are used in repair of rotator cuff repair [4], bankart’s repair [5], SLAP repair [6], rupture of the distal end of biceps brachii [7], tendo Achilles avulsion type injury [8], lateral ligaments of the ankle [9], medial patellofemoral ligament reconstruction [10], etc. The cost of preloaded suture anchors varies from INR 6500 to 10,500. In our country, both preloaded and non-loaded suture anchors (Fig. 2) are available. In the Indian context, wherein the cost of the implant can act as a constraining factor in patient’s choice for treatment; it is imperative to improvise a cheap but effective method to create a twin-loaded suture anchor.
Technique
Consent and approval for publication of this technique were obtained from the Institutional Ethics Committee. The suture anchor is introduced using a cannulated type inserter device (Fig.1). The inserter device is long and tubular and has two ends: Distal end is the narrow end where the suture anchor is attached (suture anchor inserting end),and the proximal end is wide so that it can be easily gripped by the surgeon’s hand (holding end). The internal width of the cannulated device is approximately 3 mm diameter and the challenge is to pass four strands of the sutures (for a twin-loaded suture anchor) through the cannulated device as the sutures can get entangled inside the cannulated device or negotiating through the 15 cm long tubular device can be fiddly when attempted using surgical gloves intraoperatively. Some instrument suppliers provide a thin flimsy lasso wire made from stainless steel that is inserted in an antegrade fashion from the gripping end of the suture anchor holder, and the steel wire loop comes out from the suture anchor inserting the end of the introducer device. Ethibond is a braided polyester multifilament suture. It is possible to only pass a single strand of number 2 Ethibond. The wire loop is so flimsy that it breaks when we try to pass both strands of number 2 Ethibond simultaneously (Fig. 3).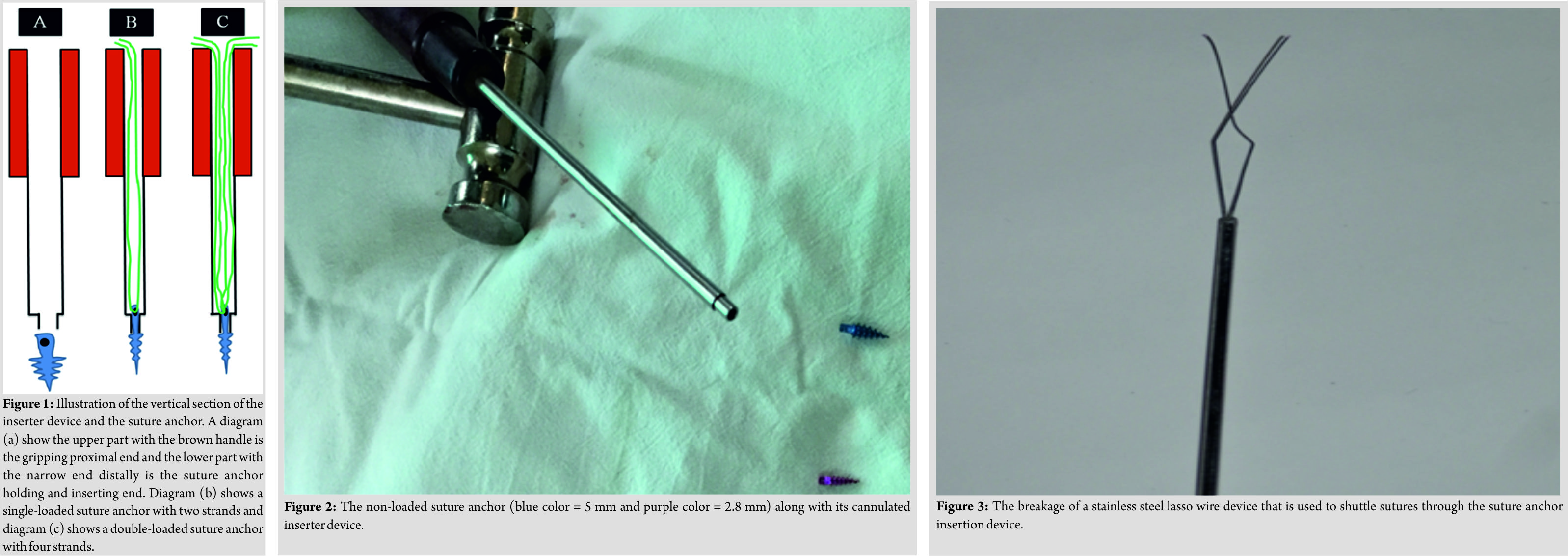 If you decide to pass two number 2 Ethibond is sequential manner then after passing one set of Ethibond sutures through the inserter device, then trying to re-insert the lasso stainless steel wire is difficult as the lasso wire does not go inside the inserter device due to crowding of space. Hence, a method was devised to overcome the challenges posed by existing devices available to pass unloaded suture anchors. This description is for the Indian made locally available 5 mm non-loaded suture anchor. First, two sutures (number 2 Ethibond) are taken, and the sutures are cut off just distal to the needles. The eyelet of the suture anchor is very minute and passing two sutures through the eyelet can be challenging. The part of the Ethibond suture just distal to the curved needle is stiff and easily negotiates the eyelet of the suture anchor (Fig. 4). Cutting the Ethibond suture just distal to the needle and passing that cut stiff end through the eyelet of the suture anchor is easier. Both the Ethibond sutures are passed through the eyelet of the 5 mm suture anchor (twin loaded) and this leaves us with four strands. Another tip for easy passage of the sutures through the eyelet is that after passing one suture, the assistant holds both the strands toward the lower part of the eyelet and the surgeon can pass the second suture through the upper part of the eyelet of the anchor (Fig. 4). Then, a number 1 Ethilon is taken, and the needle is cut off, and a loop of Ethilon is made. The Ethilon suture has wavy appearance due to the packing in the suture pack. Once the needle is cut from the Ethilon loop, then the surgeon can put one finger inside the loop and stretch the other free ends to remove the slack in the Ethilon, and this makes it easier to negotiate through the suture inserter device. In our experience, Ethilon number 1 is the most appropriate suture material to “lasso” the Ethibond sutures because it is sturdy and does not break inside the shaft of the introducer device while pulling both the Ethibond sutures simultaneously. Using Ethilon with smaller diameter leads to breakage of the suture material inside the shaft of the introducer device due to crowding of Ethibond sutures. The tips of both ends of Ethilon are introduced into the distal end of the suture anchor introducer device (Fig. 5), and the ends are passed through the tubular device till the ends emerge from the proximal end (Fig. 6). The loop of Ethilon is still kept outside the distal end. Now, all four strands of Ethibond are fed into the Ethilon loop (Fig. 7) and this loop is drawn into the tubular device taking the four strands of Ethibond along with it (Fig. 8). The Ethilon loop is drawn out of the proximal end of the introducer device along with the four strands of Ethibond (Fig. 9).
If you decide to pass two number 2 Ethibond is sequential manner then after passing one set of Ethibond sutures through the inserter device, then trying to re-insert the lasso stainless steel wire is difficult as the lasso wire does not go inside the inserter device due to crowding of space. Hence, a method was devised to overcome the challenges posed by existing devices available to pass unloaded suture anchors. This description is for the Indian made locally available 5 mm non-loaded suture anchor. First, two sutures (number 2 Ethibond) are taken, and the sutures are cut off just distal to the needles. The eyelet of the suture anchor is very minute and passing two sutures through the eyelet can be challenging. The part of the Ethibond suture just distal to the curved needle is stiff and easily negotiates the eyelet of the suture anchor (Fig. 4). Cutting the Ethibond suture just distal to the needle and passing that cut stiff end through the eyelet of the suture anchor is easier. Both the Ethibond sutures are passed through the eyelet of the 5 mm suture anchor (twin loaded) and this leaves us with four strands. Another tip for easy passage of the sutures through the eyelet is that after passing one suture, the assistant holds both the strands toward the lower part of the eyelet and the surgeon can pass the second suture through the upper part of the eyelet of the anchor (Fig. 4). Then, a number 1 Ethilon is taken, and the needle is cut off, and a loop of Ethilon is made. The Ethilon suture has wavy appearance due to the packing in the suture pack. Once the needle is cut from the Ethilon loop, then the surgeon can put one finger inside the loop and stretch the other free ends to remove the slack in the Ethilon, and this makes it easier to negotiate through the suture inserter device. In our experience, Ethilon number 1 is the most appropriate suture material to “lasso” the Ethibond sutures because it is sturdy and does not break inside the shaft of the introducer device while pulling both the Ethibond sutures simultaneously. Using Ethilon with smaller diameter leads to breakage of the suture material inside the shaft of the introducer device due to crowding of Ethibond sutures. The tips of both ends of Ethilon are introduced into the distal end of the suture anchor introducer device (Fig. 5), and the ends are passed through the tubular device till the ends emerge from the proximal end (Fig. 6). The loop of Ethilon is still kept outside the distal end. Now, all four strands of Ethibond are fed into the Ethilon loop (Fig. 7) and this loop is drawn into the tubular device taking the four strands of Ethibond along with it (Fig. 8). The Ethilon loop is drawn out of the proximal end of the introducer device along with the four strands of Ethibond (Fig. 9). 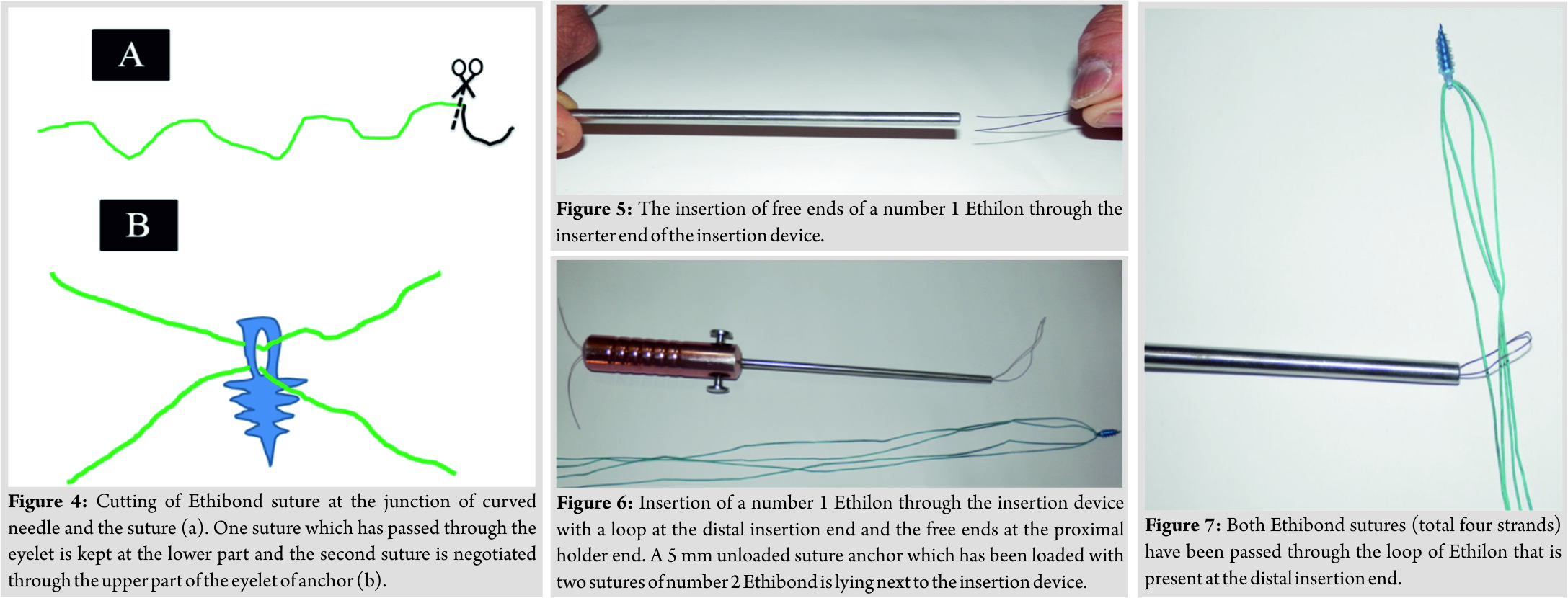 The four strands of Ethibond are pulled from the proximal end, and the eyelet of the suture anchor is loaded onto the distal end of the introducer device. The four strands of Ethibond are fastened around the proximal end of the introducer device (Fig. 10). The suture anchor is then inserted in the bone after making a pilot hole in the cortex using 2 mm Kirschner wire. The stability of fixation of the suture anchor is tested by applying moderate traction on the sutures [11]. If the suture anchor has good bony purchase, then the suture anchor would not migrate proximally on applying traction on the trailing suture ends. If the suture anchor migrates and pulls out of the bone on applying traction, then it suggests poor purchase. This can particularly be encountered in elderly patients with an osteoporotic bone having rotator cuff repair. The Ethibond suture ends from the suture anchor were fed into the eyelet of free curved needles and sutured to the tendon either in Mason-Allen, modified Kessler, or Krackow technique depending on the location of the tear and quality of the tendon to be sutured.
The four strands of Ethibond are pulled from the proximal end, and the eyelet of the suture anchor is loaded onto the distal end of the introducer device. The four strands of Ethibond are fastened around the proximal end of the introducer device (Fig. 10). The suture anchor is then inserted in the bone after making a pilot hole in the cortex using 2 mm Kirschner wire. The stability of fixation of the suture anchor is tested by applying moderate traction on the sutures [11]. If the suture anchor has good bony purchase, then the suture anchor would not migrate proximally on applying traction on the trailing suture ends. If the suture anchor migrates and pulls out of the bone on applying traction, then it suggests poor purchase. This can particularly be encountered in elderly patients with an osteoporotic bone having rotator cuff repair. The Ethibond suture ends from the suture anchor were fed into the eyelet of free curved needles and sutured to the tendon either in Mason-Allen, modified Kessler, or Krackow technique depending on the location of the tear and quality of the tendon to be sutured.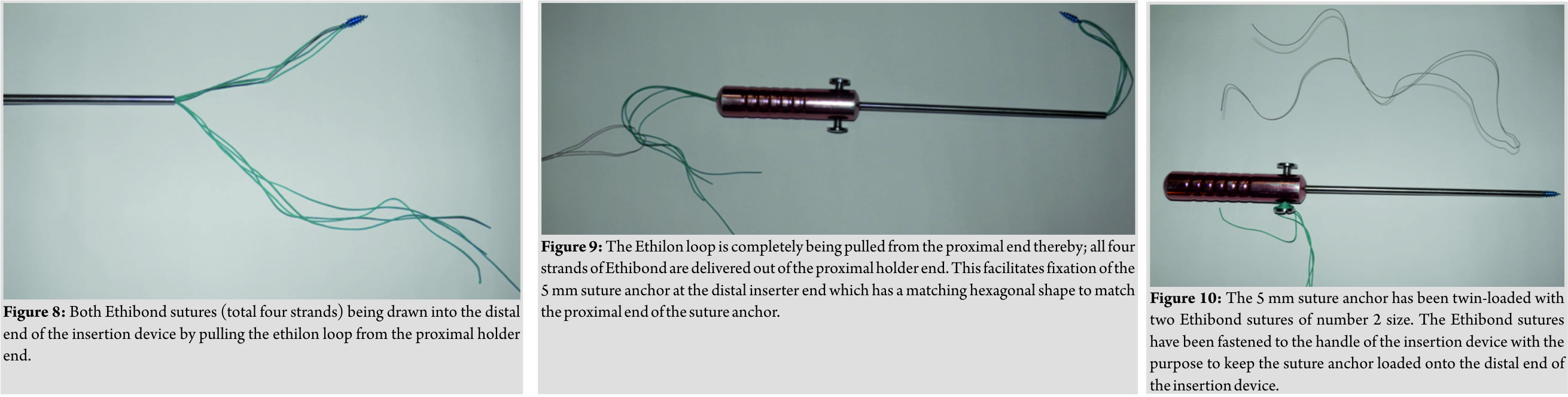
Discussion
We have used this technique in cases such as rotator cuff repair, subscapularis repair, biceps tenodesis, symptomatic partial rotator cuff tear, avulsion injuries of the insertion of tendo Achilles, debridement, and reattachment of tendo Achilles insertion in insertional tendinopathy and avulsion of medial collateral ligament of the knee from the femoral side. Good outcome was observed in all cases with no instance of failure of suture anchor, breakage of suture, migration of suture anchor or need for revision surgery due to the failure of repair. 2.8 mm and 5 mm suture anchors available from local orthopedic implant distributor costs INR 1500. The cost of two number No 2 Ethibond is approximately INR 308 and that of a single number 1–0 Ethilon is approximately INR 142. Hence, the total cost of a double-loaded suture anchor using our technique would be approximately INR 1950. Cost of preloaded suture anchor ranges from INR 6500 to INR 10,500 depending on the manufacturer. The double loading of unloaded suture anchor technique is a quick procedure and usually takes than 1–2 min depending on experience. This technique can be easily taught to scrub nurses, surgical assistants, and resident doctors assisting the case. The technique is simple with no additional need for any sophisticated instruments and can be accomplished with basic materials available in the operating theatre. The biggest advantage is that if multiple suture anchors have to be inserted, then the same Ethilon loop used to facilitate loading of one suture anchor can be re-used to load other suture anchors for the same patient. Thereby this technique drastically reduces the cost in cases such as large rotator cuff tears involving the supraspinatus, infraspinatus, and the subscapularis where multiple suture anchors need to be inserted. This technique has not been previously described as most suture anchors come preloaded with sutures especially in the western countries. However, in India and other countries where affordability plays a limiting factor, creating double-loaded suture anchor with easily available and cheap material helps to provide affordably and quality care to our patients. For 2.8 mm unloaded suture anchor, it is possible to convert into a single-loaded suture anchor because the diameter of the eyelet of 2.8 mm unloaded suture anchor is so small that it would not accommodate two number 2 Ethibond sutures. The limitation of the present study is that the results of this technique have not been compared to commercially available preloaded suture anchors. In the future, we plan to undertake studies to compare our technique with preloaded suture anchors to evaluate the stability of fixation and clinical outcome.
Conclusion
This is a novel, time saving, simple, cheap, and easily reproducible method to create an effective double-loaded suture anchor from a non-loaded suture anchor.
Clinical Message
The technique described can be easily replicated by specialists and general orthopedic surgeons working in resource limited settings
References
1. Denard PJ, Burkhart SS. The evolution of suture anchors in arthroscopic rotator cuff repair. Arthroscopy 2013;29:1589-95.
2. Chen JS, Novikov D, Kaplan DJ, Meislin RJ. Effect of additional sutures per suture anchor in arthroscopic bankart repair: A review of single-loaded versus double-loaded suture anchors. Arthroscopy 2016;32:1415-20.
3. Kamath GV, Hoover S, Creighton RA, Weinhold P, Barrow A, Spang JT, et al. Biomechanical analysis of a double-loaded glenoid anchor configuration: Can fewer anchors provide equivalent fixation? Am J Sports Med 2013;41:163-8.
4. Longo UG, Buchmann S, Berton A, Maffulli N, Denaro V. Arthroscopic knots and strength sutures for rotator cuff repair. Sports Med Arthrosc Rev 2011;19:251-65.
5. Castagna A, Garofalo R, Conti M, Flanagin B. Arthroscopic bankart repair: Have we finally reached a gold standard? Knee Surg Sports Traumatol Arthrosc 2016;24:398-405.
6. Kibler WB, Sciascia A. Current practice for the surgical treatment of SLAP lesions: A systematic review. Arthroscopy 2016;32:669-83.
7. Kodde IF, Baerveldt RC, Mulder PG, Eygendaal D, van den Bekerom MP. Refixation techniques and approaches for distal biceps tendon ruptures: A systematic review of clinical studies. J Shoulder Elbow Surg 2016;25:e29-37.
8. Kiliçoğlu O, Türker M, Yildız F, Akalan E, Temelli Y. Suture anchor tenodesis in repair of distal achilles tendon injuries. Eur J Orthop Surg Traumatol 2014;24:117-22.
9. Hu CY, Lee KB, Song EK, Kim MS, Park KS. Comparison of bone tunnel and suture anchor techniques in the modified broström procedure for chronic lateral ankle instability. Am J Sports Med 2013;41:1877-84.
10. Saper MG, Meijer K, Winnier S, Popovich J Jr., Andrews JR, Roth C, et al. Biomechanical evaluation of classic solid and all-soft suture anchors for medial patellofemoral ligament reconstruction. Am J Sports Med 2017;45:1622-6.
11. Brady PC, Arrigoni P, Burkhart SS. What do you do when you have a loose screw? Arthroscopy 2006;22:925-30.
 |
| Dr. Karthik Vishwanathan |
| How to Cite This Article: Vishwanathan K. Simple, Cost-Effective Technique to Create a Double-Loaded Suture Anchor from a Non-loaded Suture Anchor. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 80-83. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Letter to the Editor: Spina Ventosa Involving Bilateral Proximal Phalanx in a 6-year-old Girl: A Multifocal Tuberculosis
February 1, 2026 Letter to the Editor: Spina Ventosa Involving Bilateral Proximal Phalanx in a 6-year-old Girl: A Multifocal Tuberculosis April 7, 2014 Malakoplakia of Proximal Tibia- A Case Report
April 7, 2014 Malakoplakia of Proximal Tibia- A Case Report February 1, 2026 Symptomatic Intratendinous Ganglion Cyst of the Patellar Tendon: Case Report and Review of the Literature
February 1, 2026 Symptomatic Intratendinous Ganglion Cyst of the Patellar Tendon: Case Report and Review of the Literature December 10, 2022 A Hidden “Suspender” in Irreducible Isolated Anteromedial Radial Head Dislocations – A Case Report and Review
December 10, 2022 A Hidden “Suspender” in Irreducible Isolated Anteromedial Radial Head Dislocations – A Case Report and Review