
A thorough pre-operative MRI evaluation and high index of suspicion with single-stage reconstruction of this rare injury triad gives excellent outcome.
Dr. Ishan Shevate,
Dr. DY Patil Medical College and Hospital, Pune, Maharashtra, India.
E-mail: ishanshevate@gmail.com
Abstract
Introduction: The medial collateral ligament (MCL) is the most commonly injured ligament of the knee joint; however, its displacement into the medial knee compartment is rare. Traumatic posterior root of medial meniscus (PRMM) tears are commonly found in high-grade injuries involving anterior cruciate ligament (ACL) or posterior cruciate ligament (PCL) tears along with MCL tears. Diagnosis of these injuries can be made by a preoperative magnetic resonance imaging (MRI), but they can be missed at times due to severe soft-tissue swelling in the acute phase.
Case Report: A 25-year-old gentleman presented with injury to the front of his left knee 5 days back. On examination, he had a Grade 3 effusion with valgus stress test and posterior drawer test being positive and medial joint line tenderness was present. A firm localized swelling was palpable on the medial joint line. MRI scan revealed a mid-substance PCL tear, ACL sprain, PRMM tear, and tibial side rupture of superficial MCL with proximally migrated wavy MCL fibers lying below the medial meniscus confirmed on arthroscopy. Medial meniscus root repair by pull through technique and PCL reconstruction with a 3-strand peroneus longus graft followed by open MCL repair with augmentation using a semitendinosus graft was performed. Postoperatively, the knee was kept in a straight knee brace for 4 weeks, followed by a hinged knee brace and appropriate physiotherapy were started. At 2 years follow-up, the patient had attained full range of knee motion with good quadriceps strength, tibial step off maintained, and negative posterior drawer test and valgus stress test. Displacement of torn MCL into the medial knee compartment is an extremely rare injury. Proximal or distal avulsion of MCL with intra-articular incarceration has been reported in isolation or associated with ACL tear. Such an injury triad as reported here has not been reported in the literature to the best of our review.
Conclusion: In our case, we report a very unusual injury triad of PCL tear, PRMM tear, and distal MCL tear with intra-articular entrapment below the medial meniscus operated by a single-stage surgery with excellent outcomes.
Keywords: Medial collateral ligament tear, intra-articular entrapment, posterior root medial meniscus tear, posterior cruciate ligament tear, unusual triad.
The medial collateral ligament (MCL) is the most commonly injured ligament of the knee joint. Displacement of torn MCL into the medial knee compartment is an extremely rare injury. Proximal or distal avulsion of MCL with intra-articular incarceration has been reported in isolation or associated with anterior cruciate ligament (ACL) tear [1,2,3,4]. Concomitant posterior cruciate ligament (PCL) tear with MCL or posteromedial corner (PMC) injuries are known but rarely occurring injuries [5]. PRMM tears are often degenerative and commonly seen in middle-aged females [6,7]. Traumatic PRMM tears are commonly found in high-grade injuries involving ACL or PCL tears along with MCL tears. These are rare injuries, hence require high index of suspicion for timely diagnosis and treatment [8,9,10]. An incidence rate of around 2.74% of acute medial meniscus posterior root tears was found to be associated with multiligament injuries [8]. Complete tear of MCL and PMC with cruciate rupture is categorized into severe medial instability of knee [10]. These injuries usually occur following a high-energy trauma. Diagnosis of these unusual injuries is made by a pre-operative magnetic resonance imaging (MRI), but they can be missed at times due to severe soft-tissue swelling on medial side giving a diffuse hyperintensity in posteromedial joint area in the acute phase [11]. We report a case of a 25-year-old gentleman with an undescribed injury triad involving complete PCL tear, posterior root medial meniscus (PRMM) tear, and tibial rupture of MCL with intra-articular incarceration and its management.
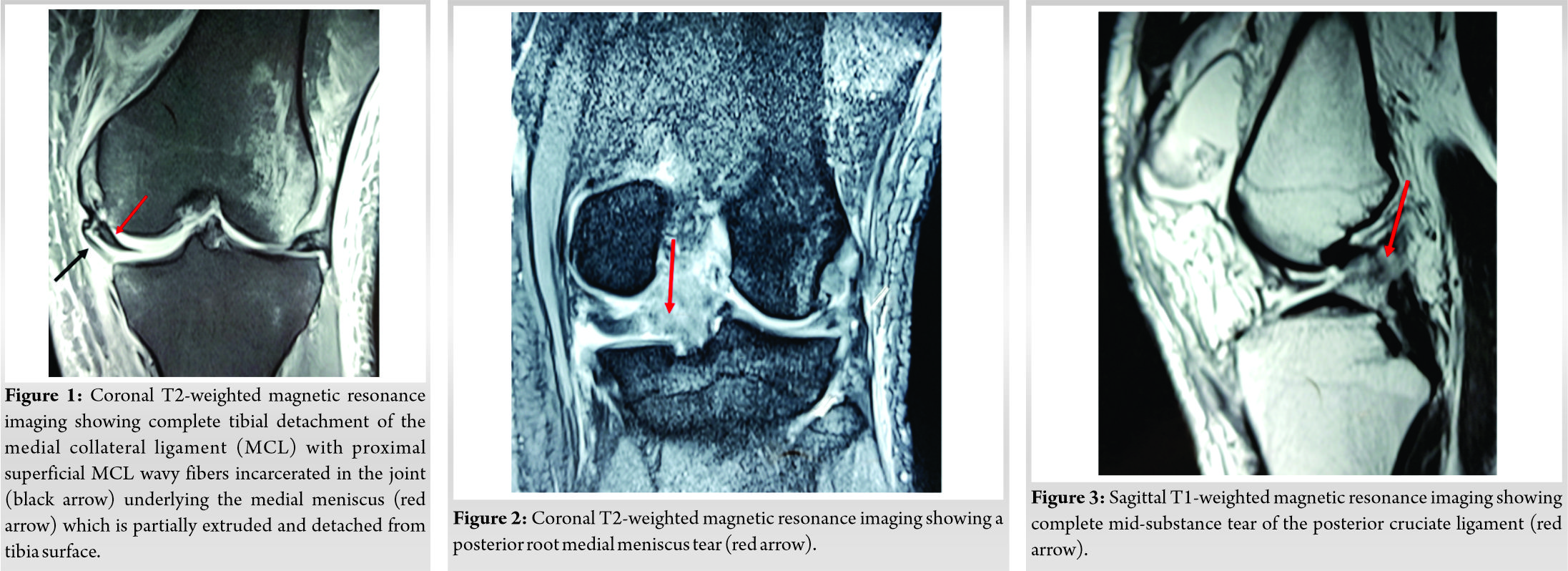
A 25-year-old gentleman presented to the emergency department with a history of bumper injury to the front of his left knee 5 days back. He did not give any history of knee dislocation. He recalled knee angulating backwards with a posterior jerk followed by buckling of the knee before he lost his balance. He was unable to bear weight and walk on his left leg. On local examination, he had a Grade 3 effusion with positive patellar tap. The valgus stress test was Grade 3 and had a Grade 3 posterior drawer test with considerable pain. The sag sign was positive with loss of tibial step off. Joint line tenderness was present on medial and posterior aspect. A firm localized swelling was palpable on the medial joint line in the region of superficial MCL (sMCL). Plain radiographs showed increased patellofemoral space due to effusion and posterior translation of the tibia. MRI scan revealed a complete mid-substance PCL tear, ACL sprain, PRMM tear, and tibial side rupture of sMCL with proximally migrated wavy MCL fibers lying below the medial meniscus displaced into the medial compartment of the joint (Fig. 1, 2, 3).
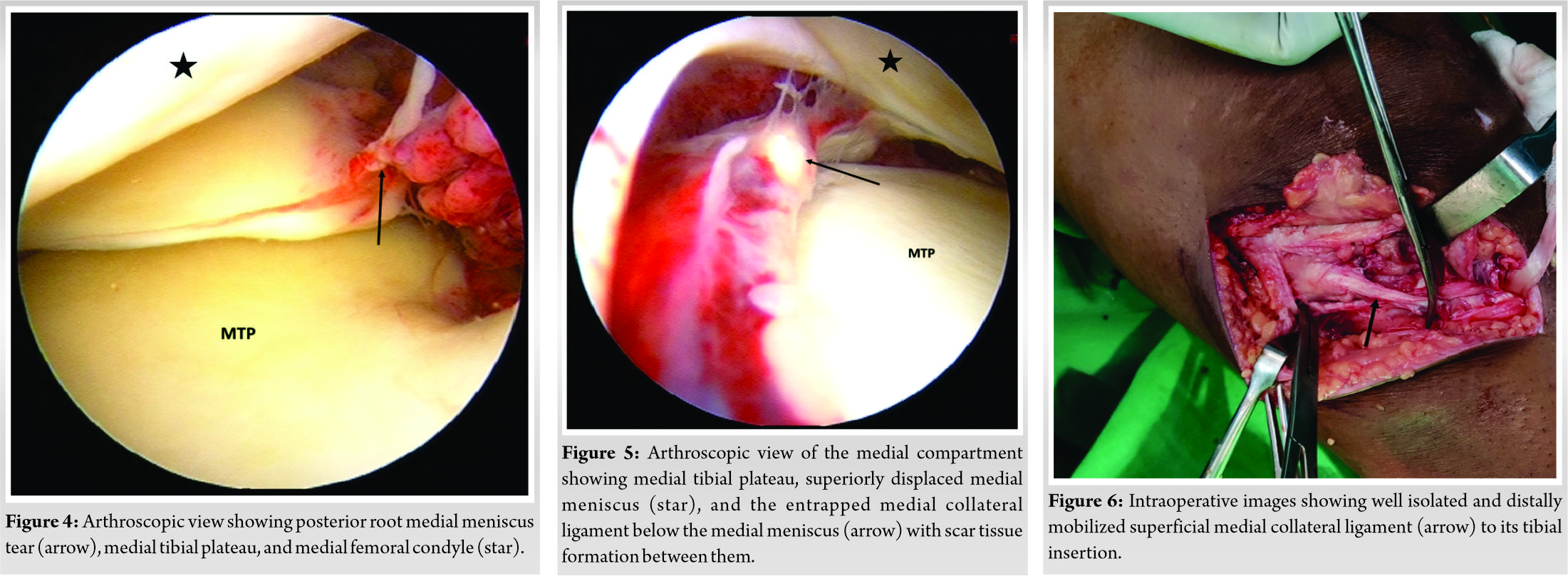
A structured pre-habilitation was started for muscle strengthening, reeducation, and range of motion. Surgery was planned 3 weeks post-injury after the acute signs subsided and knee flexion was around 100°. The patient was explained the need of surgery and informed consent was taken. Diagnostic round of arthroscopy confirmed complete tear of PCL with positive floppy ACL sign. It revealed a PRMM tear (Fig. 4). Medial drive through sign was positive. Moreover, as the MRI scan revealed, the distal fibers of sMCL were seen incarcerated into the medial compartment passing between the body of medial meniscus and the tibial plateau (Fig. 5).
We decided to go ahead with medial meniscus root repair and PCL reconstruction using separate anatomic tibial tunnels followed by open MCL repair with augmentation. Medial meniscus root repair was performed by passing one no. 2 fiber wire and one fiber tape by pull through technique using ACL drill guide set at 45°. The root was not fixed at this point. The peroneus longus graft was harvested from the same leg. PCL tibial tunnel was drilled with the drill guide at 60° entering more anteromedially as compared to the root repair tunnel to avoid convergence. A 3-strand graft was passed and fixed using adjustable loop and bioabsorbable screw. The early scar tissue formed between the MCL stump and undersurface of medial meniscus was freed arthroscopically. Using a medial approach, the MCL was freed from the undersurface of medial meniscus and the capsule (Fig. 6).
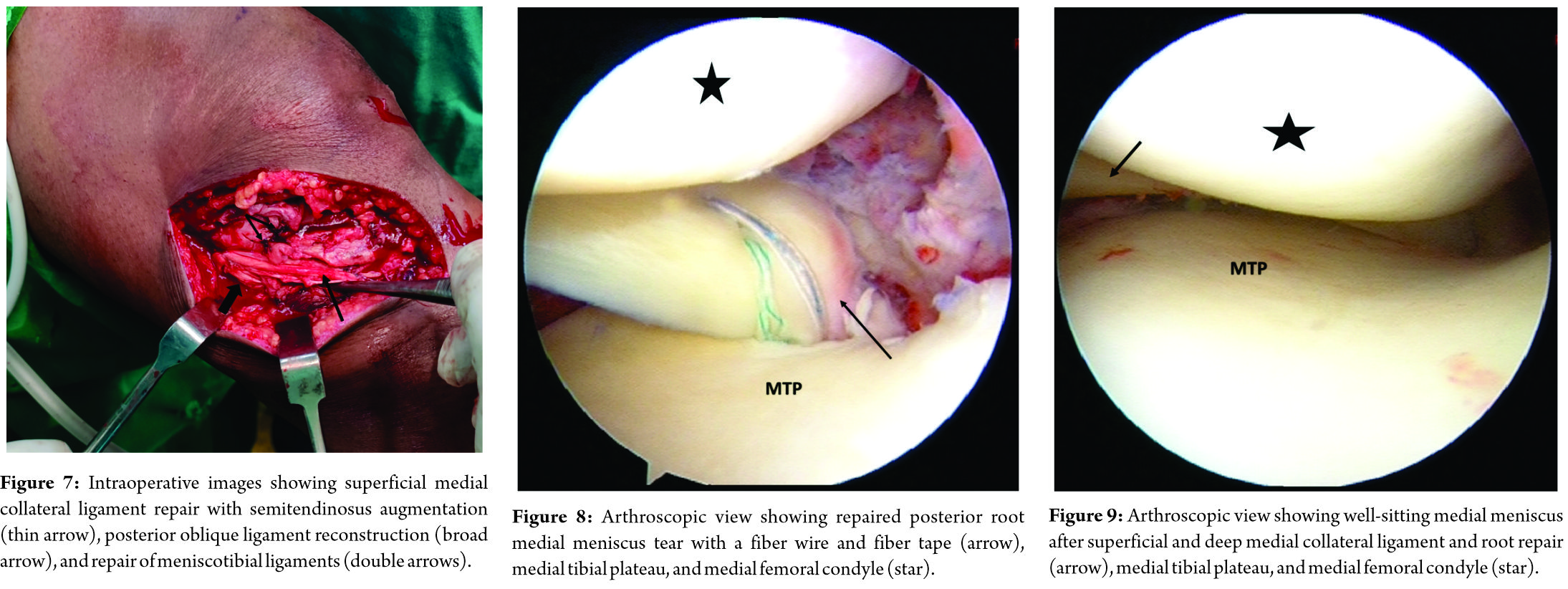
The deep MCL was repaired primarily to its tibial attachment with 2-0 Ethibond. The sMCL was advanced back to its tibial attachment site and repaired with titanium 3.0 mm suture anchor. Considering the time from injury and the amount of MCL stump that was left behind to suture back, it was decided to augment the sMCL. Using Stannard’s modification of Kim’s technique, sMCL was augmented with semitendinosus graft and fixed over the femoral attachment with 5.0 titanium suture anchor [12,13] (Fig. 7). Finally, the medial meniscus root was fixed over a titanium suture disc after checking the reduction and tension (Fig. 8). The medial meniscus was found to be sitting well over the tibial condyle post repairs (Fig. 9). Postoperatively, the knee was placed in a straight knee brace for 4 weeks followed by a hinged knee brace. He was kept non-weight-bearing with crutch support for 4 weeks. Range of motion exercises were started gradually from 0 to 90° over the period of 4 weeks. Static quadriceps, gluteus exercises, and straight leg raises along with calf pumps were started immediately according to the pain tolerance. After 4 weeks, partial weight-bearing was begun gradually progressing to full weight-bearing without support by 8–10 weeks. At 1-year follow-up, the patient had attained full range of knee motion with good quadriceps strength. There was no joint line tenderness. Tibial step off was maintained with negative posterior drawer test and valgus stress test. He had returned to pre-injury sporting and routine activities without symptoms.
In our reported case, the most characteristic injury was the tibial rupture of MCL and medial capsular tear with entrapment of the stump between the medial meniscus and tibial plateau, concomitant with complete mid-substance PCL tear and PRMM tear. Such an injury triad has not been reported in the literature to the best of our review. Pre-operative diagnosis of such injuries on MRI is very important to avoid disastrous consequences.
There have been reports previously described of intra-articular incarceration of the ruptured MCL either from femoral or tibial side [1,2,3,4]. In the report by Desai et al., the tibial stump of MCL was interposed between the medial meniscus and medial tibial plateau in a 9-year-old boy [1]. Walton et al. reported a case of proximal rupture of MCL with intercondylar notch incarceration [2]. The case reported by Kini et al., had torn distal MCL entrapped in the joint in combination with ACL tear [3]. Patel et al. reported a case with proximal and distal avulsion of MCL with displacement into the medial joint. This was associated with torn and displaced medial patellar retinaculum into medial patellofemoral joint, PCL tear, ACL tear, and posterior horn medial meniscus tear [4]. Kennedy in his classic biomechanical study of knee dislocation described the mechanism of such injuries. With hyperextension of the knee, the posterior capsule tears first, followed by the cruciate. A valgus force along with axial rotation of the knee then ruptures the superficial and deep MCL. The forces subsequently pass posteriorly through the relatively mobile post-horn of medial meniscus to the non-mobile root. The root then gets avulsed from the tibial insertion site [14]. In their study by Ritchie et al., they showed that in Grade 3, tears of MCL in combination with PCL tear led to increased laxity in internal rotation of tibia and significantly increased posterior tibial translation. Hence, the restoration of MCL in concomitant PCL-MCL injuries is recommended to restore normal biomechanics [15]. This principle was followed in our case as well. Kim et al. in their case series of 10 knees with medial meniscus posterior root tear associated with ligament injuries, reported one case with PCL, MCL, and coronary ligament tear associated with PRMM tear. It was managed operatively in single sitting with good functional results [8]. The limitation of our study being a case report is a detailed study of a greater number of cases is required to see for other associated injuries, different treatment options, and the complications associated.
In our case, we report a very unusual injury triad of PCL tear, PRMM tear, and distal MCL tear with intra-articular entrapment below the medial meniscus. A pre-operative MRI scan detected all these injuries. A single-stage treatment of all the injuries can be performed with excellent outcomes.
An unusual knee injury triad has been described here with, MCL tibial rupture with intra-articular entrapment, a PRMM tear, and complete intrasubstance tear of PCL. Pre-operative MRI evaluation could pick up all these injuries and helped in planning the surgery. A single-stage repair of posterior root, repair with augmentation of MCL and PCL reconstruction after an adequate prehab gives good results.
References
- 1.Desai R, Parikh S, Laor T. Intra-articular entrapment of the medial collateral ligament. Orthopedics 2010;33:687. [Google Scholar | PubMed]
- 2.Walton E, Williams M, Robinson J R. Incarceration of the medial collateral ligament in the intercondylar notch following proximal avulsion. Skeletal Radiol 2017;46:1575-8. [Google Scholar | PubMed]
- 3.Kini SG, du Pre K, Bruce W. Posttraumatic incarceration of medial collateral ligament into knee joint with anterior cruciate ligament injury. Chin J Traumatol 2015;18:367-369. [Google Scholar | PubMed]
- 4.Patel JJ. Intra-articular entrapment of the medial collateral ligament: Radiographic and MRI findings. Skeletal Radiol 1999;28:658-60. [Google Scholar | PubMed]
- 5.Forsythe B, Mascarenhas R, Pombo MW, Harner CD. Combined injuries to the posterior cruciate ligament and medial collateral ligament of the knee. Knee Joint 2012;36:421-6. [Google Scholar | PubMed]
- 6.Kim SB, Ha JK, Lee SW, Kim DW, Shim JC, Kim JG, et al. Medial meniscus root tear refixation: Comparison of clinical, radiologic, and arthroscopic findings with medial meniscectomy. Arthroscopy 2011a;27:346-54. [Google Scholar | PubMed]
- 7.Hwang BY, Kim SJ, Lee SW, Lee HE, Lee CK, Hunter DJ, et al. Risk factors for medial meniscus posterior root tear. Am J Sports Med 2012;40:1606-10. [Google Scholar | PubMed]
- 8.Kim YJ, Kim JG, Chang SH, Shim JC, Kim SB, Lee MY. Posterior root tear of the medial meniscus in multiple knee ligament injuries. Knee 2010;17:324-8. [Google Scholar | PubMed]
- 9.Ra HJ, Ha JK, Jang HS, Kim JG. Traumatic posterior root tear of the medial meniscus in patients with severe medial instability of the knee. Knee Surg Sports Traumatol Arthrosc 2015;23:3121-6. [Google Scholar | PubMed]
- 10.Ozkoc G, Circi E, Gonc U, Irgit K, Pourbagher A, Tandogan RN. Radial tears in the root of the posterior horn of the medial meniscus. Knee Surg Sports Traumatol Arthrosc 2008;16:849-54. [Google Scholar | PubMed]
- 11.Lee YG, Shim JC, Choi YS, Kim JG, Lee GJ, Kim HK. Magnetic resonance imaging findings of surgically proven medial meniscus root tear: Tear configuration and associated knee abnormalities. J Comput Assist Tomogr 2008;32:452-7. [Google Scholar | PubMed]
- 12.Kim SJ, Lee DH, Kim TE, Choi NH. Concomitant reconstruction of the medial collateral and posterior oblique ligaments for medial instability of the knee. J Bone Joint Surg Br 2008;90:1323-7. [Google Scholar | PubMed]
- 13.Stannard JP. Medial and posteromedial instability of the knee: Evaluation, treatment, and results. Sports Med Arthrosc 2010;18:263-8. [Google Scholar | PubMed]
- 14.Kennedy JC. Complete dislocation of the knee joint. J Bone Joint Surg Am 1963;45:889-904. [Google Scholar | PubMed]
- 15.Ritchie JR, Bergfeld JA, Kambic H, Manning T. Isolated sectioning of the medial and posteromedial capsular ligaments in the posterior cruciate ligament-defificient knee. Influence on posterior tibial translation. Am J Sports Med 1988;26:389-94. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Severe Metallosis after Tumor Mega-Prosthesis: Revise or Retain? – A Case Series
July 1, 2026 Severe Metallosis after Tumor Mega-Prosthesis: Revise or Retain? – A Case Series July 11, 2014 Complete Traumatic Separation of Proximal Femoral Epiphysis in A 2 Year Old Child
July 11, 2014 Complete Traumatic Separation of Proximal Femoral Epiphysis in A 2 Year Old Child January 19, 2013 A Case Report of Synovial Chondromatosis of the Knee Joint arising from the Marginal Synovium
January 19, 2013 A Case Report of Synovial Chondromatosis of the Knee Joint arising from the Marginal Synovium May 9, 2017 Early Motor Delay: An Outstanding, Initial Sign of Osteogenesis Imperfecta Type 1
May 9, 2017 Early Motor Delay: An Outstanding, Initial Sign of Osteogenesis Imperfecta Type 1