
Intra-articular lipomas are very rare and painless, but if they interfere with our daily activities, the removal should be considered..
Dr. Naoki Ishida,
Department of Orthopedic Surgery, Hokuto Medical Corporation Hokuto Hospital, 7-5 Kisen, Inada, Obihiro, Hokkaido, Japan. E-mail: ishida@hokuto7.or.jp
Abstract
Introduction: Lipomas are the most common type of soft-tissue tumor, but intra-articular lipomas are very rare. Most cases occur in the knee joint. This is a report of intra-articular lipoma in the knee joint, 8 months after removal with good post-operative outcome.
Case Report: A 56-year-old female who presented soft-tissue mass on her right knee. She felt uncomfortable but not in pain. The mass grew gradually and she wanted to be surgically removed. The mass was too large (5 cm × 4 cm × 2 cm) to be removed endoscopically, so arthrotomy was made. The mass was true lipoma histologically. She is living happily without recurrence after surgery.
Conclusion: We have described an intra-articular synovial lipoma in the knee of a middle-aged female. Intra-articular lipomas are very rare. The tumor in this case was relatively large but painless, and the chief complaint was discomfort. It grew gradually, so the removal was performed. At present, the patient is living happy without recurrence after surgery.
Keywords: Intra-articular lipoma, knee, removal, arthroscopy.
Lipoma is a frequent benign tumor of the soft tissue [1]. There are two types of lipomas, true lipoma and lipoma arborescens. Basically, intra-articular true lipoma is so rare, with only dozens of cases reported in the literature up to now [2,3,4,5,6,7,8,9,10]. Clinically, most of the patients with intra-articular lipoma are asymptomatic, some show as pressure symptoms caused by mass lesions, such as locking, kneeling pain, and so on. Magnetic resonance imaging (MRI) is an essential modality to suggest the diagnosis preoperatively [2,3,4,5]. The curative treatment of intra-articular lipoma is removal. If possible, arthroscopic removal is minimally invasive and is desirable. Here, we present the clinical case of a female patient with an intra-articular lipoma in her knee.
Written informed consent was obtained from the patient to publish this case report and any accompanying images.
A 56-year-old female was referred to our hospital from another orthopedic clinic with a soft-tissue mass on her right knee without cause. She had no particular medical history, family history, or trauma history. She noticed the mass 8 months earlier. The mass gradually grew in size and deep flexion became uncomfortable. She felt no pain and had no limitation of activities. She felt that something like a mass went in and out as the knee moved in her right knee.
On examination, the right knee was found to be swollen, especially at lateral recess. The mass was soft, non-tender, no localized temperature increase, and no joint effusion. Moreover, it was highly mobile and had no adhesions to its surroundings. The range of knee motion was 0–140, although it hurt a little at maximum flexion. There was no evidence of muscular atrophy or instability of the knee joint.
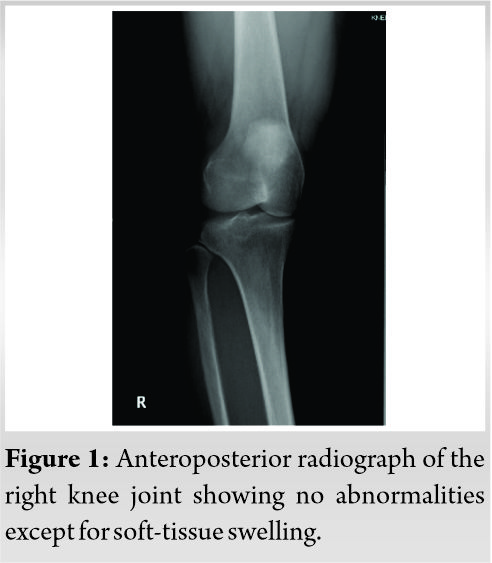
The results of blood tests were essentially normal. X-ray findings of the right knee joint showed no abnormalities. No osteoarthritic change or bone erosion was present. A soft-tissue shadow was not seen (Fig. 1).
MRI showed an oval-shaped mass of low to high heterogeneous signal intensity on T1- and T2-weighted images at the lateral joint space. Low signal intensity was observed in the fat suppression image (Fig. 2). Therefore, a tumor derived from adipose tissue with fibrous component is suspected.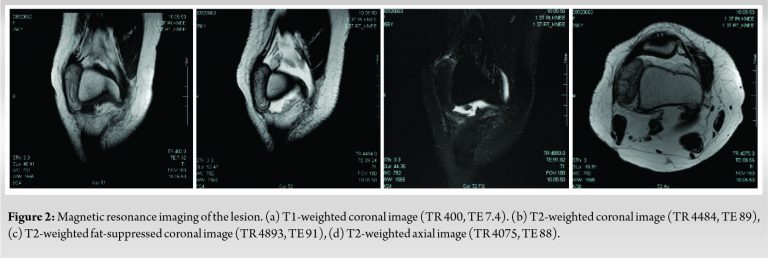
The mass was 5 cm × 4 cm × 2 cm in size. No contrast agent used.
As a differential diagnosis of adipose-derived soft-tissue tumor, true lipoma, lipoma arborescens, and liposarcoma can be considered. The patient subsequently underwent an operative arthroscopy.
First, the inside of the knee joint was carefully checked with an arthroscope. Mild degeneration of the lateral meniscus was observed. No other abnormalities such as synovial proliferation and cartilage lesion were seen. A large mass was found in the lateral recess.
It was soft, mobile and had no adhesion to its surroundings. It was too large to be removed endoscopically.
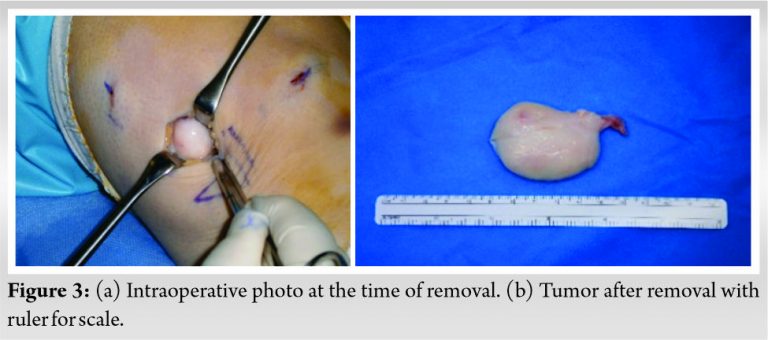
An arthrotomy was made by a lateral parapatellar incision of about 4 cm. An ovoid soft-tissue mass wrapped in a white capsule appeared. The mass was not adhesive to its surroundings and was mobile. The mass had a stalk that was connected to the anterolateral joint capsule near the lateral fat pad.
On excision of the stalk, the mass was easily removed (Fig. 3). When the mass was cut and opened, the inside looked like adipose tissue.
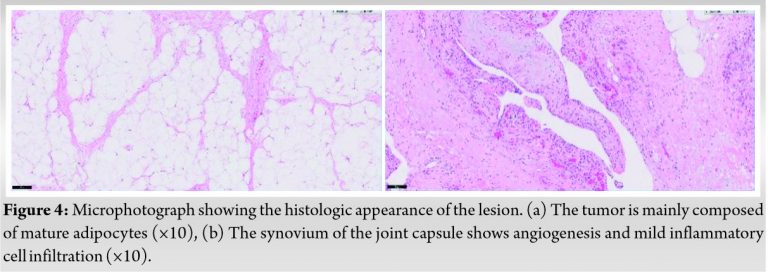
Histologically, the synovium of the joint capsule shows angiogenesis and mild inflammatory cell infiltration. There was no contradiction as a true lipoma occurred in the knee joint, and no particular malignant findings are observed (Fig. 4).
Eight months after the operation, there is no recurrence and no particular abnormality. She is doing well with no symptoms and no range of motion restrictions.
Lipomas are the most common type of soft-tissue tumor [1]. Although they may arise almost anywhere there is fatty tissue in the body, intra-articular examples are extremely rare. Only dozens of cases have been reported so far [2,3,4,5,6,7,8,9,10]. Most cases occur in the knee joint. There are two different benign types of lipoma: The true lipoma and the more common lipoma arborescens [2,3,4,5,6,7,8,9,10].
Intra-articular true lipoma is defined as a solitary round or ovoid mass of fatty tissue contained in a thin, fibrous capsule and without synovial changes. They typically arise from fat pad area or from the suprapatellar pouch.
The clinical findings of intra-articular lipoma depend on the site and size of the mass. Most of the patients may be asymptomatic and some have complaints of dull pain or discomfort due to pressure, joint swelling, motion pain, and limitation of the range of motion [2,3,4,5,6,7,8,9,10].
Twisting and strangulation of the stalk can cause sudden pain in the knee [2,3,4].
Lipomas are usually relatively small, which may lead to a locked knee, catching, and the limitation of the range of knee motion like a free body.
However, there is a report of huge case exceeding 10 cm (13 cm × 8.5 cm) surprisingly [5].
There is also a report that lipoma is located the anterior cruciate ligament and the posterior cruciate ligament and is too small to be diagnosed by MRI. Therefore, there may be potential cases of intra-articular lipoma that is not diagnosed [5,9,14].
Lipoma arborescens is caused by irritation such as previous trauma, osteoarthritis, and other chronic inflammatory disease (e.g., rheumatoid arthritis, etc.).
It is a villous lipomatous proliferation of the synovial membrane [4,5,7,9,11,12].
Hence, true lipoma and lipoma arborescens should be treated as different things.
Lipoma arborescens is characterized by a diffuse subsynovial deposit of fat and a villous appearance, associated with joint effusion and synovial cyst, and bone erosion.
Above all, joint effusion is typically seen with lipoma arborescens.
It is important to consider liposarcoma as well [1,13].
Liposarcoma accounts for about 20% of malignant soft-tissue tumors. Most liposarcoma is asymptomatic and is often 5 cm or larger when noticed. Moreover, it occurs in the deep part, is hard, adheres to surrounding tissues, and has poor mobility.
Our patient had no history of preceding trauma or joint disorders.
The patient was a middle-aged woman with no symptoms such as pain, joint effusion, and limited range of motion. The tumor is soft and has no adhesion to the surroundings, and is relatively large at 5 cm, but the possibility of malignancy is very low. From these clinical findings, true lipoma is most likely.
The laboratory findings are generally unremarkable. Joint fluid typically is negative for crystals, and cultures of the fluid are negative as well [2,3,4,5,7]. X-rays show no specific findings, only soft-tissue shadows in the region of the suprapatellar pouch and joint space [2,3,4,5,7,8]. They often show osteoarthritic changes.
MRI is an indispensable test for diagnosis of the intra-articular lesions such as synovial lipoma and lipoma arborescens (villous lipomatous proliferation of the synovial membrane). Typically, images of intra-articular synovial lipoma appears the high signal intensity on both T1-weighted and T2-weighted images. Moreover, low signal intensity is observed in the fat suppression images.
Removal of the lesions under arthroscopic guidance or by an open surgical method is curative for intra-articular synovial lipoma [2,3,4,5,6,7,8,9,10].
On the other hand, thorough arthroscopic synovectomy is essential treatment for lipoma arborescens [11,12].
Arthroscopic removal is clearly less invasive than open arthrotomy. Hence, arthroscopic removal is desirable if possible [2,3,4,5]. If it is too large to be removed under arthroscopy, it must be removed with a short open incision.
There have been no recurrence of the lesion following excision in the previous studies so far [3,5,14]. Post-operative results are excellent and the patients are painless and living their daily lives.
We have described an intra-articular synovial lipoma in the knee of a middle-aged female. Intra-articular lipomas are very rare. The tumor in this case was relatively large but almost asymptomatic, and the chief complaint was discomfort. At present, the patient is living happy without recurrence after surgery.
MRI is essential for the diagnosis of intra-knee lesions. If lipoma is suspected and interferes with life, removal is considered. There have been no reports of recurrence after removal, and good results have been obtained.
References
- 1.Rydholm A, Berg NO. Size, site and clinical incidence of lipoma. Factors in the differential diagnosis of lipoma and sarcoma. Acta Orthop Scand 1983;54:929-34. [Google Scholar | PubMed]
- 2.Poorteman L, Declercq H, Natens P, Wetzeis K, Vanhoenacker F. Intra-articular synovial lipoma of the knee joint. BJR Case Rep 2015;1:20150061. [Google Scholar | PubMed]
- 3.Hirano K, Deguchi M, Kanamoto T. Intra-articular synovial lipoma of the knee joint (located in the lateral recess): A case report and review of the literature. Knee 2007;14:63-7. [Google Scholar | PubMed]
- 4.Matsumoto K, Okabe H, Ishizawa M, Hiraoka S. Intra-articular lipoma of the knee joint. A case report. J Bone Joint Surg Am 2001;83:101-5. [Google Scholar | PubMed]
- 5.Jaime DR, Jose JN. Large intra-articular true lipoma of the knee. BMC Musculoskelet Disord 2019;20:110. Pudlowski RM, Gilula LA, Kyriakos M. Intraarticular lipoma with osseous metaplasia: Radiographic-pathologic correlation. AJR Am J Roentgenol 1979;132:471-3. [Google Scholar | PubMed]
- 6.Amarjit KS, Budhiraja S, Chandramouleeswari K, Anita S. Knee locking in osteoarthritis due to synovial lipoma: A case report. J Clin Diagn Res 2013;7:1708-9. [Google Scholar | PubMed]
- 7.Hill JA, Martin WR 3rd, Milgram JW. Unusual arthroscopic knee lesions: Case report of an intra-articular lipoma. J Natl Med Assoc 1993;85:697-9. [Google Scholar | PubMed]
- 8.Kheok SW, Ong KO. Benign periarticular, bone and joint lipomatous lesions. Singapore Med J 2017;58:521-7. [Google Scholar | PubMed]
- 9.Yamada S, Yonekura A, Asahara T, Miyamoto T, Shindo H. Intra-articular lipoma of the knee limiting range of motion: Case report and review of literature. Orthop Traumatol 2010;59:817-21. [Google Scholar | PubMed]
- 10.Souza TP, Carneiro JB, Reis MF, Batista BB, Gama FA, Ribeiro SL. Primary lipoma arborescens of the knee. Eur J Rheumatol 2017;4:219-21. [Google Scholar | PubMed]
- 11.Sola JB, Wright RW. Arthroscopic treatment for lipoma arborescens of the knee. J Bone Joint Surg 1998;80:99-103. [Google Scholar | PubMed]
- 12.Khan AM, Cannon S, Levack B. Primary intra-articular liposarcoma of the knee. Case report. J Knee Surg 2003;16:107-9. [Google Scholar | PubMed]
- 13.Ozalay M, Tandogan RN, Akpinar S, Cesur N, Hersekli MA, Ozkoç G, et al. Arthroscopic treatment of solitary benign intra-articular lesions of the knee that cause mechanical symptoms. Arthroscopy 2005;21:12-8. [Google Scholar | PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2023 Medial Swivel Dislocation of the Talonavicular Joint Due to High-Energy Trauma: A Case Report
March 10, 2023 Medial Swivel Dislocation of the Talonavicular Joint Due to High-Energy Trauma: A Case Report October 10, 2016 Reviewers Acknowledgement & Photo-Gallery September – October 2016
October 10, 2016 Reviewers Acknowledgement & Photo-Gallery September – October 2016 January 10, 2024 Reviewers Acknowledgement & Photo Gallery January 2024
January 10, 2024 Reviewers Acknowledgement & Photo Gallery January 2024 October 8, 2012 Pseudo-Acetabulum due to Heterotopic Ossification in a Child with Post Traumatic Neglected Posterior Hip Dislocation-Fulltext
October 8, 2012 Pseudo-Acetabulum due to Heterotopic Ossification in a Child with Post Traumatic Neglected Posterior Hip Dislocation-Fulltext