
Isolated Lesser Tuberosity fractures of Humerus are rare and can be missed easily, identifying and fixing these fractures early can lead to excellent clinical outcomes.
Dr. Amyn M. Rajani, Orthopaedic Arthroscopic Knee and Shoulder (OAKS) Clinic, 707 Panchshil Plaza, N S Patkar Marg, opp. Ghanasingh Fine Jewels, next to Dharam Palace, Gamdevi, Mumbai. Maharashtra - 400 007. India. E-mail: dramrajani@gmail.com
Abstract
Introduction: Lesser tuberosity avulsion fractures are rare and often missed. Patients often complain only of heaviness around the shoulder and some loss in range of motion.
Case Report: This is a rare case of a lesser tuberosity avulsion fracture with displacement. The patient was a 29-year-old male who suffered an injury to the right shoulder due to a fall. Post-fall, the patient developed typical heaviness and restrictions in the range of motion of his right shoulder. Radiographs initially taken were not true anteroposterior (AP) views. The fracture was primarily missed by another surgeon, after which on opting for a true AP radiographs, the fracture was diagnosed. The fracture was managed by an open deltopectoral approach. Fracture fragment was reduced to its footprint and was fixed using 2 × 4.0 mm cancellous screws. Post-surgery, the patient was advised 3 weeks of immobilization after which mobilization was started. By monitored physiotherapy, consistent results can be obtained without loss of reduction. In this case too, full ranges with strength were achieved by 3 months postoperatively.
Conclusion: Such fractures often missed may cause loss of external rotation movements in the patient and eventually malunion of the fragment if displaced. Watchfulness and timely management of the fractures can give excellent results. This case report aims at increasing the awareness among the budding shoulder surgeons in identifying such injuries at the earliest, and the means of managing them.
Keywords: Lesser tuberosity, avulsion, subscapularis, heaviness, loss of rotation, deltopectoral approach.
Abduction injury or even direct trauma to the shoulder is commonly associated with proximal humerus or greater tuberosity isolated fracture. However, due to the anatomical location of lesser tuberosity lying anteriorly, it is less commonly involved in traumatic injuries. Isolated avulsion fracture of the lesser tuberosity is an unusual phenomenon that usually occurs in association with fractures involving two or three segments of proximal humerus or as a part of a posterior fracture dislocation [1,2,3]. The typical mechanism of injury is an abduction external rotation trauma to the shoulder [2,4,5]. Using this case report, we intend to throw light on such rare presentations, which if not watchful can be easily missed
The patient, a 29-year-old male, due to COVID-19 infection, was under monitoring at home when due to sudden drop in saturation, fell down on the ground with the right arm externally rotated, and abducted with the right shoulder impacting the ground first. The patient, being unconscious, was immediately shifted to the hospital and was kept under intensive care. The patient regained consciousness after 3 days. The patient immediately started feeling heavy in the right shoulder with some restriction in movements. The patient was advised to have a portable radiograph in the intensive care units, where fracture was missed (Fig. 1).
On finishing the treatment of COVID-19, the patient presented to us and a fresh set of radiographs were taken (Fig. 2). This was 14 days post-injury. The patient was diagnosed with non-displaced greater tuberosity fracture along with lesser tuberosity displaced fracture, with restriction in external rotation and weakness in internal rotation. 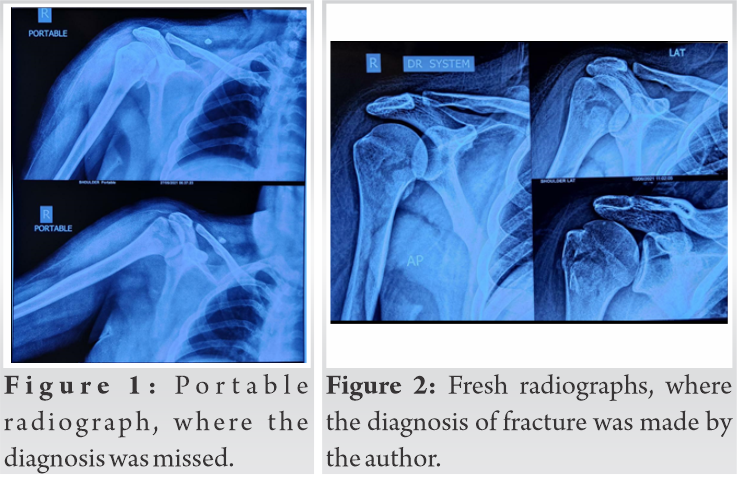
To identify the integrity of the subscapularis muscle, magnetic resonance imaging (MRI) was advised. MRI was clearly suggestive of subscapularis avulsion fracture (Fig. 3).
Computed tomography (CT) scan was also done to define the bone size and displacement from its original position (Fig. 4).
The patient was planned for an open subscapularis repair and lesser tuberosity reduction surgery.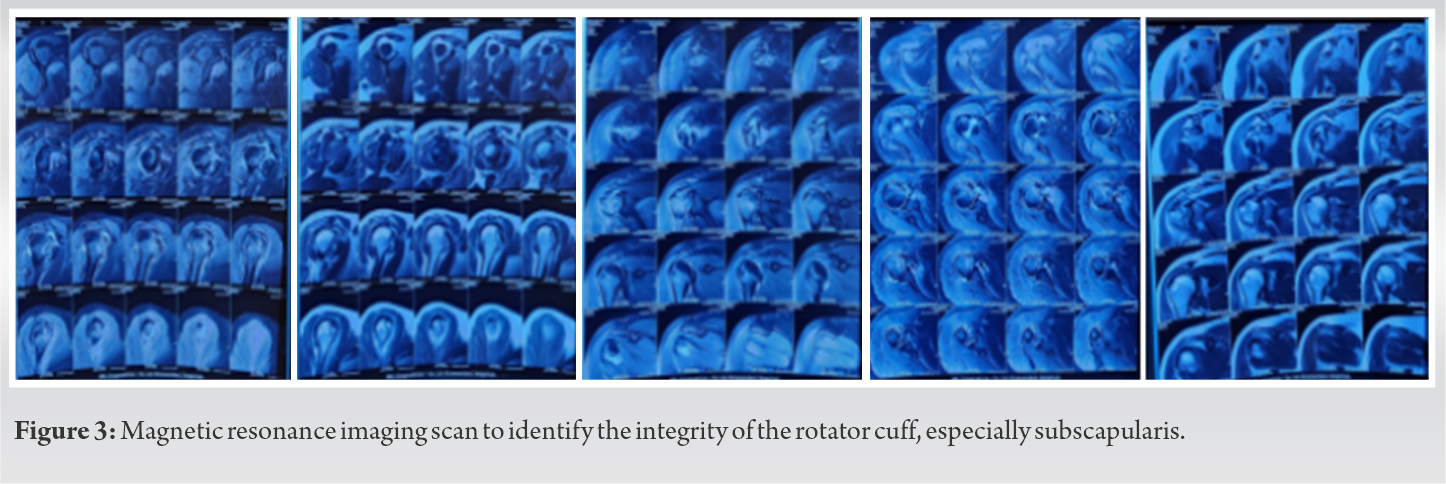
Deltopectoral approach was chosen and the lesser tuberosity fragment was identified. Along with the torn fibers of subscapularis tendon, the fragment was mobilized and fracture site was cleared for any fibrotic callus. The fragment on complete reduction was fixed using 2 4.0 mm cancellous screws. Greater tuberosity fragment was undisplaced with early signs of union, so was left alone (Fig. 5). Post-fixation, the patient was immobilized for a period of 3 weeks.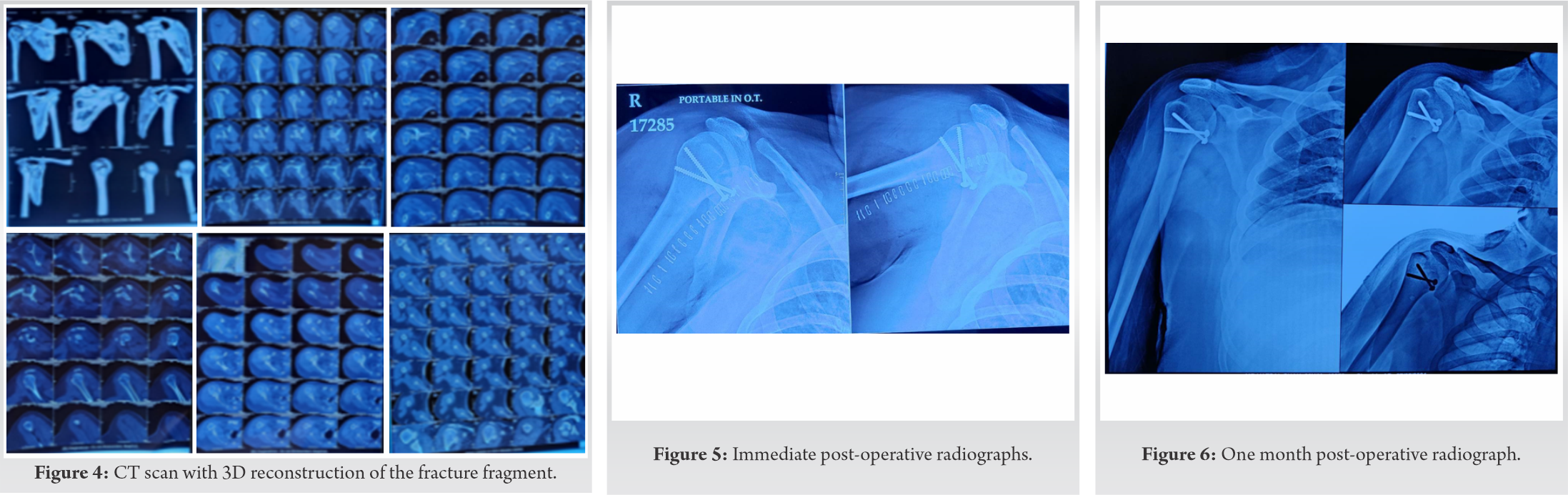
The patient was then eventually mobilized with pendulum movements and progressive range of motion exercises. The patient achieved near-complete passive ranges of motion at 4 weeks postoperatively (Fig. 6). Muscle activation exercises were started, followed by progressive strengthening of the muscles.
At 3 months follow-up, the patient has normal ranges of motion with complete union of the fracture fragment and full scar integrity (Fig. 7, 8).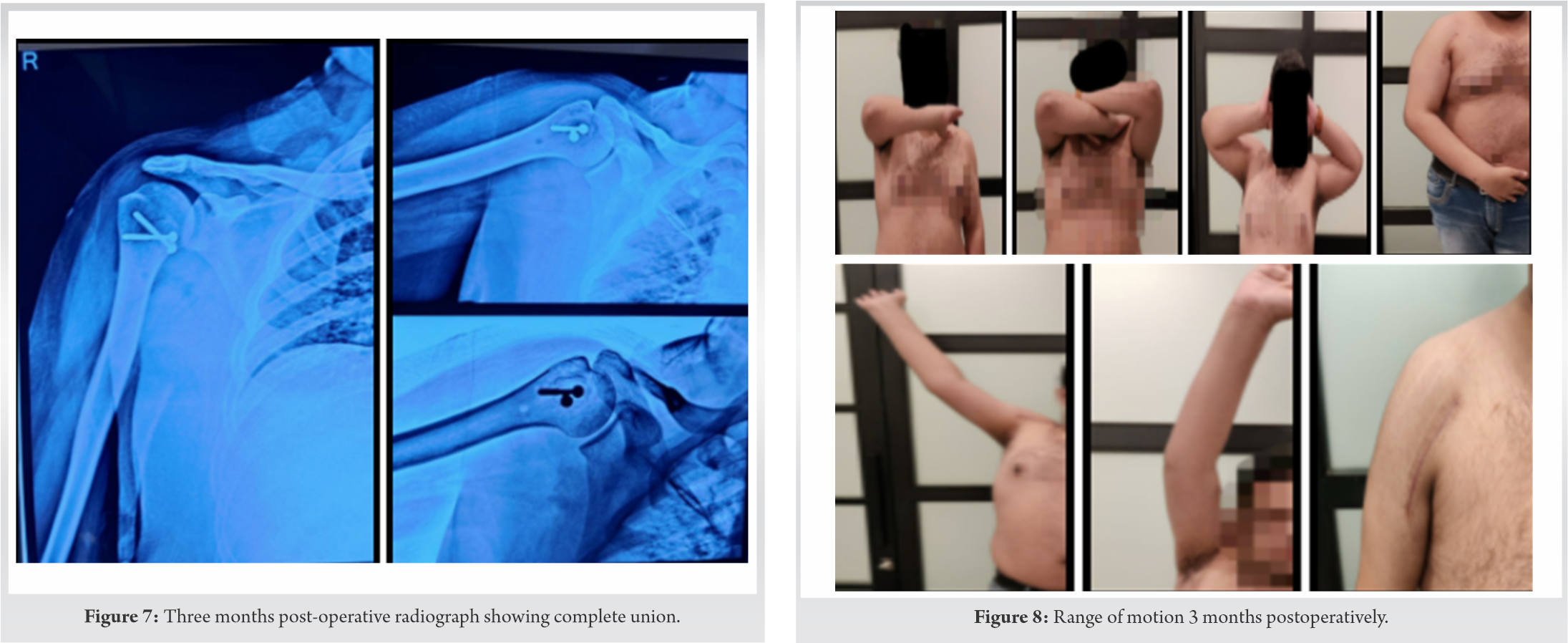
The lesser tuberosity is protected from direct injury by its small size and its location on the medial side of the head of the humerus. Therefore, most of the authors believe that the main mechanism of injury is muscular violence. When the subscapularis muscle forcefully contracts to resist abduction and external rotation of the shoulder, it is forced to extend, and the resultant strong traction force thus avulses the lesser tuberosity [3].
Similar incident had occurred with our patient causing him pain, heaviness, and sudden restriction in the range of motion in the affected shoulder.
It is very easy to miss these kinds of fractures. An anteroposterior (AP) view in maximal internal rotation projects the lesser tuberosity in profile and may be helpful in diagnosis. Large displaced fractures can be easily seen on standard AP radiographs, but the axillary view is often necessary to detect smaller fragments with minimal displacement [4,6,7,8].
In our case, because an AP radiograph was unable to completely delineate the fracture fragment, we went on to get a radiograph in maximum internal rotation. This technique works well to delineate most of the lesser tuberosity fractures.
Diagnosis also needs support of additional diagnostic modalities such as CT scan and MRI. CT scan can help us detect the actual size and thickness of the fragment. MRI, on the other hand, can be used to detect soft-tissue injuries such as avulsion of rotator cuff and isolated subscapularis avulsion. MRI can identify the injury at the subscapularis tendon footprint with variable size and displacement [9].
Once diagnosed, management of lesser tuberosity avulsion fracture can be done in three ways: Conservatively by immobilization, open reduction and internal fixation, and surgical excision of fracture fragment. The conservative treatment may be an effective alternative to open reduction and internal fixation, even in acute cases of isolated lesser tuberosity fractures as long as the long head of the biceps tendon is not dislocated [10].
Surgical reduction and suture fixation is safe and effective in restoring subscapularis function and return to sports, even in cases of delayed treatment. Full recovery of shoulder external rotation may not be seen until 6 months postoperatively [11]. However, in our case, full recovery of the fracture site with near-complete ranges of motion was achieved.
By this research article, we want to conclude that watchfulness for the identification of lesser tuberosity avulsion fracture is inevitable. It has some clear indicative signs such as feeling of heaviness in the shoulder, loss of external rotation of the shoulder, and restriction in other ranges of motion. This can be confused with a rotator cuff tear in some cases but MRI can help distinguish the soft-tissue involved. Furthermore, method of fixation can vary from suture repair to needle suture anchor to screw fixation depending on the size of the fragment. Rehabilitation and close follow-up can help achieve complete range of motion and strength as well.
Isolated Lesser Tuberosity fractures of Humerus are rare and can be missed easily, identifying and fixing these fractures early can lead to excellent clinical outcomes.
References
- 1.Levine B, Pereira D, Rosen J. Avulsion fractures of the lesser tuberosity of the humerus in adolescents: Review of the literature and case report. J Orthop Trauma 2005;19:349-52. [Google Scholar | PubMed]
- 2.van Laarhoven HA, te Slaa RL, van Laarhoven EW. Isolated avulsion fracture of the lesser tuberosity of the humerus. J Trauma 1995;39:997-9. [Google Scholar | PubMed]
- 3.Ogawa K, Takahashi M. Long-term outcome of isolated lesser tuberosity fractures of the humerus. J Trauma 1997;42:955-9. [Google Scholar | PubMed]
- 4.Ross GJ, Love MB. Isolated avulsion fracture of the lesser tuberosity of the humerus: Report of two cases. Radiology 1989;172:833-4. [Google Scholar | PubMed]
- 5.Pace A, Ribbans W, Kim JH. Isolated lesser tuberosity fracture of the humerus. Orthopedics 2008;31:94. [Google Scholar | PubMed]
- 6.Earwaker J. Isolated avulsion fracture of the lesser tuberosity of the humerus. Skeletal Radiol 1990;19:121-5. [Google Scholar | PubMed]
- 7.Scheibel M, Martinek V, Imhoff AB. Arthroscopic reconstruction of an isolated avulsion fracture of the lesser tuberosity. Arthroscopy 2005;21:487-94. [Google Scholar | PubMed]
- 8.Shibuya S, Ogawa K. Isolated avulsion fracture of the lesser tuberosity of the humerus. A case report. Clin Orthop Relat Res 1986;211:215-8. [Google Scholar | PubMed]
- 9.Bedoya MA, Barrera CA, Bencardino JT, Ho-Fung V. Humeral lesser tuberosity avulsion fractures magnetic resonance imaging characteristics in the pediatric population. Pediatr Radiol 2021;51:1421-30. [Google Scholar | PubMed]
- 10.Athanasiadis LP, Petropoulou ET, Neonakis EM. Conservative treatment of isolated avulsion fracture of the lesser tuberosity of the humerus: A case report. J Res Pract 2017;1:38-40. [Google Scholar | PubMed]
- 11.Vezeridis PS, Bae DS, Kocher MS, Kramer DE, Yen YM, Waters PM. Surgical treatment for avulsion injuries of the humeral lesser tuberosity apophysis in adolescents. J Bone Joint Surg Am 2011;93:1882-8. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 10, 2024 V-Y Quadricepsplasty for Knee Stiffness Post Total Knee Arthroplasty: A Case Report and Literature Review
June 10, 2024 V-Y Quadricepsplasty for Knee Stiffness Post Total Knee Arthroplasty: A Case Report and Literature Review July 1, 2025 Management of Large Osteochondral Fracture of the Patella in an Adolescent: A Rare Case Report
July 1, 2025 Management of Large Osteochondral Fracture of the Patella in an Adolescent: A Rare Case Report July 11, 2014 Simple Bone Cyst of Metacarpal: Rare Lesion with Unique Treatment
July 11, 2014 Simple Bone Cyst of Metacarpal: Rare Lesion with Unique Treatment April 10, 2024 Is Modular Prosthesis Superior to Monoblock Variant in Hemiarthroplasty for Fracture Neck of Femur?
April 10, 2024 Is Modular Prosthesis Superior to Monoblock Variant in Hemiarthroplasty for Fracture Neck of Femur?