
Missed Monteggia injuries in children are complex problems that require a step-by-step approach and surgical treatment.
Dr. Dimitrios G Begkas, Department of Orthopaedics, Asclepieion Voulas General Hospital, 1 Vasileos Pavlou Street, Voula - 16673, Athens, Greece. E-mail: drdbegkas@gmail.com
Abstract
Introduction: Monteggia injuries are relatively rare in the pediatric population. They can be missed leading to complications arising from a chronic radial head dislocation. There is limited information about their proper management in the literature. Thus, their treatment remains controversial.
Case Report: We present a case of a 10-year-old boy who was examined in the orthopedic outpatient clinic of our hospital, due to limited range of motion of his left elbow and difficulty in extending his left thumb, after a forearm injury which occurred 9 months before and was initially treated conservatively. After appropriate imaging was obtained, a Bado type I Monteggia lesion was diagnosed. This was treated by open reduction of the head of radius, osteotomy of the ulna and lengthening using an external fixator, as well as annular ligament reconstruction by the use of synthetic tendon graft. The patient was followed up for 18 months after surgery and during his last examination showed very good clinical and functional results.
Conclusion: Missed Monteggia injuries in children are complex problems warranting a step-by-step approach. Their management with ulnar osteotomy, bone lengthening, and reconstruction of the annular ligament presents a viable option with excellent clinical, functional, and radiological outcomes.
Keywords: Children, dislocation, external fixation, Monteggia fracture, osteotomy, ulna.
Monteggia injuries consist of a dislocation of the head of radius combined with a fracture or plastic deformation of the ulna. There are relatively rare and constitute 1% of all pediatric fractures [1]. A missed Monteggia lesion is defined as a dislocation of the head of radius that remains unreduced for at least 4 weeks after injury [2,3]. Although there is disagreement in the literature about proper management of these injuries, their surgical treatment is usually recommended in patients who experience pain, loss of elbow motion, and functional problems, but the morphology of the concave surface of the head of radius is preserved [4]. Persistent chronic posterior interosseous nerve (PIN) palsy in the setting of a chronic dislocation of the head of radius is rare [5,6].
We present this case to demonstrate a step-by-step approach to a complex problem and its management using an advanced and highly effective surgical technique.
In August 2016, a 10-year-old boy presented to the orthopedic outpatient clinic of our hospital, complaining of limited range of motion of the left elbow as well as difficulty in extending the left thumb. There was a history of an injury to his left forearm 9 months ago, which was initially treated conservatively. Unfortunately, the patient had come from another country and had no previous radiographs. Clinical examination revealed difficulty to flex and inability to rotate his left elbow. Specifically, the patient presented: 90° flexion, 70° pronation, 20° loss in extension, and almost no supination. His Mayo Elbow Performance Score was poor (55/100). The anteroposterior and lateral radiographs of the left elbow showed an anterior dislocation of the radial head (Fig. 1a and b). We concluded that the patient had most probably suffered a Monteggia Bado type I fracture which had been missed and therefore gone untreated. A computed tomography scan of the left elbow was performed to determine if there were any bony fragments in the joint. However, there were no intra-articular fragments.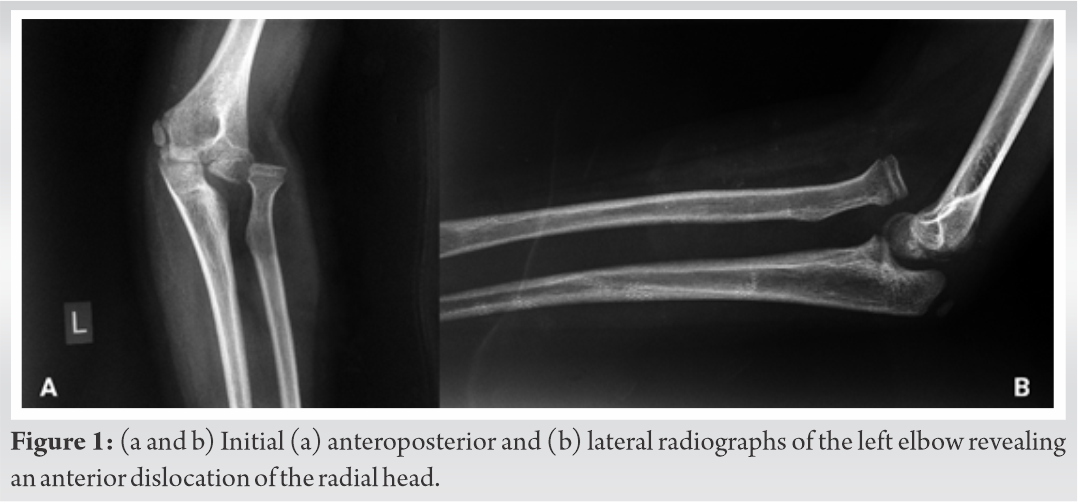
The patient’s main complaint was the difficulty of extending his thumb. Parents were also concerned about serious limitations in elbow range of motion. For these reasons, it was decided to try to reduce the radial head. The patient was taken to the operating theater and an above elbow tourniquet was placed. A posterolateral Boyd’s approach was utilized. Initially, the humeroradial joint was cleared of scar tissue and of the remains of the annular ligament. The radial head could only be partially reduced, so we had to perform a proximal ulnar osteotomy. To be able to distract the osteotomy, we applied a mini rail external fixator to the ulna and proceeded to perform a proximal ulnar osteotomy. At that point, the radial head was found to sublux during supination and pronation. Therefore, annular ligament reconstruction was performed using a synthetic tendon graft and anchor sutures (Fig. 2). In addition, the radiocapitellar joint was fixed with a Kirschner wire. Given the fact, the PIN was not found to be interpositioned within the radiocapitellar joint or the proximal radioulnar joint, we did not proceed to a nerve exploration. After surgery, the arm was placed in an above elbow half cast. Post-operative radiographs were obtained, showing an adequate radiocapitellar alignment (Fig. 3). Bone elongation started 7 days postoperatively at a rate of 1 mm per day, until a distraction of 8 mm was achieved (Fig. 4).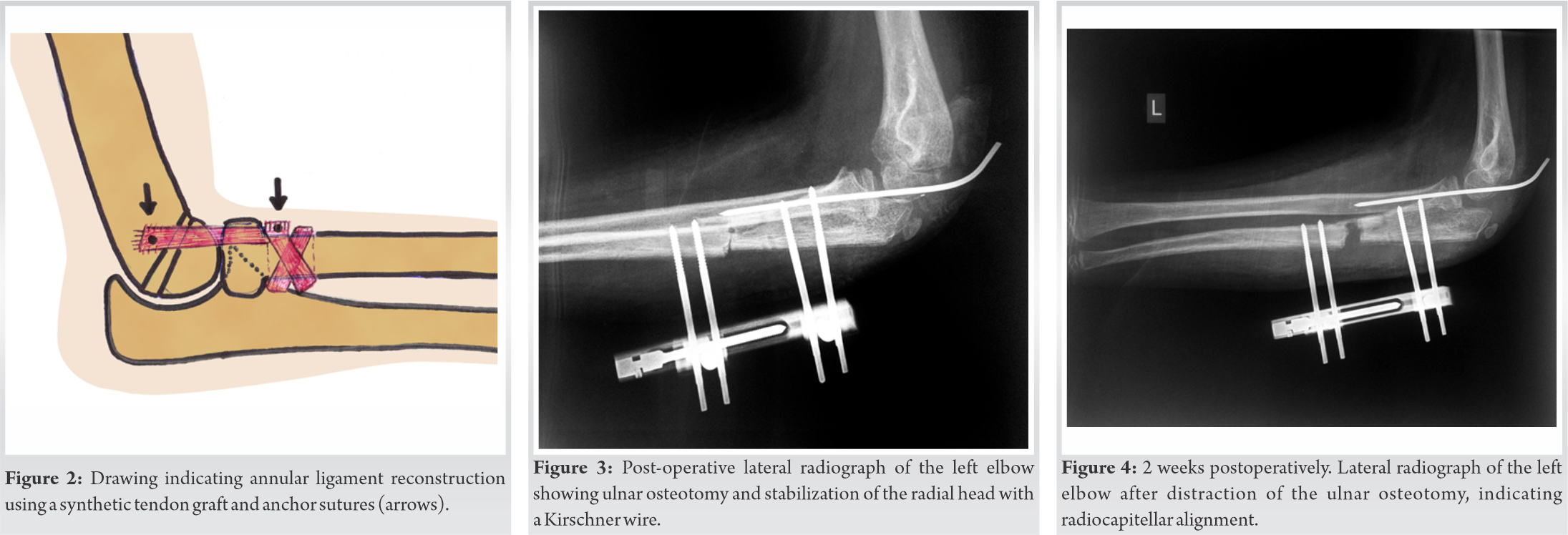
The radiocapitellar k-wire was removed 1 month postoperatively. Union of the ulna was achieved at 3 months after surgery and the external fixator was removed (Fig. 5a). The patient was followed up until 18 moths postoperatively (Fig. 5b). During his final examination, the range of motion of the left elbow improved to: 150° flexion, 80°pronation, 70° supination, and only 10° loss in extension (Fig. 6a and b). His Mayo elbow performance score was excellent (100/100). In addition, the extension of his thumb was also improved.
In a long-standing Monteggia lesion, usually, the first step is to clear the radiocapitellar joint of the remains of the annular ligament and fibrotic tissue that do not allow the reduction of the head of radius [7]. If the reduction remains unstable, then an ulnar osteotomy is performed [8]. If needed, lengthening of the ulna can be added. The whole fixation can be achieved by the use of a precontoured plate with or without bone grafts [9]. In a case series of 30 chronic Monteggia lesions treated by open reduction and plate fixation, there were generally good outcomes.
In another study, the authors have proposed an alternative method of ulnar lengthening, using an external fixation device and gradual reduction of the head of radius by closed means, which was successful in a total of four cases [10]. However, this is a long process which, if not successful, will require a second open radial head reduction procedure. Recently, a technique of ulnar osteotomy with angulation and lengthening, using a temporary external fixation device, followed by definitive plate fixation and open reduction of the dislocated head of radius has been described, which was overall successful in 13 cases [11].
Annular ligament reconstruction with the Bell Tawse procedure, where a strip of triceps or forearm fascia is used, remains controversial and there is a lack of long-term data reported. In a case series of 22 patients who all underwent open reduction of the radial head, ulnar osteotomy, and annular ligament reconstruction, the radial head remained in a completely reduced position in seventeen patients at long-term follow-up [12]. In a similar case series, where 13 patients underwent annular ligament reconstruction, the radial head remained reduced in 12 of them at long-term follow-up [13].
Persistent, chronic PIN palsy in the setting of a chronic radial head dislocation is an extremely rare condition [5,6]. In a case report of persistent complete PIN palsy in a patient with a chronic type I Monteggia elbow fracture dislocation who was treated with open reduction of the head of radius and exploration of the nerve, the authors hypothesize that in chronic anterior dislocation of the head of radius, a compressive neuropathy can be developed secondary to cicatrix overlying the capsule as well as the chronic compression of the nerve at the arcade of Froshe. They recommend formal open reduction of the radial head and examination of the radiocapitellar joint and proximal radioulnar joint to identify PIN subluxation or incarceration [14]. In our case, the PIN was not found to be interpositioned within these two joints and we did not proceed to nerve exploration.
In a recently published case report, the authors described the reduction of a 4-week-old Monteggia lesion in a 6-year-old child by open reduction, gradual bone lengthening of the ulna by external fixator and reconstruction of the annular ligament using the Bell Tawse method. The patient was followed-up 1 year after the procedure showing good radiological and clinical results [15].
In our case, where we had a 9-month-old Monteggia lesion, we first tried to reduce the radial head and then clear the radiocapitellar joint. The inability to reduce the radial head led us to perform an ulnar osteotomy. Due to the fact that lengthening was required, we decided to use an external fixator with a lengthening device to achieve gradual lengthening and avoid the need for grafting. The external fixator offered us the additional advantage of its removal without the need for a second operation. Remaining instability at the time of surgery led us to perform an annular ligament reconstruction. We used a synthetic tendon graft and anchor sutures to minimize surgical time as well as donor site morbidity. Fixation of the radiocapitellar joint by a Kirschner wire was added to increase stability. After 18 months of follow-up, during his final examination, our patient presented excellent clinical, functional, and radiological results and was able to return to his normal pre-injury daily and athletic activities without any problems. As we can see, through the aforementioned surgical technique, we were able to deal step by step with all the difficulties that arose from this complex injury and in the end to have an excellent result.
Missed Monteggia lesions may be complicated by serious limited functionality and, therefore, require a step-by-step approach and surgical treatment. In long-standing cases, open reduction of the radial head and clearing and exploration of the joint should be the first step, especially when there is a neurological deficit. Ulnar osteotomy and lengthening, where needed, can be performed with the aid of an external fixator allowing for gradual lengthening. This avoids the need for grafting as well as a second operation for removal of hardware. Annular ligament reconstruction could be reserved for the cases when, after the ulnar osteotomy there is remaining instability. Synthetic tendon graft is a good alternative, saving time, and limiting donor site morbidity.
Missed Monteggia injuries in children are complex problems that can be complicated by severely limited functionality and disability of the patient and, therefore, require a step-by-step approach and surgical treatment.
References
- 1.Ring D, Jupiter JB, Waters PM. Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-24. [Google Scholar | PubMed]
- 2.Hui JHP, Sulaiman AR, Lee HC, Lam KS, Lee EH. Open reduction and annular ligament reconstruction with fascia of the forearm in chronic monteggia lesions in children. J Pediatr Orthop 2005;25:501-6. [Google Scholar | PubMed]
- 3.Song KS, Ramnani K, Bae KC, Cho CH, Lee KJ, Son ES. Indirect reduction of the radial head in children with chronic Monteggia lesions. J Orthop Trauma 2012;26:597-601. [Google Scholar | PubMed]
- 4.Bae DS. Successful strategies for managing Monteggia injuries. J Pediatr Orthop 2016;36:67-70. [Google Scholar | PubMed]
- 5.Chang MC, Liu Y, Lo WH. Wraparound injury of posterior interosseous nerve on the unreduced radial head: A case report. Zhonghua Yi Xue Za Zhi (Taipei) 1996;58:459-63. [Google Scholar | PubMed]
- 6.Osamura N, Ikeda K, Hagiwara N, Tomita K. Posterior interosseous nerve injury complicating ulnar osteotomy for a missed Monteggia fracture. Scand J Plast Reconstr Surg Hand Surg 2004;38:376-8. [Google Scholar | PubMed]
- 7.Stoll TM, Willis RB, Paterson DC. Treatment of the missed Monteggia fracturein the child. J Bone Joint Surg Br 1992;74:436-40. [Google Scholar | PubMed]
- 8.Hirayama T, Takemitsu Y, Yagihara K, Mikita A. Operation for chronic dislocation of the radial head in children. Reduction by osteotomy of the ulna. J Bone Joint Surg Br 1987;69:639-42. [Google Scholar | PubMed]
- 9.Delpont M, Louahem D, Cottalorda J. Monteggia injuries. Orthop Traumatol Surg Res 2018;104:113-20. [Google Scholar | PubMed]
- 10.Bor N, Rubin G, Rozen N, Herzenberg JE. Chronic anterior Monteggia lesions in children: Report of 4 cases treated with closed reduction by ulnar osteotomy and external fixation. J Pediatr Orthop 2015;35:7-10. [Google Scholar | PubMed]
- 11.Wang Q, Du M, Pei X, Luo J, Li Y, Liu Y, et al. External fixator-assisted ulnar osteotomy: A novel technique to treat missed Monteggia fracture in children. Orthop Surg 2019;11:102-8. [Google Scholar | PubMed]
- 12.Nakamura K, Hirachi K, Uchiyama S, Takahara M, Minami A, Imaeda T, et al. Long-term clinical and radiographic outcomes after open reduction for missed Monteggia fracture-dislocations in children. J Bone Joint Surg Am 2009;91:1394-404. [Google Scholar | PubMed]
- 13.Wang MN, Chang WN. Chronic posttraumatic anterior dislocation of the radial head in children: Thirteen cases treated by open reduction, ulnar osteotomy and annular ligament reconstruction through a Boyd incision. J Orthop Trauma 2006;20:1-5. [Google Scholar | PubMed]
- 14.Ruchelsman DE, Pasqualetto M, Price AE, Grossman JA. Persistent posterior interosseous nerve palsy associated with a chronic Type I Monteggia fracture-dislocation in a child: A case report and review of the literature. Hand (NY) 2009;4:167-72. [Google Scholar | PubMed]
- 15.Shinohara D, Yasuda T, Arai M, Sato K, Arima T, Kanzaki K. A long-standing Monteggia fracture in a child who underwent bone lengthening and annular ligament reconstruction: A case report. J Orthop Case Rep 2019;9:30-3. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2016 Treatment of Stiff Elbow in Young Patients with Interpositional Arthroplasty for Mobility: Case Series
October 10, 2016 Treatment of Stiff Elbow in Young Patients with Interpositional Arthroplasty for Mobility: Case Series October 11, 2013 Ipsilateral Fracture Shaft Femur with Neglected Dislocation of Prosthesis: A Case Report
October 11, 2013 Ipsilateral Fracture Shaft Femur with Neglected Dislocation of Prosthesis: A Case Report May 10, 2023 Subacute Bacterial Infection Mimicking a Slipped Capital Femoral Epiphysis in an Obese Adolescent Male – A Case Report and Review of Literature
May 10, 2023 Subacute Bacterial Infection Mimicking a Slipped Capital Femoral Epiphysis in an Obese Adolescent Male – A Case Report and Review of Literature July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report