
CCJ instability is not only traumatic case but also can be due to repetitive movements and can be treated using the peroneus brevis as a local autograft for ligamentoplasty.
Dr. Fanny Pierret, Department of Orthopaedic, Orthopeadic Surgery Resident, CHU Sart-Tilman 1, Avenue de l’Hopital, 4000 Liège, Belgium. E-mail: fpfanny6@gmail.com
Abstract
Introduction: Most calcaneocuboïd joint (CCJ) subluxations are traumatic, secondary to a high-energy flexion-supination mechanism. We describe here a case of atraumatic chronic subluxation of the CCJ which is a rare, difficult to diagnose condition. Moreover, we describe a surgical technique using a peroneus brevis autograft hemi-tendon, which has not been yet published in the literature.
Case Presentation: A 58-year-old woman presented initially for a painful right hallux. A careful clinical examination revealed tenderness of the lateral side of the foot. The intensity of the pain had been increasing for the past 5 years, due to repetitive movements of pronosupination of the mid-foot. As it turned out, this repetitive movement was caused by the daily use of a floor scrubber for her work as a janitor, resulting in a chronic CCJ instability. The foot computed tomography (CT) scan confirmed the CCJ subluxation with an osseous avulsion on calcaneal apophysis, proof of ligamentous injury.
Conclusions: We present a rare case of atraumatic CCJ subluxation, due to overuse activity. Calcaneocuboid joint instability is difficult to diagnose. Anamnesis is critical to understand which pathologic movements are responsible for joint instability. CT scan is helpful. As a treatment, we used an innovative surgical technique similar to the hemi-Castaing procedure used for chronic ankle instability. This technique, which has not been yet described in the literature, is simple, non-invasive, and reconstructs the dorsal calcaneocuboid ligament and part of the bifurcate ligament.
Keywords: Calcaneocuboïd joint injury, subluxation, chronic instability, surgical treatment.
Mostly, calcaneocuboïd joint (CCJ) instability is a traumatic injury due to an inversion mechanism [1]. Lateral ligaments of the ankle are usually involved in the inversion mechanism. However, in a minority of cases, it concerns the foot’s ligament, with an isolated calcaneocuboid injury. Andermahr et al. reviewed of 13 cases of isolated CCJ injury and proposed a grading system for CCJ instability based on anteroposterior varus stress radiography [2].
We describe here a case of atraumatic CCJ instability, for which anamnesis was crucial to diagnose. We present also a novel technique of calcaneocuboid ligament reconstruction, which is similar to the hemi-Castaing procedure in ankle instability.
The patient was a healthy 58-year-old woman. She was not overweight nether sporty. She worked as a janitor in a hospital and used daily a floor scrubber. The medical history began in August 2017 when the patient presented with a painful right hallux and a stiff right heel. The clinical examination confirmed the heel pain and a dynamic varus hallux deformity. The hallux deformity was only present with weight-bearing. Initially, there was not any lateral foot pain. We made weight-bearing radiography of the two feet and a foot magnetic resonance imaging (MRI). On the right foot, there was a calcaneal spur. The Djian-Annonier angle was 129° (range between 120 and 130°). The talocalcaneal divergence was 17° on the face (range between 15 and 20°) and 27.6° on the profile (range between 20 and 30°). The calcaneal-fifth metatarsal angle was 0° (Figs. 1 and 2). There was no sign of tibiotalar, midfoot, or metatarsophalangeal joints arthrosis. There was no sign of hallux valgus or varus deformation. There were signs of plantar fasciitis and fibular and posterior tibial tenosynovitis on foot MRI but no sign of lesion of the calcaneocuboid ligaments (Fig. 3).
As a conservative treatment, we prescribed a sole with medial arch support and heel recess and we performed an infiltration of the first metatarsophalangeal joint. The patient came back in June 2020, complaining of the right hallux pain again. A new clinical examination revealed tenderness at the CCJ palpation. There was an increase in CCJ motion compared to the contralateral foot and pain increased with midfoot inversion. A foot CT scan in a supine position was performed and showed a CCJ subluxation with an inferior tilt of the cuboid. There was an osseous avulsion on the calcaneal-apophysis but no arthrosis either in the hindfoot or either in the midfoot (Fig. 4). We did not perform an infiltration of the CCJ as a diagnostic or therapeutic use. Indeed, the localization and the joint source of pain were obvious and any infiltration was needed to confirm it.
Although the patient was initially consulted for a painful hallux deformity, the anamnesis, clinical examination, and foot CT scan pointed to a Chopart joint injury. Because of the joint instability and the risk of joint degeneration, a surgical approach was indicated. A CCJ ligamentoplasty was planned to treat this subluxation. Given the absence of joint arthrosis, arthrodesis was not indicated.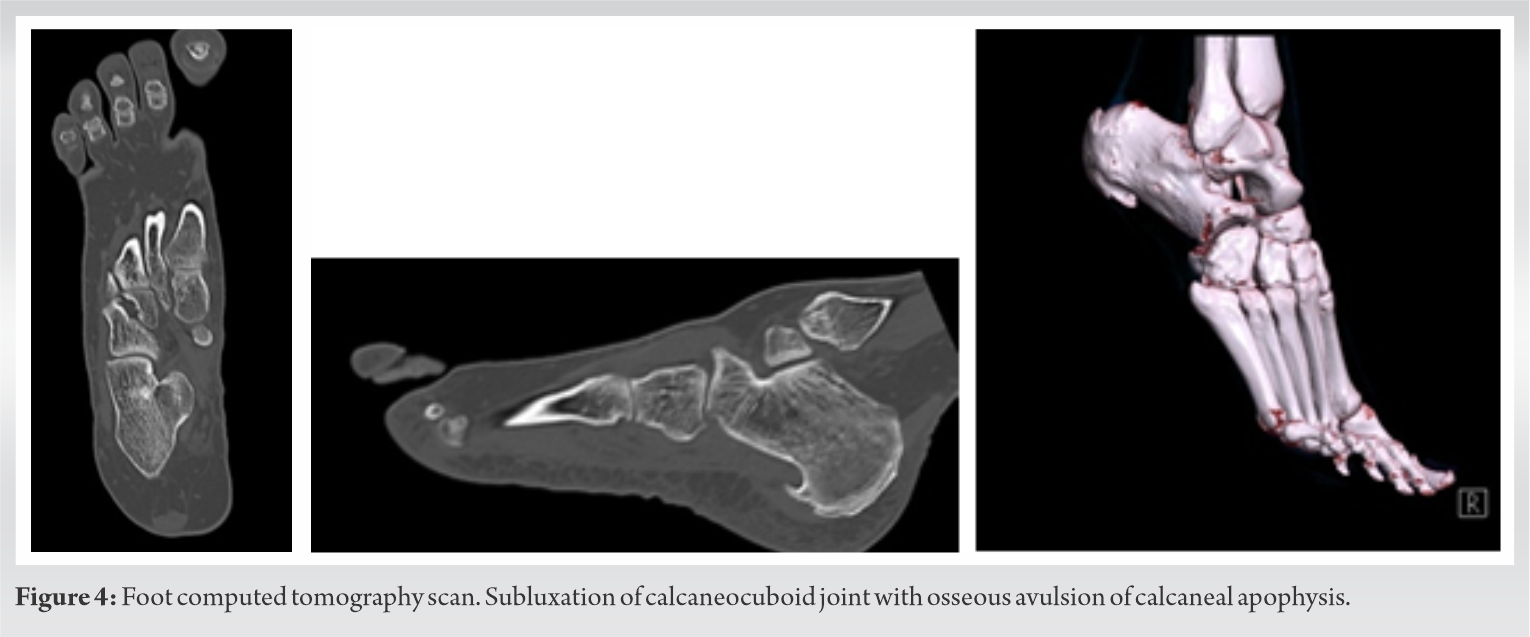
The patient was followed with control at 2, 6, and 12 weeks then 6 months and 1 year post-operative. Radiography was done at 6 weeks (Fig. 5). The evolution was excellent, without any pain, and a complete return to her work and her activities at 1 year post-operative.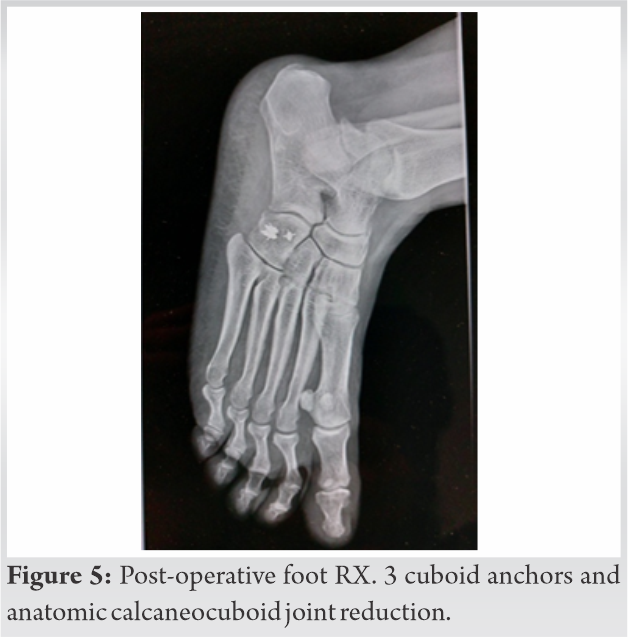
The patient was in a supine position with a pillow under her right buttock. Landmarks structures were identified with palpation: lateral malleolus, CCJ, and 5th metatarsal base. An antibiotic prophylaxis with 2 g of cefazoline was given. We used a thigh tourniquet inflated at 300 mmHg. First, we performed a 5 cm straight incision perpendicular to the CCJ. The peroneus longus and brevis tendons were identified. There was a cracking of the distal portion of the short fibular tendon. The two tendons were reclined in a posteroinferior position. Instability of the CCJ was confirmed with supination, inversion, and plantar flexion of the foot. There was a complete section of the dorsolateral calcaneocuboid ligament and a partial section of the bifurcate ligament. There was not any sign of cartilage injury (Fig. 6).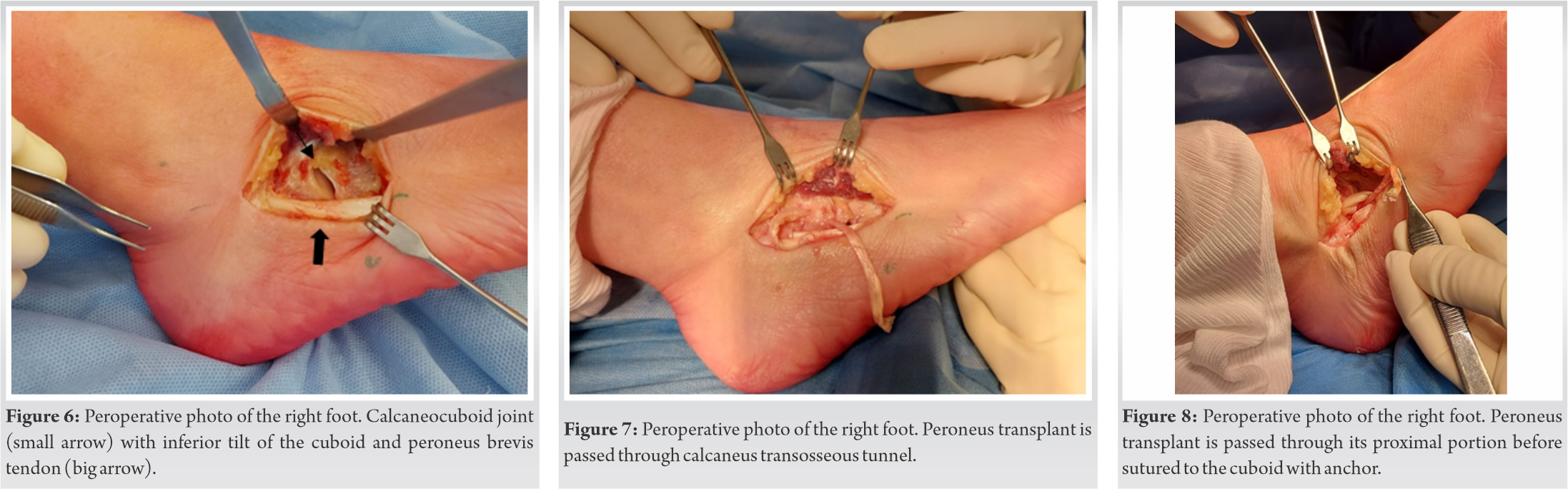
Two more incisions were made along the peroneus tendon; one at the myotendinous junction and one just above the retinaculum. We dissected the peroneus brevis tendon and performed a proximal hemisection of the tendon. The hemi-tendon was passed under the fibular retinaculum, used as a fibular transplant.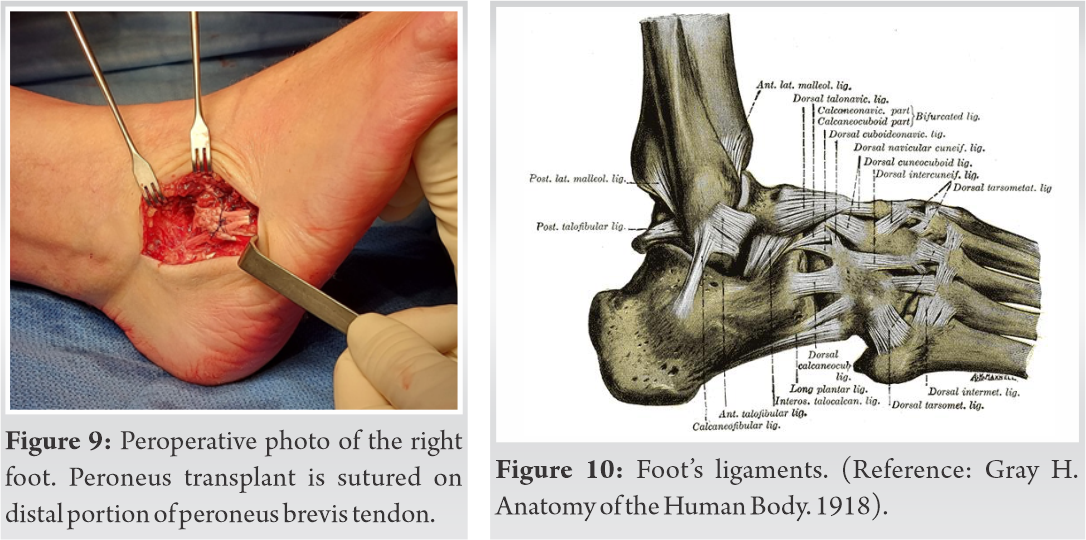
We performed a calcaneal transosseous tunnel with a 3.5 mm drill bit. The transplant was passed through the tunnel (Fig. 7), through its proximal portion (Fig. 8), and then sutured to the cuboid with three anchors (Fig. 9), with the foot in eversion (rotator cuff anchor DePuy®). The distal portion of the transplant was sutured on the proximal portion with an overcoat suture and resulted in an anatomical and stable joint reduction confirmed clinically and with peroperative fluoroscopy (Fig. 9). The peroperative and post-operative radiography confirmed the good position of the implant. After the intervention, the patient was immobilized in a plaster splint for 2 weeks without weight-bearing and then in a walking plaster for 3 more weeks. After 5 weeks, weight-bearing was permitted without any brace. Physiotherapy was started at 6 weeks for 3 months.
Injuries of the CCJ are uncommon. Most injuries occur due to high-energy traumatisms, such as sport accidents [3] or falls [4]. The incidence is also higher in ballet dancers, due to pointe work [5,6,7,11]. They can also be caused by an inversion of the ankle, in a sprained ankle mechanism [8]. The mechanism is a forced inversion with plantar flexion. Pure ligamentous injuries are very rare due to the joint configuration. Indeed, CCJ is a stable joint, due to its good congruity and its saddle configuration. Calcaneocuboïd ligaments include the bifurcate ligament, the dorsolateral ligament, and the plantar ligaments (the long and the short) (Fig. 10). It is also reinforced with the longus peroneus tendon and the plantar fascia.
The main movements in the calcaneocuboid joint are medial and lateral rotations around an anteroposterior axis in the calcaneal process (like a pivot), responsible for the foot supination/pronation [1]. We discuss here the case of an atraumatic CCJ injury, resulting in a chronic CC joint instability with plantar subluxation of the cuboid. As previously mentioned, atraumatic CCJ injuries are very rare. The CCJ subluxation is a partial loss of joint congruity, due to capsule disruption, ligament laxity, and tendinitis. It causes lateral foot pain, swelling, and difficulty walking. Clinical diagnosis is not easy and a computed tomography (CT) scan seems to be helpful in this case objectifies the joint subluxation and osseous avulsion on calcaneal-apophysis. Anamnesis is critical in this case to understand the specific mechanism responsible for this instability. As mentioned above, the patient worked as a cleaning lady in a hospital. Her daily job consisted of using a washing ground robot which is a big engine difficult to manipulate. To counteract the engine’s moves, the patient had to block it with her right foot resulting in repeated forced foot inversions.
We performed a literature review on PubMed with the keywords: CCJ injury – subluxation – chronic instability – surgical treatment. Several surgical procedures have been described in the literature to treat CCJ instability. Without cartilage injury and arthrosis, the best treatment consists in CCJ ligament reconstruction without arthrodesis to preserve joint mobility and biomechanics of the foot. A variety of reconstructions have been used, such as tenodesis with the tendon of plantaris, peroneus brevis, gracilis, hamstring, extensor digitorum brevis muscle, and a periosteal flap.
Lorher and Arentz used a local periosteal flap to strengthen the dorsolateral calcaneocuboïd ligament with an anatomical ligament repair in an elite 13-year-old gymnast [9]. Andermarhr et al. [2] used a peroneus brevis autograft for reconstruction of Grade II of calcaneocuboid ligament injury. A gracilis tendon autograft was used in the case report described by Punwar and Madhav [11] to treat a 16-year-old professional female girl. Abyar et al. [12] used a semitendinosus allograft in a V-shaped configuration to treat an ankle sprain injury due to a motor collision in a 19-year-old girl. Hirschmann et al. [13] used a flap of the extensor digitorum brevis muscle to augment the dorsal calcaneocuboid ligament.In our case, we decided to use the peroneus brevis tendon autograft according to the hemi-Castaing ligamentoplasty used for lateral ankle instability [14]. A tenodesis of the split tendon was performed to repair the ligament disruption. Andermarhr et al. [2] described a technique using the whole peroneus brevis tendon, which is completely detached, to treat CCJ instability. In our technique, we used a hemi-tendon of peroneus brevis. The eversion peroneus brevis function is still partially preserved, with maintaining his distal insertion on the base of the 5th metatarsal. To the best of our knowledge, this technique has never been reported in the literature. This technique is a simple, non-invasive, and reproduces an anatomical reconstruction of the CC joint stability. Moreover, it preserves the biomechanics of the foot and does not compromise the lateral foot stability.
Recently, we had a similar case with an atraumatic CCJ injury. The diagnosis was more difficult to make and, here, we use a lidocaine infiltration in the CCJ to confirm the localization of the pain. Retrospectively, we think that diagnostic infiltration is not mandatory, but can help when the source of pain is not obvious.
Atraumatic CCJ instability is a rare cause of chronic lateral foot pain, which is difficult to diagnose but should be kept in mind when performing the clinical examination. Anamnesis is critical to understand the pathologic mechanism responsible for the instability. We recommend performing a foot CT scan and bilateral weight-bearing foot radiography to diagnose this dynamic instability. Several techniques can be used to reconstruct the calcaneocuboid ligaments. We recommend the use of peroneus brevis hemi-tendon autograft. The outcome at 1 year is excellent, without any pain, any walking trouble, and no daily activity limitation.
CCJ instability is not only traumatic case but also can be due to repetitive movements, consideration as an overuse pathology. Diagnosis is not easy because the pathology is non- well-known. As a surgical treatment, the peroneus brevis tendon can be used as a local autograft for ligamentoplasty. This technique is simple, non-invasive, and anatomical.
References
- 1.Draper TR. Non-Achilles Ankle Tendinopathy. United States: UpToDate; 2021. [Google Scholar | PubMed]
- 2.Andermahr J, Helling HJ, Maintz D, Monig S, Koebke J, Rehm KE. The injury of the calcaneocuboid ligaments. Foot Ankle Int 2000;21:379-82. [Google Scholar | PubMed]
- 3.Sheahan K, Pomeroy E, Bayer T. An isolated cuboid dislocation. A case report. Int J Surg Case Report 2017;39:1-4. [Google Scholar | PubMed]
- 4.Drummond DS, Hastings DE. Total dislocation of the cuboid bone: Report of a case. J Bone Joint Surg Br 1969;51:716-8. [Google Scholar | PubMed]
- 5.Adams E, Madden C. Cuboid subluxation: A case study and review of the literature. Curr Sport Med Rep 2009;8:300-7. [Google Scholar | PubMed]
- 6.Marshall P, Hamilton WC. Cuboid subluxation in ballet dancers. Am Sports Med 1992;20:169-75. [Google Scholar | PubMed]
- 7.Durall CJ. Examination and Treatment of cuboid syndrome: A literature review. Sport Health 2011;3:514-9. [Google Scholar | PubMed]
- 8.Dewar FP, Evans DC. Occult fracture-subluxation of the midtarsal joint. J Bone Joint Surg Br 1968;50:386-8. [Google Scholar | PubMed]
- 9.Lorher H, Arentz S. Calcaneocuboid joint instability: A novel operative technique for anatomic reconstruction. Foot Ankle Int 2004;25:349-56. [Google Scholar | PubMed]
- 10.Andermahr J, Helling HJ, Maintz D, Monig S, Koebke J, Rehm KE. The injury of the calcaneocuboid ligaments. Foot Ankle Int 2000;21:379-82. [Google Scholar | PubMed]
- 11.Punwar S, Madhav R. Dislocation of calcaneocuboid joint presenting as a lateral instability of the ankle. J Bone Joint Surg Br 2007;89:1247-8. [Google Scholar | PubMed]
- 12.Abyar E, Cone B, McKissack H, Johnson M. A novel technique in treatment of calcaneocuboid dislocation with bifurcate ligament reconstruction using a semitendinosus allograft. J Bone Joint Surg 2020;10:1-5. [Google Scholar | PubMed]
- 13.Hirschmann MT, Niklaus FF, Muller C. Anatomic reconstruction of a chronically instable calcaneocuboid joint with augmented extensor digitorum brevis muscle flap: A new method. Foot Ankle Int 2008;29:1258-61. [Google Scholar | PubMed]
- 14.Sperati G, Ceri L. Hemi-Castaing ligamentoplasty for the surgical treatment of chronic lateral ankle instability in young athletes: Our 7 years experience. Acta Biomed 2018;90:141-5. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 A Case Report of an Intra-Articular Lipoma in the Inferomedial Recess of the Anterior Knee Joint: Clinical Implications and Diagnostic Challenges: Case Report and Review of Literature
January 1, 2026 A Case Report of an Intra-Articular Lipoma in the Inferomedial Recess of the Anterior Knee Joint: Clinical Implications and Diagnostic Challenges: Case Report and Review of Literature July 30, 2019 Acute Traumatic Pseudo-pointing Index Finger Due to an Isolated Second Metacarpal-Trapezoid Dislocation: A Case Report
July 30, 2019 Acute Traumatic Pseudo-pointing Index Finger Due to an Isolated Second Metacarpal-Trapezoid Dislocation: A Case Report October 10, 2022 Case Report of Both Bone Forearm Refracture in an 8-year-old Girl
October 10, 2022 Case Report of Both Bone Forearm Refracture in an 8-year-old Girl June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study