
Of discussed case report, K-wire fixation one of the safest procedure with good clinical outcome for fractured bone cyst of metacarpal.
Dr. Gaurav B Mate, Department of Orthopaedics, B. J. Government Medical College, Pune, Maharashtra, India. E-mail: Gaurav.b.mate@gmail.com
Abstract
Introduction: A benign cystic lesion, the simple bone cyst (unicameral/essential bone cyst), it may be found in any long bone (most commonly found in femur and proximal humerus), usually in immature skeletal persons. Metacarpal simple bone cyst is an exceedingly rare occurrence and few treatment options have been described for the same.
Case Report: A 42-year-old manual laborer male (right hand dominant) came with history of trivial trauma to right hand thumb with hammer. He complained of mild swelling and pain since trauma. On imaging the right hand, an expansive lytic lesion was seen in the metaphyseo-diahyseal region of the first metacarpal. There was thinning of the cortex with break in cortex visible at mid diaphyseal region. There was absence of any soft-tissue involvement or periosteal reaction. Magnetic resonance imaging reported a T2 hyperintense and T1 isointense benign osteolytic lesion with pathological fracture. On aspiration, a reddish tinged fluid was found. A closed fixation was performed with the help of an intramedullary k-wire.
Conclusion: Simple bone cyst, although rare in metacarpal bone, is an important differential diagnosis in cases with cystic lesion. Simple bone cyst, although a benign lesion, can cause extensive involvement of the metacarpal bones and destroy the entire diaphysis. It requires adequate treatment which is simple and effective.
Keywords: Simple bone cyst, K-wire, metacarpal.
Simple bone cyst is a benign cystic lesion found commonly in skeletally immature patients in the metadiaphyseal region [1,2]. Most common to the femur and humerus, hand is an extremely rare area for cysts to be present. So far, only a few reports have described unicameral bone cysts (UBCs) of the phalanges, metacarpals, and carpals. Treatments have mainly consisted of curettage and bone grafting with fixation as required [2,3,4,5,6,7].
A 42-year-old manual laborer male (right hand dominant) gave history of trivial trauma to right hand thumb with hammer 2 days before presentation. He complained of mild swelling and pain since trauma. The pain was constant dull aching in nature and with mild swelling. The patient did not have any complaints of the part before the injury. There was no history of previous trauma or infection of the said area previously. His family and personal history were insignificant. On examination, there was minimal swelling of the dorsum of thenar side with no redness or rise in temperature locally. The patient had moderate tenderness and was able to do movement of the area with difficult. No sensorimotor or vascular deficit was found distally and no obvious deformity was visible.
On imaging the right hand (Fig. 1), an expansive lytic lesion was seen involving the entire metaphyseo-diahyseal region of the first metacarpal. There was thinning of the cortex with break in cortex continuity visible at mid diaphyseal region. There was absence of any soft-tissue involvement or periosteal reaction. Proximal and distal joints were normal and rest all the bones appeared to be normal. Magnetic resonance imaging (MRI) was performed with T1, T2, and short tau inversion recovery (STIR) imaging in multiple planes (Fig. 2, 3). It showed a T2/STIR hyperintense and T1 isointense benign osteolytic lesion involving entire of the 1st metacarpal with incomplete cortical fractures involving the shaft. The periosteum, surrounding soft tissue, and articular surfaces were normal. With the above report in mind, we went for a biopsy of the lesion. On aspiration, a reddish tinged fluid was found. All routine blood investigations including coagulation profile were normal. A closed fixation was performed with the help of an intramedullary k-wire (Fig. 4). The patient had minimal discomfort post-operative and a 2-week follow-up radiograph of the patient showed a well healing lesion (Fig. 5). K-wires were removed at 3 weeks and a 4 weeks follow-up X-ray (Fig. 6) showed a healing fracture with good amount of callus formation, decrease in soft-tissue swelling and intramedullary calcification. The patient was able to mobilize his thumb with almost no pain. There were no signs of infection and the k-wire wounds healed well.
an expansive lytic lesion was seen involving the entire metaphyseo-diahyseal region of the first metacarpal. There was thinning of the cortex with break in cortex continuity visible at mid diaphyseal region. There was absence of any soft-tissue involvement or periosteal reaction. Proximal and distal joints were normal and rest all the bones appeared to be normal. Magnetic resonance imaging (MRI) was performed with T1, T2, and short tau inversion recovery (STIR) imaging in multiple planes (Fig. 2, 3). It showed a T2/STIR hyperintense and T1 isointense benign osteolytic lesion involving entire of the 1st metacarpal with incomplete cortical fractures involving the shaft. The periosteum, surrounding soft tissue, and articular surfaces were normal. With the above report in mind, we went for a biopsy of the lesion. On aspiration, a reddish tinged fluid was found. All routine blood investigations including coagulation profile were normal. A closed fixation was performed with the help of an intramedullary k-wire (Fig. 4). The patient had minimal discomfort post-operative and a 2-week follow-up radiograph of the patient showed a well healing lesion (Fig. 5). K-wires were removed at 3 weeks and a 4 weeks follow-up X-ray (Fig. 6) showed a healing fracture with good amount of callus formation, decrease in soft-tissue swelling and intramedullary calcification. The patient was able to mobilize his thumb with almost no pain. There were no signs of infection and the k-wire wounds healed well.
Differential diagnosis of a benign osteolytic lesion of hand in a skeletally mature male is as follows [8,9,10,11,12,13]:
• Enchondroma
Benign cartilage forming lesions of the hand, present as lytic lesion in metadiaphysis, well circumscribed, histologically show cartilage cells
• Aneurysmal bone cyst
An expansile eccentric lesion with multiple air fluid levels (on MRI) with blood filled cavities
• UBC [14,15]
Expansile lesion in metadiaphyseal region. Single cavity and X-rays show single cavity with classical “fallen leaf” appearance in some cases with fracture
• Chondroblastoma (exceedingly rare)
• Chondromyxoid fibroma (exceedingly rare)
• Giant cell reparative granuloma
• Intraosseous ganglion cyst
Benign expansile lesion, histologically contains myxoid material. From the above based on MRI and aspiration findings, our diagnosis pointed toward either a UBC or an aneurysmal bone cyst. This was associated with a pathological fracture. Various modes of treatment have been considered for a UBC such as intralesional steroid injection, curettage, and bone grafting and intramedullary nailing [16,17]. However, cyst recurrence is a problem common to all treatment methods. UBCs have been proposed to occur as a result of trauma, intraosseous synovial cyst, and venous occlusion leading to raised intramedullary pressures. We broke the septae intraoperatively and fixation was done by a Kirschner wire appropriately. The patient had minimal pain postoperatively and was able to go home immediately on the next day. Fifteen days follow-up is awaited.
The end result at 4 weeks follow-up was a well healing calcification of the pathological fracture of UBC in the 1st metacarpal. The patient had almost no pain and was able to do active movements of his thumb easily. There were no signs of risk of infection or further progress of the bone cyst. Soft-tissue edema had subsided and bone girth had almost returned to normal.
Simple bone cysts, although extremely rare in the hand bones, need to be considered as a differential in such cases and treated appropriately.
UBCs of the hand bones can be a challenging diagnosis and difficult to treat considering the size of bones and the surrounding tissues. K-wire fixation offers an easy and effective technique for the same. However, further studies into this area can boost better and faster diagnosis and treatment.
References
- 1.Wilkins RM. Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-24. [Google Scholar | PubMed]
- 2.Diaz VA, Vernon SE, Ouellette EA. Pain and deformity of the index finger in a 41-year-old woman. Clin Orthop Relat Res 2009;467:1387-91. [Google Scholar | PubMed]
- 3.Head SA. Unicameral bone cyst located in metacarpal bone: Report of a case. J Am Osteopath Assoc 1984;84:372-3. [Google Scholar | PubMed]
- 4.Baruch A, Haas A, Lifschitz-Mercer B, Zeligowsky A. Simple bone cyst of the metacarpal. J Hand Surg Am 1987;12:1103-6. [Google Scholar | PubMed]
- 5.Ewald FC. Bone cyst in a phalanx of a two-and-a-half- year-old child: Case report and discussion. J Bone Joint Surg Am 1972;54:399-401. [Google Scholar | PubMed]
- 6.Jasan M, House JH, Brand JC. Bilateral unicameral bone cysts in the hamate bones. J Hand Surg Am 1990;15:888-90. [Google Scholar | PubMed]
- 7.Unicameral bone cyst of the lunate in an adult: Case report. J Orthop Surg Res 2010;5:79. [Google Scholar | PubMed]
- 8.Tham S, Ireland DC. Intraosseous ganglion cyst of the lunate: Diagnosis and management. J Hand Surg Br 1992;17:429-32. [Google Scholar | PubMed]
- 9.Weiner SD. Enchondroma and chondrosarcoma of bone: Clinical, radiologic, and histologic differentiation. Instr Course Lect 2004;53:645-9. [Google Scholar | PubMed]
- 10.Ratner V, Dorfman HD. Giant-cell reparative granuloma of the hand and foot bones. Clin Orthop Relat Res 1990;260:251-8. [Google Scholar | PubMed]
- 11.Adler CP. Multifocal osteoblastoma of the hand. Skeletal Radiol 2000;29:601-4. [Google Scholar | PubMed]
- 12.Mahnken AH, Nolte-Ernsting CC, Wildberger JE, Heussen N, Adam G, Wirtz DC, et al. Aneurysmal bone cyst: Value of MR imaging and conventional radiography. Eur Radiol 2003;13:1118-24. [Google Scholar | PubMed]
- 13.Reynolds J. The ‘‘fallen fragment sign’’ in the diagnosis of unicameral bone cysts. Radiology 1969;92:949-53. [Google Scholar | PubMed]
- 14.McVey MJ, Kettner NW. Pathologic fracture of metacarpal enchondroma: Case study and differential diagnosis. J Manipulative Physiol Ther 2002;25:340-4. [Google Scholar | PubMed]
- 15.Shimal A, Wee B, Nicklaus-Wollenteit IU, Sumathi V, Davies AM, James SL. Subperiosteal aneurysmal bone cyst of the metacarpal. Eur J Radiol 2009;71:117-9. [Google Scholar | PubMed]
- 16.Roposch A, Saraph V, Linhart WE. Flexible intramedullary nailing for the treatment of unicameral bone cysts in long bones. J Bone Joint Surg Am 2000;82:1447-53. [Google Scholar | PubMed]
- 17.Patwardhan S, Shah K, Shyam A, Sancheti P. Simple bone cyst of metacarpal: Rare lesion with unique treatment. J Orthop Case Rep 2014;4:63-5. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 September 29, 2019 Bimalleolar Fracture: A Unique Case of Complication of Complex Regional Pain Syndrome of Lower Extremity After Prolonged Undue Immobilisation
September 29, 2019 Bimalleolar Fracture: A Unique Case of Complication of Complex Regional Pain Syndrome of Lower Extremity After Prolonged Undue Immobilisation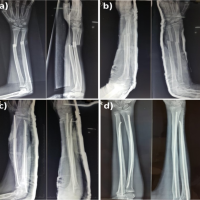 May 10, 2024 Pediatric Forearm Fractures: Investigating the Functional Outcomes of Titanium Elastic Nailing for Unstable Both-Bone Fractures
May 10, 2024 Pediatric Forearm Fractures: Investigating the Functional Outcomes of Titanium Elastic Nailing for Unstable Both-Bone Fractures April 7, 2014 Fibrous Dysplasia of the Spine – A Case Involving Three Levels of Thoracic Spine
April 7, 2014 Fibrous Dysplasia of the Spine – A Case Involving Three Levels of Thoracic Spine November 27, 2020 Synovial Non-langerhans Cell Histiocytosis of the Shoulder: A Case Report and Review of the Literature
November 27, 2020 Synovial Non-langerhans Cell Histiocytosis of the Shoulder: A Case Report and Review of the Literature